The details of the Omicron variant are becoming clearer, and they are encouraging.
They’re not entirely encouraging, and I will get into some detail about one of the biggest problems — the stress on hospitals, which are facing huge numbers of moderately ill Covid-19 patients. But regular readers of this newsletter know that I try to avoid the bad-news bias that often infects journalism. (We journalists tend to be comfortable delivering bad news straight up but uncomfortable reporting good news without extensive caveats.)
So I want to be clear: The latest evidence about Covid is largely positive. A few weeks ago, many experts and journalists were warning that the initial evidence from South Africa — suggesting that Omicron was milder than other variants — might turn out to be a mirage. It has turned out to be real.
There are at least three main ways that Omicron looks substantially milder than other versions of the virus:
1. Less hospitalization
Somebody infected with Omicron is less likely to need hospital treatment than somebody infected with an earlier version of Covid.
An analysis of patients in Houston, for example, found that Omicron patients were only about one-third as likely to need hospitalization as Delta patients. In Britain, people with Omicron were about half as likely to require hospital care, the government reported. The pattern looks similar in Canada, Emily and Azeen note.
Hospitalizations are nonetheless rising in the U.S., because Omicron is so contagious that it has led to an explosion of cases. Many hospitals are running short of beds and staff, partly because of Covid-related absences. In Maryland, more people are hospitalized with Covid than ever.
“Thankfully the Covid patients aren’t as sick. But there’s so many of them,” Craig Spencer, an emergency room doctor in New York, tweeted on Monday, after a long shift. “The next few weeks will be really, really tough for us.”
The biggest potential problem is that overwhelmed hospitals will not be able to provide patients — whether they have Covid or other conditions — with straightforward but needed care. Some may die as a result. That possibility explains why many epidemiologists still urge people to take measures to reduce Covid’s spread during the Omicron surge. It’s likely to last at least a couple more weeks in the U.S.
2. Milder hospitalization
Omicron is not just less likely to send somebody to the hospital. Even among people who need hospital care, symptoms are milder on average than among people who were hospitalized in previous waves.
A crucial reason appears to be that Omicron does not attack the lungs as earlier versions of Covid did. Omicron instead tends to be focused in the nose and throat, causing fewer patients to have breathing problems or need a ventilator.
As Dr. Rahul Sharma of NewYork-Presbyterian/Weill Cornell told The Times, “We’re not sending as many patients to the I.C.U., we’re not intubating as many patients, and actually, most of our patients that are coming to the emergency department that do test positive are actually being discharged.”
In London, the number of patients on ventilators has remained roughly constant in recent weeks, even as the number of cases has soared, John Burn-Murdoch of The Financial Times noted.
3. And deaths?
In the U.S., mortality trends typically trail case trends by about three weeks — which means the Omicron surge, which began more than a month ago, should be visible in the death counts. It isn’t yet:
Data as of Jan. 3.Source: New York Times database
Covid deaths will still probably rise in the U.S. in coming days or weeks, many experts say. For one thing, data can be delayed around major holidays. For another, millions of adults remain unvaccinated and vulnerable.
But the increase in deaths is unlikely to be anywhere near as large as the increase last summer, during the Delta wave. Look at the data from South Africa, where the Omicron wave is already receding:
South Africa reported identification of Omicron on Nov. 24.Source: Johns Hopkins University
The bottom line
Given the combination of surging cases and milder disease, how should people respond?
Dr. Leana Wen, Baltimore’s former health commissioner, wrote a helpful Washington Post article in which she urged a middle path between reinstituting lockdowns and allowing Omicron to spread unchecked.
“It’s unreasonable to ask vaccinated people to refrain from pre-pandemic activities,” Wen said. “After all, the individual risk to them is low, and there is a steep price to keeping students out of school, shuttering restaurants and retail shops and stopping travel and commerce.”
But she urged people to get booster shots, recommended that they wear KN95 or N95 masks and encouraged governments and businesses to mandate vaccination. All of those measures can reduce the spread of Covid and, by extension, hospital crowding and death.
Different people will make different decisions, and that’s OK. Severely immunocompromised people — like those who have received organ transplants or are actively receiving cancer treatment — have reason to be extra cautious. For otherwise healthy older people, on the other hand, the latest data may be encouraging enough to affect their behavior.
Consider this: Before Omicron, a typical vaccinated 75-year-old who contracted Covid had a roughly similar risk of death — around 1 in 200 — as a typical 75-year-old who contracted the flu. (Here are the details behind that calculation, which is based on an academic study.)
Omicron has changed the calculation. Because it is milder than earlier versions of the virus, Covid now appears to present less threat to most vaccinated elderly people than the annual flu does.
The flu, of course, does present risk for the elderly. And the sheer size of the Omicron surge may argue for caution over the next few weeks. But the combination of vaccines and Omicron’s apparent mildness means that, for an individual, Covid increasingly resembles the kind of health risk that people accept every day.
Even as daily new COVID cases set all-time records and hospitals fill up, epidemiologists have arrived at a perhaps surprising consensus. Yes, the latest Omicron variant of the novel coronavirus is bad. But it could have been a lot worse.
Even as cases have surged, deaths haven’t—at least not to the same degree. Omicron is highly transmissible but generally not as severe as some older variants—“lineages” is the scientific term.
We got lucky. But that luck might not hold. Many of the same epidemiologists who have breathed a sigh of relief over Omicron’s relatively low death rate are anticipating that the next lineage might be much worse.
Fretting over a possible future lineage that combines Omicron’s extreme transmissibility with the severity of, say, the previous Delta lineage, experts are beginning to embrace a new public health strategy that’s getting an early test run in Israel: a four-shot regimen of messenger-RNA vaccine.
“I think this will be the strategy going forward,” Edwin Michael, an epidemiologist at the Center for Global Health Infectious Disease Research at the University of South Florida, told The Daily Beast.
Omicron raised alarms in health agencies all over the world in late November after officials in South Africa reported the first cases. Compared to older lineages, Omicron features around 50 key mutations, some 30 of which are on the spike protein that helps the virus to grab onto our cells.
Some of the mutations are associated with a virus’s ability to dodge antibodies and thus partially evade vaccines. Others are associated with higher transmissibility. The lineage’s genetic makeup pointed to a huge spike in infections in the unvaccinated as well as an increase in milder “breakthrough” infections in the vaccinated.
That’s exactly what happened. Health officials registered more than 10 million new COVID cases the first week of January. That’s nearly double the previous worst week for new infections, back in May. Around 3 million of those infections were in the United States, where Omicron coincided with the Thanksgiving, Christmas, and New Year holidays and associated traveling and family gatherings.
But mercifully, deaths haven’t increased as much as cases have. Worldwide, there were 43,000 COVID deaths the first week of January—fewer than 10,000 of them in the U.S. While deaths tend to lag infections by a couple weeks, Omicron has been dominant long enough that it’s increasingly evident there’s been what statisticians call a “decoupling” of cases and fatalities.
“We can say we dodged a bullet in that Omicron does not appear to cause as serious of a disease,” Stephanie James, the head of a COVID testing lab at Regis University in Colorado, told The Daily Beast. She stressed that data is still being gathered, so we can’t be certain yet that the apparent decoupling is real.
Assuming the decoupling is happening, experts attribute it to two factors. First, Omicron tends to infect the throat without necessarily descending to the lungs, where the potential for lasting or fatal damage is much, much higher. Second, by now, countries have administered nearly 9.3 billion doses of vaccine—enough for a majority of the world’s population to have received at least one dose.
In the United States, 73 percent of people have gotten at least one dose. Sixty-two percent have gotten two doses of the best mRNA vaccines. A third have received a booster dose.
Yes, Omicron has some ability to evade antibodies, meaning the vaccines are somewhat less effective against this lineage than they are against Delta and other older lineages. But even when a vaccine doesn’t prevent an infection, it usually greatly reduces its severity.
For many vaccinated people who’ve caught Omicron, the resulting COVID infection is mild. “A common cold or some sniffles in a fully vaxxed and boosted healthy individual,” is how Eric Bortz, a University of Alaska-Anchorage virologist and public health expert, described it to The Daily Beast.
All that is to say, Omicron could have been a lot worse. Viruses evolve to survive. That can mean greater transmissibility, antibody-evasion or more serious infection. Omicron mutated for the former two. There’s a chance some future Sigma or Upsilon lineage could do all three.
When it comes to viral mutations, “extreme events can occur at a non-negligible rate, or probability, and can lead to large consequences,” Michael said. Imagine a lineage that’s as transmissible as Omicron but also attacks the lungs like Delta tends to do. Now imagine that this hypothetical lineage is even more adept than Omicron at evading the vaccines.
That would be the nightmare lineage. And it’s entirely conceivable it’s in our future. There are enough vaccine holdouts, such as the roughly 50 million Americans who say they’ll never get jabbed, that the SARS-CoV-2 pathogen should have ample opportunities for mutation.
“As long as we have unvaccinated people in this country—and across the globe—there is the potential for new and possibly more concerning viral variants to arise,” Aimee Bernard, a University of Colorado immunologist, told The Daily Beast.
Worse, this ongoing viral evolution is happening against a backdrop of waning immunity. Antibodies, whether vaccine-induced or naturally occurring from past infection, fade over time. It’s not for no reason that health agencies in many countries urge booster doses just three months after initial vaccination. The U.S. Centers for Disease Control and Prevention is an outlier, and recommends people get boosted after five months.
A lineage much worse than Omicron could evolve at the same time that antibodies wane in billions of people all over the world. That’s why many experts believe the COVID vaccines will end up being annual or even semi-annual jabs. You’ll need a fourth jab, a fifth jab, a sixth jab, et cetera, forever.
Israel, a world leader in global health, is already turning that expectation into policy. Citing multiple studies that showed a big boost in antibodies with an additional dose of mRNA and no safety concerns, the country’s health ministry this week began offering a fourth dose to anyone over the age of 60, who tend to be more vulnerable to COVID than younger people.
That should be the standard everywhere, Ali Mokdad, a professor of health metrics sciences at the University of Washington Institute for Health, told The Daily Beast. “Scientifically, they’re right,” he said of the Israeli health officials.
If there’s a downside, it’s that there are still a few poorer countries—in Africa, mostly—where many people still struggle to get access to any vaccine, let alone boosters and fourth doses. If and when other richer countries follow Israel’s lead and begin offering additional jabs, there’s some risk of even greater inequity in global vaccine distribution.
“The downside is for the rest of the world,” Mokdad said. “I’m waiting to get my first dose and you guys are getting a fourth?”
The solution isn’t to deprive people of the doses they need to maintain their protection against future—and potentially more dangerous—lineages. The solution, for vaccine-producing countries, is to further boost production and double down on efforts to push vaccines out to the least privileged communities.
A sense of urgency is key. For all its rapid spread, Omicron has actually gone fairly easy on us. Sigma or Upsilon might not.
Over the past two years, historians and analysts have compared the coronavirus to the 1918 flu pandemic. Many of the mitigation practices used to combat the spread of the coronavirus, especially before the development of the vaccines, have been the same as those used in 1918 and 1919 — masks and hygiene, social distancing, ventilation, limits on gatherings (particularly indoors), quarantines, mandates, closure policies and more.
Yet, it may be that only now, in the winter of 2022, when Americans are exhausted with these mitigation methods, that a comparison to the 1918 pandemic is most apt.
The highly contagious omicron variant has rendered vaccines much less effective at preventing infections, thus producing skyrocketing caseloads. And that creates a direct parallel with the fall of 1918, which provides lessons for making January as painless as possible.
In February and March 1918, an infectious flu emerged. It spread from Kansas, through World War I troop and material transports, filling military post hospitals and traveling across the Atlantic and around the world within six months. Cramped quarters and wartime transport and industry generated optimal conditions for the flu to spread, and so, too, did the worldwide nature of commerce and connection. But there was a silver lining: Mortality rates were very low.
In part because of press censorship of anything that might undermine the war effort, many dismissed the flu as a “three-day fever,” perhaps merely a heavy cold, or simply another case of the grippe (an old-fashioned word for the flu).
Downplaying the flu led to high infection rates, which increased the odds of mutations. And in the summer of 1918, a more infectious variant emerged. In August and September, U.S. and British intelligence officers observed outbreaks in Switzerland and northern Europe, writing home with warnings that went largely unheeded.
Unsurprisingly then, this seemingly more infectious, much more deadly variant of H1N1 traveled west across the Atlantic, producing the worst period of the pandemic in October 1918. Nearly 200,000 Americans died that month. After a superspreading Liberty Loan parade at the end of September, Philadelphia became an epicenter of the outbreak. At its peak, nearly 700 Philadelphians died per day.
Once spread had begun, mitigation methods such as closures, distancing, mask-wearing and isolating those infected couldn’t stop it, but they did save many lives and limited suffering by slowing infections and spread. The places that fared best implemented proactive restrictions early; they kept them in place until infections and hospitalizations were way down, then opened up gradually, with preparations to reimpose measures if spread returned or rates elevated, often ignoring the pleas of special interests lobbying hard for a complete reopening.
In places in the United States where officials gave in to public fatigue and lobbying to remove mitigation methods, winter surges struck. Although down from October’s highs, these surges were still usually far worse than those in the cities and regions that held steady.
In Denver, in late November 1918, an “amusement” lobby — businesses and leaders invested in keeping theaters, movie houses, pool halls and other public venues open — successfully pressured the mayor and public health officials to rescind and then revise a closure order. This, in turn, generated what the Rocky Mountain News called “almost indescribable confusion,” followed by widespread public defiance of mask and other public health prescriptions.
In San Francisco, where resistance was generally less successful than in Denver, there was significant buy-in for a second round of masking and public health mandates in early 1919 during a new surge. But opposition created an issue. An Anti-Mask League formed, and public defiance became more pronounced. Eventually anti-maskers and an improving epidemic situation combined to end the “masked” city’s second round of mask and public health mandates.
The takeaway: Fatigue and removing mitigation methods made things worse. Public officials needed to safeguard the public good, even if that meant unpopular moves.
The flu burned through vulnerable populations, but by late winter and early spring 1919, deaths and infections dropped rapidly, shifting toward an endemic moment — the flu would remain present, but less deadly and dangerous.
Overall, nearly 675,000 Americans died during the 1918-19 flu pandemic, the majority during the second wave in the autumn of 1918. That was 1 in roughly 152 Americans (with a case fatality rate of about 2.5 percent). Worldwide estimates differ, but on the order of 50 million probably died in the flu pandemic.
In 2022, we have far greater biomedical and technological capacity enabling us to sequence mutations, understand the physics of aerosolization and develop vaccines at a rapid pace. We also have a far greater public health infrastructure than existed in 1918 and 1919. Even so, it remains incredibly hard to stop infectious diseases, particularly those transmitted by air. This is complicated further because many of those infected with the coronavirus are asymptomatic. And our world is even more interconnected than in 1918.
That is why, given the contagiousness of omicron, the lessons of the past are even more important today than they were a year ago. The new surge threatens to overwhelm our public health infrastructure, which is struggling after almost two years of fighting the pandemic. Hospitals are experiencing staff shortages (like in fall 1918). Testing remains problematic.
And ominously, as in the fall of 1918, Americans fatigued by restrictions and a seemingly endless pandemic are increasingly balking at following the guidance of public health professionals or questioning why their edicts have changed from earlier in the pandemic. They are taking actions that, at the very least, put more vulnerable people and the system as a whole at risk — often egged on by politicians and media figures downplaying the severity of the moment.
Public health officials also may be repeating the mistakes of the past. Conjuring echoes of Denver in late 1918, under pressure to prioritize keeping society open rather than focusing on limiting spread, the Centers for Disease Control and Prevention changed its isolation recommendations in late December. The new guidelines halved isolation time and do not require a negative test to reenter work or social gatherings.
Thankfully, we have an enormous advantage over 1918 that offers hope. Whereas efforts to develop a flu vaccine a century ago failed, the coronavirus vaccines developed in 2020 largely prevent severe illness or death from omicron, and the companies and researchers that produced them expect a booster shot tailored to omicron sometime in the winter or spring. So, too, we have antivirals and new treatments that are just becoming available, though in insufficient quantities for now.
Those lifesaving advantages, however, can only help as much as Americans embrace them. Only by getting vaccinated, including with booster shots, can Americans prevent the health-care system from being overwhelmed. But the vaccination rate in the country remains a relatively paltry 62 percent, and only a scant 1 in 5 have received a booster shot. And as in 1918, some of the choice rests with public officials. Though restrictions may not be popular, officials can reimpose them — offering public support where necessary to those for whom compliance would create hardship — and incentivize and mandate vaccines, taking advantage of our greater medical technology.
As the flu waned in 1919, one Portland, Ore., health official reflected that “the biggest thing we have had to fight in the influenza epidemic has been apathy, or perhaps the careless selfishness of the public.”
The same remains true today.
Vaccines, new treatments and century-old mitigation strategies such as masks, distancing and limits on gatherings give us a pathway to prevent the first six weeks of 2022 from being like the fall of 1918. And encouraging news about the severity of omicron provides real optimism that an endemic future — in which the coronavirus remains but poses far less of a threat — is near. The question is whether we get there with a maximum of pain or a minimum. The choice is ours.
Why are so many vaccinated people getting COVID-19 lately?
A couple of factors are at play, starting with the emergence of the highly contagious omicron variant. Omicron is more likely to infect people, even if it doesn’t make them very sick, and its surge coincided with the holiday travel season in many places.
People might mistakenly think the COVID-19 vaccines will completely block infection, but the shots are mainly designed to prevent severe illness, says Louis Mansky, a virus researcher at the University of Minnesota.
And the vaccines are still doing their job on that front, particularly for people who’ve gotten boosters.
Two doses of the Pfizer-BioNTech or Moderna vaccines or one dose of the Johnson & Johnson vaccine still offer strong protection against serious illness from omicron. While those initial doses aren’t very good at blocking omicron infection, boosters — particularly with the Pfizer and Moderna vaccines — rev up levels of the antibodies to help fend off infection.
Omicron appears to replicate much more efficiently than previous variants. And if infected people have high virus loads, there’s a greater likelihood they’ll pass it on to others, especially the unvaccinated. Vaccinated people who get the virus are more likely to have mild symptoms, if any, since the shots trigger multiple defenses in your immune system, making it much more difficult for omicron to slip past them all.
Advice for staying safe hasn’t changed. Doctors say to wear masks indoors, avoid crowds and get vaccinated and boosted. Even though the shots won’t always keep you from catching the virus, they’ll make it much more likely you stay alive and out of the hospital.
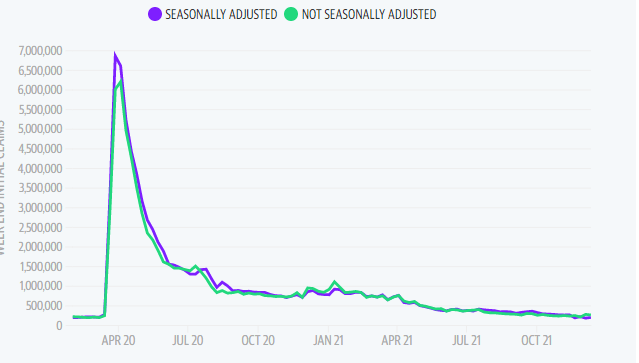
First-time unemployment filings fell by 8,000 claims from the previous week’s reading, marking the second lowest print during the pandemic and signaling continued recovery in the labor market as high demand for workers pours into the new year.
The Labor Department released its latest report on initial and continuing claims on Thursday at 8:30 a.m. ET. Here were the main metrics from the print, compared to consensus estimates compiled by Bloomberg:
Initial jobless claims, week ended Dec. 25: 198,000 vs. 206,000 expected and upwardly revised to 206,000 during prior week
Continuing claims, week ended Dec. 18: 1.716 million vs. 1.875 million expected and downwardly revised to 1.856 million during prior week
The newest print brings the four-week moving average to 199,300 in the week ending Dec. 25, Bloomberg data reflected. Continuing claims dropped to a fresh pandemic low of 1.716 million. Forecast for this week’s jobless claims release ranged from 190,000-225,000 from 22 economists surveyed by Bloomberg.
First-time filings for unemployment remained below the 2019 average of 218,000, when the unemployment rate was at a half-century low of 3.5%, according to Bloomberg. The current unemployment rate is also expected to edge down to 4.1% in December as the labor market continues to tighten.
At 205,000, last week’s initial unemployment claims were on par with economist forecasts and below pre-pandemic levels yet again. Earlier in December, jobless claims fell sharply to 188,000, the lowest level since 1969. The prints serve an early indication of the relative strength expected to show in December’s jobs report, though the economic impact of the virus remains unclear.
“Fortunately, there’s no evidence in this data of a new wave of fresh job loss,” Bankrate senior economic analyst Mark Hamrick said, commenting on last week’s figures. “New claims are only slightly above the lowest point in decades notched a couple of weeks ago.”
“With so much uncertainty now and the high level of concern about the Omicron variant, we’ll take stability when we can get it,” Hamrick added.
“It’s stunning to see how much the rate has fallen in the last five months,” he told Yahoo Finance Live. “We expect that pace of decline to slow, but it doesn’t take much to get below 4%, even with a tick up in the labor participation rate, which has been depressed over the last year and a half.”
Record cases of COVID-19 may discourage workers from looking for work as U.S. households continue to cite fear of COVID or virus-related caretaking needs as reasons for staying out of the job market.
“The pandemic’s resurgence is affecting the economy,” Hamrick said in a note last week. “The question is for how long and how much, and it is too early to know the answers.”
At the 390-bed Terrace View nursing home on the east side of Buffalo, 22 beds are shut down. There isn’t enough staff to care for a full house, safely or legally.
That means some fully recovered patients in the adjacent Erie County Medical Center must stay in their hospital rooms, waiting for a bed in the nursing home. Which means some patients in the emergency department, who should be admitted to the hospital, must stay there until a hospital bed opens up. The emergency department becomes stretched so thin that 10 to 20 percent of arrivals leave without seeing a caregiver — after an average wait of six to eight hours, according to the hospital’s data.
“We used to get upset when our ‘left without being seen’ went above 3 percent,” said Thomas Quatroche, president and chief executive of the Erie County Medical Center Corp., which runs the 590-bed public safety net hospital.
Nursing home bed and staff shortages were problems in the United States before the coronavirus pandemic. But the departure of 425,000 employees over the past two years has narrowed the bottleneck at nursing homes and other long-term care facilities at the same time that acute care hospitals are facing unending demand for services due to a persistent pandemic and staff shortages of their own.
With the omicron variant raising fears of even more hospitalizations, the problems faced by nursing homes are taking on even more importance. Several states have sent National Guard members to help with caregiving and other chores.
Hospitalizations, which peaked at higher than 142,000 in January, are rising again as well, reaching more than 71,000 nationally on Thursday, according to data tracked by The Washington Post. In some places, there is little room left in hospitals or ICUs.
About 58 percent of the nation’s 14,000 nursing homes are limiting admissions, according to a voluntary survey conducted by the American Health Care Association, which represents them. According to the U.S. Bureau of Labor Statistics, 425,000 employees, many of them low-paid certified nursing assistants who are the backbone of the nursing home workforce, have left since February 2020.
“What we’re seeing on the hospital side is a reflection of that,” said Rob Shipp, vice president for population health and clinical affairs at the Hospital Association of Pennsylvania, which represents medical providers in that state. The backups are not just for traditional medical inpatients ready for follow-up care, he said, but psychiatric and other patients as well.
A handful of developmentally disabled patients at Erie County Medical Center waited as long as a year for placement in a group setting, Quatroche said. Medical patients recovered from illness and surgery who cannot go home safely may wait days or weeks for a bed, he said.
“I don’t know if everyone understands how serious the situation is,” Quatroche said. “You really don’t know until you need care. And then you know immediately.”
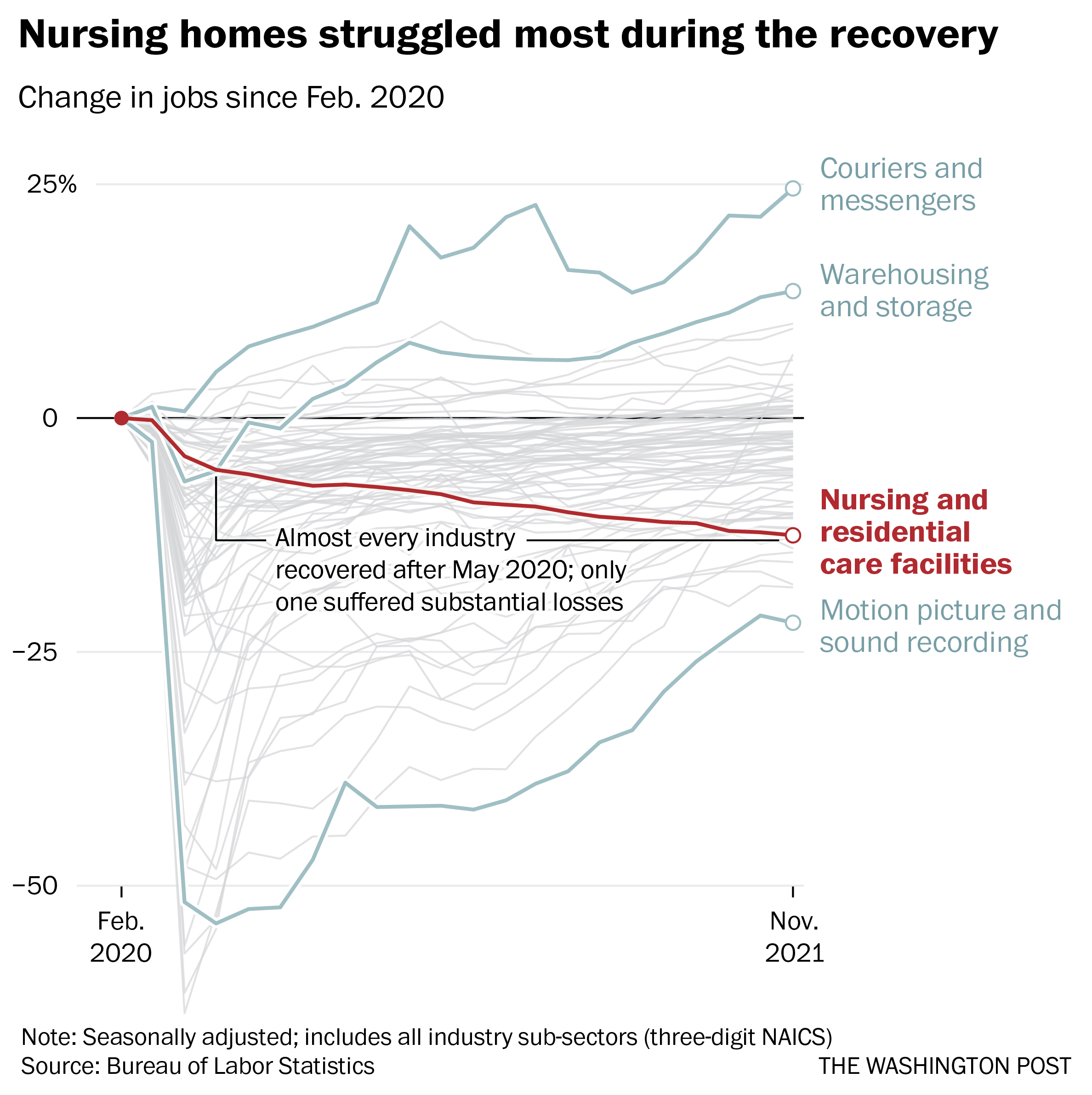
Nearly 237,000 workers left during the recovery, data through November show. No other industry suffered anything close to those losses over the same period, according to the Bureau of Labor Statistics.
Workers in the broader health-care industry have been quitting in record numbers for most of the pandemic, plagued by burnout, vulnerability to the coronavirus and poaching by competitors. Low-wage workers tend to quit at the highest rates, Labor Department data show, and nursing home workers are the lowest paid in the health sector, with nonmanagerial earnings averaging between $17.45 an hour for assisted living to $21.19 an hour for skilled nursing facilities, according to the BLS.
Nursing home occupancy fell sharply at the start of the pandemic, but inched back upward in 2021, according to the nonprofit National Investment Center for Seniors Housing and Care. One major force that held it back was worker shortages.
“Operators in the business have said we could admit more patients, but we cannot find the staff to allow that to happen,” said Bill Kauffman, senior principal at the organization.
Shortages have spawned fierce talent wars in the industry, Brookdale Senior Living Chief Executive Officer Cindy Baier said in a recent earnings call. When they don’t have enough workers, restaurants can reduce service hours and hospitals can cut elective surgeries, but nursing homes don’t have the option of eliminating critical services, she said. They must close beds.
“We are in the ‘people taking care of people’ business around-the-clock, 365 days a year,” she said.
Nursing homes tend to gain workers during a recession but can struggle to hire during expansions, according to an analysis of county-level data from the Great Recession recently published in the health care provision and financing journal Inquiry.
Steady income from their resident population and government programs such as Medicaid makes them recession-proof, and their low pay and challenging work conditions mean they’re chronically understaffed, said one of the study’s authors, Indiana University health-care economist Kosali Simon.
When recessions occur, nursing homes go on a hiring spree, filling holes in their staff with qualified workers laid off elsewhere.
“People during a recession may lose their construction jobs or jobs in retail sectors, and then look for entry-level positions at places like nursing homes where there is always demand,” Simon said.
Now, amid the “Great Resignation” and the hot job market, the opposite is happening. In sparsely populated areas and regions where pay is lower, the problem is even worse.
The Diakonos Group, which operates 26 nursing homes, assisted-living facilities and group homes in Oklahoma, closed an 84-bed location for seniors with mental health needs in May “simply because we couldn’t staff it any longer,” said Chief Executive Officer Scott Pilgrim. Patients were transferred elsewhere, including Tulsa and Oklahoma City, he said.
The home in rural Medford, which depended entirely on Medicaid payments, “was never easy to staff, but once we started through covid and everything, our staff was just burned out.”
Diakonos boosted certified nursing assistants’ pay from $12 an hour and licensed practical nurses’ pay from $20 an hour, used federal and state assistance to offer bonuses and employed overtime, but workers kept leaving for better health-care jobs and positions in other industries, he said.
“I’ve never been able to pay what we ought to pay,” Pilgrim said. Eventually he began to limit admissions and eventually was forced to close.
“The hospitals are backed up,” he said. “They’re trying to find anywhere to send people. We get referrals from states all around us. The hospitals are desperate to find places to send people.”
In south central Pennsylvania, SpiriTrust Lutheran is not filling 61 of its 344 beds in six facilities because of the worker shortage, said Carol Hess, the company’s senior vice president.
“I have nurses who went to become real estate agents,” she said. “They were just burned out.”
Pay raises of $1 to $1.50 an hour and bonuses brought the lowest-paid workers to about $15 an hour, Hess said, and the company is planning a recruiting drive after Jan. 1. But the prognosis is still grim.
“We’re competing with restaurants for our dining team members,” Hess said. “We’re competing with other folks for cleaning and laundry and others.” In the area around Harrisburg where SpiriTrust employees live, some schools that turned out certified nurse assistants closed during the pandemic and haven’t reopened.
The nursing homes have begun borrowing licensed practical nurses from WellSpan Health, the nearby hospital system that discharges many of its patients to SpriTrust after they recover. About 15 have began their orientations this month, she said, and the two systems are collaborating to pay them.
The bed shortage is causing backups that can average several days in the hospital, said Michael Seim, the hospital system’s chief quality officer. That gives the hospitals an interest in helping any way they can, he said.
“We have between 80 and 100 patients waiting for some type of skilled care,” Seim said this month. The hospital has begun caring for more people at home, enrolling 400 people so far in a program that sends clinicians to check on them there. More than 90 percent have said they are happy with the program.
“I think the future of hospital-based care is partnerships,” Seim said. “It’s going to be health systems partnering across their service areas … to disrupt the model we have.”
Healthy individuals who have been vaccinated, and especially those who have been boosted, appear unlikely to develop severe infections from the omicron variant that would land them in the hospital, say medical experts who have monitored the effects of the newest coronavirus variant since it was identified over four weeks ago.
While omicron has sent U.S. infections soaring to levels not seen since last winter’s wave, it appears to have less severe effects than the delta variant, according to a handful of international studies and early data from several U.S. hospitals.
Those infected by the omicron variant are 15 to 20 percent less likely to go to an emergency room, and 40 percent less likely to be hospitalized overnight, compared with those infected with delta, according to English data analyzed by scientists from Imperial College London. That aligns with early U.S. data from some hospitals.
At the Houston Methodist hospital system, about 15 percent of symptomatic individuals have ended up hospitalized — around a 70 percent reduction compared with those infected by the delta variant, said James Musser, chair of pathology and genomic medicine.
A separate study from Britain, which is not yet peer reviewed, found that people infected with omicron were almost 60 percent less likely to enter the hospital than those infected with delta.
“What is absolutely clear is there is lower rate of hospitalization with our omicron patients in our hospital system,” Musser said. “That does not necessarily mean that this variant is quote-unquote ‘less virulent.’ The jury’s still out on that. What we know now is that … if you are immunized and, more importantly, if you are boosted, you’re going to stay out of substantial trouble.”
He and other experts warn against complacency, however, cautioning that millions of Americans, particularly the unvaccinated, remain vulnerable to more serious disease from the most transmissible coronavirus variant to date.
Other factors that might lead to greater risk include an individual’s age, the type of vaccine or booster they received, and whether they have underlying health problems, such as heart disease or obesity, said Michael Osterholm, director of the Center for Infectious Disease Research and Policy at the University of Minnesota and a member of President Biden’s covid-19 transition task force.
“Have you previously had infection? Were you vaccinated? How many doses of vaccine, and was it more than six months ago? So in some ways this is almost like a calculus problem. It’s got a lot of moving parts to it and we’re trying to figure it out,” Osterholm said.
Doctors also caution that far more people will become infected with omicron simply because of its transmissibility. If even a small fraction of those land in the hospital, they worry that health care systems that are already short-staffed because of delta infections could be overwhelmed — with potentially dire results for those needing critical care as a result of car accidents, heart attacks, strokes, or any number of things that bring people to emergency rooms.
“We need to be respectful of the fact that our hospital system has been under this kind of duress for such a long time,” said Larry Corey, a virologist at the Fred Hutchinson Cancer Research Center in Seattle. “We need to do everything we can to not allow the situation, where there’s such crowding and such intensity that we can’t optimally take care of the people who get severe disease.”
Anthony S. Fauci, Biden’s chief medical adviser, said the rapid increase in the numbers of people getting infected with the omicron variant will invariably put additional strain on the system.
“We’re going to have a real challenge to the health-care delivery system — namely the number of beds, the number of ICU beds and even the number of health care providers,” Fauci said in an interview. “Even vaccinated people are getting breakthrough infections. So if you get enough nurses and doctors infected, they are going to temporarily be out of action. And if you get enough of them out of action, you could have a double stress on the health care system.”
The welcome news for most people who are vaccinated and boosted is that omicron infections often mimic the symptoms of the common cold. Those with two shots of vaccine, but no booster, also appear to fare relatively well, though they may develop more intense symptoms that may last longer, experts said.
In a series of Twitter posts, Craig Spencer, who teaches emergency medicine at Columbia University Medical Center, said every boosted patient he has seen in the emergency room has had no difficulty breathing or shortness of breath. Those who have had two doses of either the Pfizer or Moderna vaccines also have had mild symptoms, he said, “but more than those who had received a third dose.”
But almost every patient who had to be hospitalized was unvaccinated, he said.
“No matter your political affiliation, or thoughts on masks, or where you live in this country, as an ER doctor you’d trust with your life if you rolled into my emergency room at 3am, I promise you that you’d rather face the oncoming Omicron wave vaccinated,” Spencer wrote.
Children are also filling up hospital beds in many parts of the country, especially in New York. State officials issued a warning on Christmas Eve after a fourfold increase in hospitalizations in children under 18 in New York City between Dec. 5 and last week. About half of the admissions were children under 5, who are not eligible for vaccination, according to the New York Department of Health.
Experts cautioned that those at higher risk of severe infection to previous variants probably remain vulnerable to this one.
It’s not yet clear whether older, boosted individuals and those with underlying conditions, such as diabetes and heart disease, face the same lowered risk with omicron. Answering such questions is key to assessing the likely trajectory of the variant in the U.S. since it is older and less healthy than many of its global peers.
So far, though, early U.S. data echoes what has been seen in South Africa and Britain, where omicron waves are slightly ahead of this country’s.
A group of Scottish scientists said recently that vaccinated people appear to have some protection against symptomatic infection from omicron, although less than they did against delta. A third dose or booster of an mRNA vaccine was associated with a 57 percent reduction in the odds of developing a symptomatic omicron case.
In the Johns Hopkins Hospital emergency department, physicians are seeing more infections than atany other point in the pandemic, but most of the cases are not severe, said Stuart Ray, a professor of medicine in the division of infectious diseases. But he warned that there is not yet “reassuring evidence” the United States will be spared from a disruptive wave of infections and complications.
The country faces other challenges with omicron in terms of its medicine cabinet. Two of the three existing intravenous treatments called monoclonal antibodies — those from Regeneron and Eli Lilly — do not work against the variant. Some Republican governors had touted the ability of those with covid-19 to receive monoclonal antibodies, spurring some Americans to see those treatments as an alternative to getting vaccinated.
The only monoclonal antibody that does work, sotrovimab from Vir Biotechnology and GlaxoSmithKline, is in short supply and will not be available to many of those who become infected. The Food and Drug Administration authorized two easy-to-take antiviral pills last week and one has high efficacy against omicron, but it will be in initial short supply. Distribution of the pills is expected to begin shortly.
It is also unclear whether the surge in the United States will follow the same pattern as South Africa’s, which rapidly passed the peak of omicron cases last week.
South Africa’s population is significantly younger and has far lower vaccination rates, with about 35 percent of the population immunized, and virtually no oneboosted.The country also grappled with a delta variant wave that infected a far greater portion of the population than it did in the United States.
The significant number of South African residents infected with delta compared with the United States could prove to be an important distinction that might make more Americans vulnerable to omicron, said Chris Beyrer, an epidemiologist at the Johns Hopkins Bloomberg School of Public Health.
Beyrer also noted that infections in the United States, Britain and Germany seemed to be increasing at a significantly faster rate than they were in South Africa.
“This is an incredibly infectious virus and it is moving right along,” Beyrer said. He added that the United States has numerous tools — including ready access to vaccines and booster shots, the new antiviral medicines, testing and masking — that could help curb its effects.
But referring to those who have refused to follow public health guidelines, Beyrer said, “We have a lot of resistance so that makes us vulnerable to infection.”
The number of children with covid-19 recently hospitalized in New York City has increased by nearly five times this month, state officials said at a news conference Monday.
For the week from Dec. 5, 22 children with covid-19 were admitted to hospitals in the city. During a five-day period beginning on Dec. 19, that figure rose to 109, reflecting a broader national surge in coronavirus infections driven in part by the omicron variant. Daily case counts in recent days have climbed to levels not seen since last winter, when coronavirus vaccines weren’t widely available, though the total number of hospitalizations is still significantly lower.
The increase in pediatric covid patients in New York City has been mirrored nationwide. As of last week, nearly 2,000 confirmed or suspected pediatric covid patients were hospitalized nationally, a 31 percent jump in 10 days.
New York City officials are hoping a city mandate that took effect Monday requiring workers at an estimated 184,000 businesses to get at least one vaccine dose will curb infections. “We need more and more people vaccinated,” Mayor Bill de Blasio (D) told reporters. “We need to keep doubling down on vaccination to get out of the covid era once and for all.”
De Blasio’s office announced the mandate earlier this month, just days after health officials disclosed the first case of the more transmissible omicron variant in the United States. But the mayor leaves office in a few days. Kathryn Wylde, president of the Partnership for New York City, a major corporate advocacy group, said she hopes Mayor-elect Eric Adams (D) will show flexibility in enforcement, the Associated Press reported.
Roughly 92 percent of the city’s adult population has received at least one dose of a vaccine, municipal data show, while 83 percent of adults are considered fully immunized. Youth vaccination rates remain lower: Nearly half the children ages 5 to 17 have not yet received a single dose, according to the city government.


 South Africa reported identification of Omicron on Nov. 24.Source: Johns Hopkins University
South Africa reported identification of Omicron on Nov. 24.Source: Johns Hopkins University