

Cartoon – Modern Pain Management


https://mailchi.mp/7788648545f0/the-weekly-gist-february-25-2022?e=d1e747d2d8

In our recent conversations with executives, we’ve heard that the workforce crisis continues to be the most urgent issue confronting health systems.
It’s a many-sided problem: early retirements hitting the nursing staff, leading to an overall loss of experience; early and mid-career nurses choosing to work for temporary staffing agencies for much higher pay, resulting in increased labor costs and resentment among remaining nurses; and a rising vacancy rate made more challenging by difficulty competing for talent against others offering higher pay and less stressful work environments.
But one factor undermining frontline nurse engagement hadn’t occurred to us, until we heard a chief nursing officer describe it this week. The lingering supply chain crisis is forcing hospitals to change where they purchase basic items—think IV tubing and bags, surgery kits, some basic drugs—which in turn forces nurses to adapt to using unfamiliar supplies on the fly, making for a less predictable work environment. On a busy and staff-constrained nursing unit, even small changes to standard procedures can be incredibly frustrating for nurses, and even lead to patient safety issues. Just another way in which the current environment is creating unprecedented pressure on healthcare workers, with little prospect for improvement anytime soon.
https://mailchi.mp/7788648545f0/the-weekly-gist-february-25-2022?e=d1e747d2d8
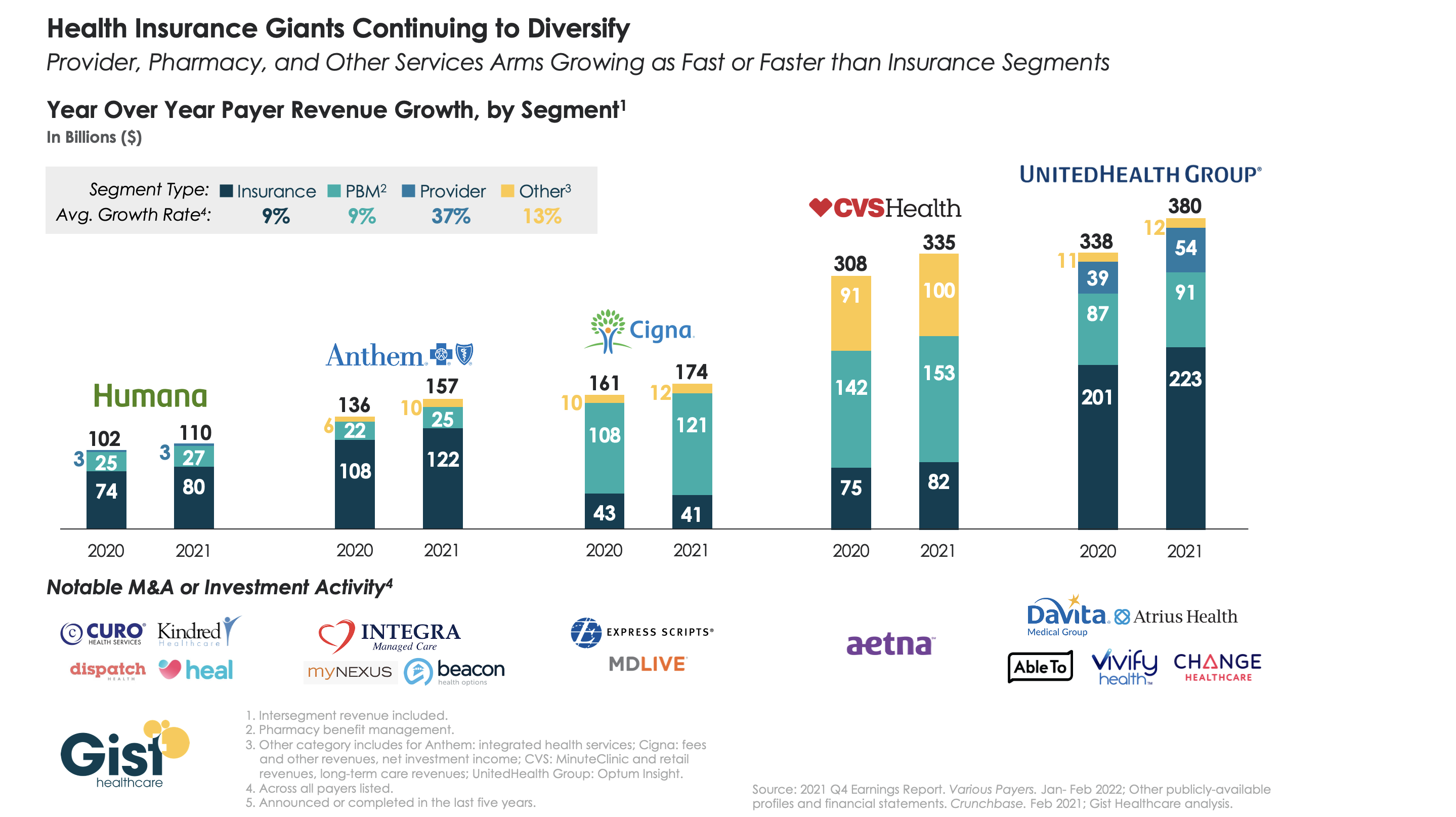
The largest health insurers are quickly becoming vertically integrated healthcare organizations that span the care and coverage continuum. While 2021 was a mixed year for these companies as healthcare volumes bounced back, their diversified portfolios helped cushion losses from higher claims.
The graphic above analyzes revenue growth by segment for the five largest insurers across the last two years. On average the insurance and pharmacy benefit management components of the companies grew at nine percent, while care delivery and integrated health services grew at much higher rates. UnitedHealth Group (UHG) and Anthem boasted the highest year-over-year revenue growth, driven by UHG’s Optum subsidiary and Anthem’s integrated health services.
Cigna and CVS Health each earned less than a quarter of their total revenue from their insurance arms last year. While Humana lags the others in topline revenue, it has assembled a robust portfolio of care delivery investments and partnerships, surpassed only by UHG.
As antitrust scrutiny on vertical integration increases (case in point: the DOJ is now challenging UHG’s acquisition of Change Healthcare), insurers will face the hard task of integrating their portfolio of service—and demonstrating that they deliver value to consumers and patients.
https://mailchi.mp/7788648545f0/the-weekly-gist-february-25-2022?e=d1e747d2d8
A recent New Yorker article details the history of the American Medical Association’s (AMA) opposition to single-payer healthcare, and the grassroots movement that nearly changed its position in 2019.
Since its founding in the 1840s, the largest association of the nation’s doctors has wielded significant influence over healthcare policy, and has been the most effective opponent of several waves of progressive healthcare reform proposals across the last century. More recent changes in the demographic makeup of its physician constituents have begun to mirror the US population. A quarter of today’s practicing physicians graduated from foreign medical schools, and gender and racial gaps in medical schools have been reduced. Today, half of medical students are female, and half are people of color.
The Gist: The perspectives, needs, and politics of the physician community are changing. Younger physicians tend to be more left-leaning, and more are employees, rather than entrepreneurial business owners. While physician pocketbook issues historically dominated the AMA’s policy positions, today’s younger physicians are increasingly motivated by social justice concerns, leading to advocacy positions that would have been unimaginable a few decades ago.
Physician societies continue to move closer to endorsing more extensive healthcare reform policies, over trying to ensure economic protection for the profession—and in the long run, this shift in physician support could prove a key driver in increasing public approval of “Medicare for All” and other coverage reforms.
https://mailchi.mp/7788648545f0/the-weekly-gist-february-25-2022?e=d1e747d2d8

The February 14th deadline for healthcare workers to receive their first dose of the COVID vaccine does not appear to have significantly worsened the hospital staffing crisis, even in rural hospitals. But the mandate hasn’t necessarily meant that all healthcare workers are now vaccinated, as some hospitals reported approving a flurry of medical and religious exemptions to avoid staff departures.
The Gist: Just as when states and early-adopter health systems enforced healthcare worker vaccine mandates last year, COVID vaccine uptake jumped just ahead of the federal deadline.
After months of challenges, we may finally be moving beyond debates over healthcare worker vaccine requirements. And as hospitalizations from the Omicron wave continue to decline, most states and health systems are not planning to implement booster requirements.
https://mailchi.mp/7788648545f0/the-weekly-gist-february-25-2022?e=d1e747d2d8

DOJ alleges that allowing UHG’s Optum subsidiary to acquire Change, a direct competitor used by most large commercial insurers for healthcare claims solutions, would give UHG 75 percent of the healthcare claims processing and management market. This would significantly reduce competition, the DOJ claims, while simultaneously giving UHG access to its competitors’ sensitive plan design and pricing information. UHG called the DOJ’s position ‘deeply flawed’ and promised to fight the case.
The Gist: This is the second big move by antitrust regulators in a week to put the brakes on consolidation in healthcare: shortly after the DOJ sued to block Rhode Island’s two largest health systems, Care New England and Lifespan, from merging, those systems abandoned plans to combine.
We are seeing the first real signs that the Biden administration is following through on plans to more closely scrutinize healthcare deals, including payer-led vertical integration. For both payers and providers, increased scrutiny will place a premium on the consumer value proposition of any combination—and force merging companies to deliver on the benefits of scale.
