


A cylindrical robot rolls into a treatment room to allow health care workers to remotely take temperatures and measure blood pressure and oxygen saturation from patients hooked up to a ventilator. Another robot that looks like a pair of large fluorescent lights rotated vertically travels throughout a hospital disinfecting with ultraviolet light. Meanwhile a cart-like robot brings food to people quarantined in a 16-story hotel. Outside, quadcopter drones ferry test samples to laboratories and watch for violations of stay-at-home restrictions.
These are just a few of the two dozen ways robots have been used during the COVID-19 pandemic, from health care in and out of hospitals, automation of testing, supporting public safety and public works, to continuing daily work and life.
The lessons they’re teaching for the future are the same lessons learned at previous disasters but quickly forgotten as interest and funding faded. The best robots for a disaster are the robots, like those in these examples, that already exist in the health care and public safety sectors.
Research laboratories and startups are creating new robots, including one designed to allow health care workers to remotely take blood samples and perform mouth swabs. These prototypes are unlikely to make a difference now. However, the robots under development could make a difference in future disasters if momentum for robotics research continues.
As roboticists at Texas A&M University and the Center for Robot-Assisted Search and Rescue, we examined over 120 press and social media reports from China, the U.S. and 19 other countries about how robots are being used during the COVID-19 pandemic. We found that ground and aerial robots are playing a notable role in almost every aspect of managing the crisis.
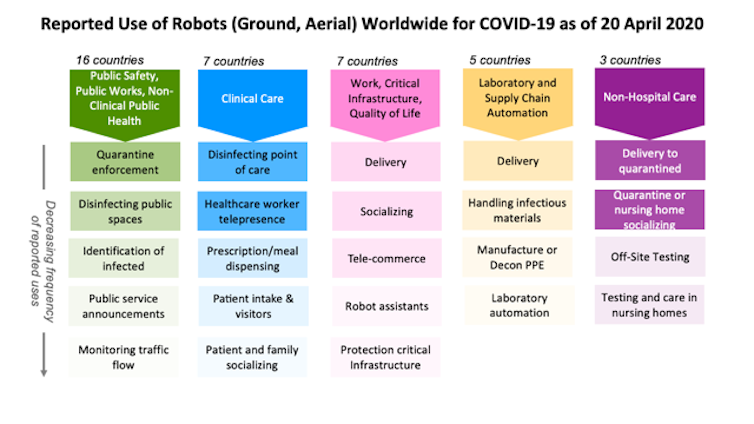
In hospitals, doctors and nurses, family members and even receptionists are using robots to interact in real time with patients from a safe distance. Specialized robots are disinfecting rooms and delivering meals or prescriptions, handling the hidden extra work associated with a surge in patients. Delivery robots are transporting infectious samples to laboratories for testing.
Outside of hospitals, public works and public safety departments are using robots to spray disinfectant throughout public spaces. Drones are providing thermal imagery to help identify infected citizens and enforce quarantines and social distancing restrictions. Robots are even rolling through crowds, broadcasting public service messages about the virus and social distancing.
At work and home, robots are assisting in surprising ways. Realtors are teleoperating robots to show properties from the safety of their own homes. Workers building a new hospital in China were able work through the night because drones carried lighting. In Japan, students used robots to walk the stage for graduation, and in Cyprus, a person used a drone to walk his dog without violating stay-at-home restrictions.
Every disaster is different, but the experience of using robots for the COVID-19 pandemic presents an opportunity to finally learn three lessons documented over the past 20 years. One important lesson is that during a disaster robots do not replace people. They either perform tasks that a person could not do or do safely, or take on tasks that free up responders to handle the increased workload.
The majority of robots being used in hospitals treating COVID-19 patients have not replaced health care professionals. These robots are teleoperated, enabling the health care workers to apply their expertise and compassion to sick and isolated patients remotely.

A small number of robots are autonomous, such as the popular UVD decontamination robots and meal and prescription carts. But the reports indicate that the robots are not displacing workers. Instead, the robots are helping the existing hospital staff cope with the surge in infectious patients. The decontamination robots disinfect better and faster than human cleaners, while the carts reduce the amount of time and personal protective equipment nurses and aides must spend on ancillary tasks.
The second lesson is the robots used during an emergency are usually already in common use before the disaster. Technologists often rush out well-intentioned prototypes, but during an emergency, responders – health care workers and search-and-rescue teams – are too busy and stressed to learn to use something new and unfamiliar. They typically can’t absorb the unanticipated tasks and procedures, like having to frequently reboot or change batteries, that usually accompany new technology.
Fortunately, responders adopt technologies that their peers have used extensively and shown to work. For example, decontamination robots were already in daily use at many locations for preventing hospital-acquired infections. Sometimes responders also adapt existing robots. For example, agricultural drones designed for spraying pesticides in open fields are being adapted for spraying disinfectants in crowded urban cityscapes in China and India.

A third lesson follows from the second. Repurposing existing robots is generally more effective than building specialized prototypes. Building a new, specialized robot for a task takes years. Imagine trying to build a new kind of automobile from scratch. Even if such a car could be quickly designed and manufactured, only a few cars would be produced at first and they would likely lack the reliability, ease of use and safety that comes from months or years of feedback from continuous use.
Alternatively, a faster and more scalable approach is to modify existing cars or trucks. This is how robots are being configured for COVID-19 applications. For example, responders began using the thermal cameras already on bomb squad robots and drones – common in most large cities – to detect infected citizens running a high fever. While the jury is still out on whether thermal imaging is effective, the point is that existing public safety robots were rapidly repurposed for public health.
The broad use of robots for COVID-19 is a strong indication that the health care system needed more robots, just like it needed more of everyday items such as personal protective equipment and ventilators. But while storing caches of hospital supplies makes sense, storing a cache of specialized robots for use in a future emergency does not.
This was the strategy of the nuclear power industry, and it failed during the Fukushima Daiichi nuclear accident. The robots stored by the Japanese Atomic Energy Agency for an emergency were outdated, and the operators were rusty or no longer employed. Instead, the Tokyo Electric Power Company lost valuable time acquiring and deploying commercial off-the-shelf bomb squad robots, which were in routine use throughout the world. While the commercial robots were not perfect for dealing with a radiological emergency, they were good enough and cheap enough for dozens of robots to be used throughout the facility.
Hopefully, COVID-19 will accelerate the adoption of existing robots and their adaptation to new niches, but it might also lead to new robots. Laboratory and supply chain automation is emerging as an overlooked opportunity. Automating the slow COVID-19 test processing that relies on a small set of labs and specially trained workers would eliminate some of the delays currently being experienced in many parts of the U.S.
Automation is not particularly exciting, but just like the unglamorous disinfecting robots in use now, it is a valuable application. If government and industry have finally learned the lessons from previous disasters, more mundane robots will be ready to work side by side with the health care workers on the front lines when the next pandemic arrives.

Of course, no one can pinpoint the exact moment that lightning will strike. But a global pandemic? Experts have predicted it, warned about the preparedness gaps and urged action. Again and again and again.
Just look at 2019. In January, the U.S. intelligence community issued its annual global threat assessment. It declared, “We assess that the United States and the world will remain vulnerable to the next flu pandemic or large-scale outbreak of a contagious disease that could lead to massive rates of death and disability, severely affect the world economy, strain international resources, and increase calls on the United States for support. . . . The growing proximity of humans and animals has increased the risk of disease transmission. The number of outbreaks has increased in part because pathogens originally found in animals have spread to human populations.”
In September, the Johns Hopkins Center for Health Security issued a report titled “Preparedness for a High-Impact Respiratory Pathogen Pandemic.” The report found that if such a pathogen emerged, “it would likely have significant public health, economic, social, and political consequences. . . . The combined possibilities of short incubation periods and asymptomatic spread can result in very small windows for interrupting transmission, making such an outbreak difficult to contain.” The report pointed to “large national and international readiness gaps.”
In October, the Nuclear Threat Initiative, working with the Johns Hopkins center and the Economist Intelligence Unit, published its latest Global Health Security Index, examining open-source information about the state of health security across 195 nations, and scoring them. The report warned, “No country is fully prepared for epidemics or pandemics, and every country has important gaps to address.” The report found that “Fewer than 5 percent of countries scored in the highest tier for their ability to rapidly respond to and mitigate the spread of an epidemic.”
In November, the Center for Strategic and International Studies published a study by its Commission on Strengthening America’s Health Security. It warned, “The American people are far from safe. To the contrary, the United States remains woefully ill-prepared to respond to global health security threats. This kind of vulnerability should not be acceptable to anyone. At the extreme, it is a matter of life and death. . . . Outbreaks proliferate that can spread swiftly across the globe and become pandemics, disrupting supply chains, trade, transport, and ultimately entire societies and economies.” The report recommended: “Restore health security leadership at the White House National Security Council.”
Came out of nowhere? Not even close. The question that must be addressed in future postmortems is why all this expertise and warning was ignored.
https://www.axios.com/coronavirus-west-virginia-first-case-ac32ce6d-5523-4310-a219-7d1d1dcb6b44.html

The pandemic is a long way from over, and its impact on our daily lives, information ecosystem, politics, cities and health care will last even longer.
The big picture: The novel coronavirus has infected more than 939,000 people and killed over 54,000 in the U.S., Johns Hopkins data shows. More than 105,000 Americans have recovered from the virus as of Sunday.
Lockdown measures: Demonstrators gathered in Florida, Texas and Louisiana Saturday to protest stay-at-home orders designed to protect against the spread of COVID-19, following a week of similar rallies across the U.S.
Catch up quick: Deborah Birx said Sunday that it “bothers” her that the news cycle is still focused on Trump’s comments about disinfectants possibly treating coronavirus, arguing that “we’re missing the bigger pieces” about how Americans can defeat the virus.
https://www.axios.com/coronavirus-latest-developments-8b8990c4-6762-494a-8ee0-5091746bda9b.html
Children in Spain were allowed to go outside on Sunday for the first time since a nationwide lockdown aimed at slowing the spread of the novel coronavirus began six weeks ago.
By the numbers: The coronavirus has infected over 2.9 million people and killed over 200,000, Johns Hopkins data shows. More than 829,000 people have recovered from COVID-19. The U.S. has reported the most cases in the world (more than 940,000 from 5.1 million tests), followed by Spain (over 223,000).
What’s happening: Australian Health Minister Greg Hunt announced a new coronavirus tracing app on Sunday that the government hopes at least 50 percent of the population will use. A top health official said the app is “only for one purpose, to help contact tracing,” as he sought to reassure Australians on privacy issues.
The big picture: The world faces its gravest challenge in decades, but geopolitical tensions won’t wait until it’s over. Trump’s threat on Wednesday to “destroy” Iranian boats that harass U.S. ships comes amid arrests of Hong Kong pro-democracy activists and clashes in Afghanistan that could further undermine peace there.
Between the lines: Policy responses to the crisis have been every-country-for-itself and — in the case of the U.S. and China — tinged with geopolitical rivalry.
Coronavirus symptoms: Fever, cough, shortness of breath.
https://coronavirus.jhu.edu/map.html

By the numbers: The coronavirus has infected over 2.9 million people and killed over 200,000, Johns Hopkins data shows. More than 829,000 people have recovered from COVID-19. The U.S. has reported the most cases in the world (more than 940,000 from 5.1 million tests), followed by Spain (over 223,000).


