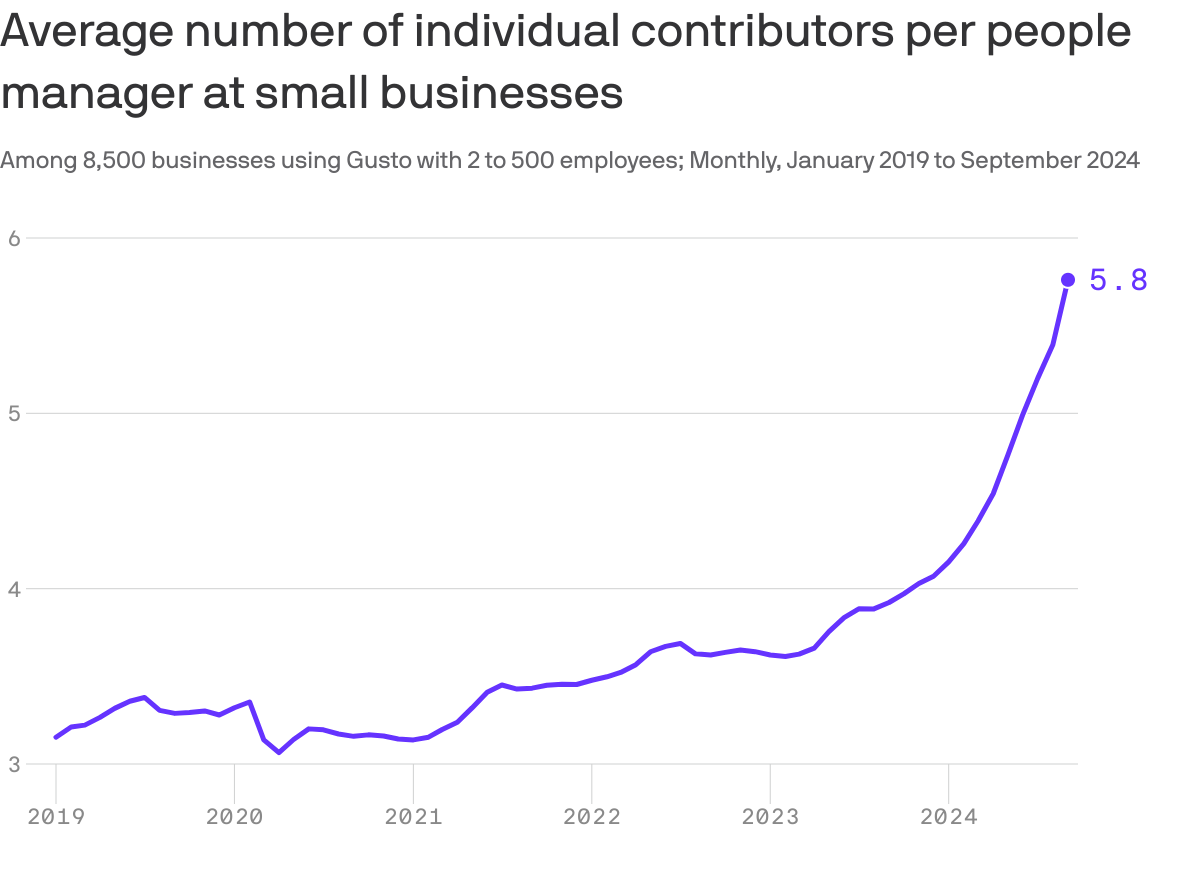
This chart may explain why your boss is taking longer to get back to you lately: They’ve got more underlings to watch over, Axios’ Emily Peck writes from a new analysis.
Why it matters: Middle managers — i.e., bosses who have bosses — were already quietly going extinct, and now AI may be hastening the process.
By the numbers:
People managers now oversee about twice as many workers as just five years ago.
There are now nearly six individual contributors per manager at the 8,500 small businesses analyzed in a report by Gusto, which handles payroll for small and medium-sized employers.
That’s up from a little over three in 2019.
🎨 The big picture:
Big Tech has been shedding middle managers for the past few years, a process that’s been dubbed the Great Flattening.
Reducing management layers is one of Microsoft’s stated goals in laying off thousands of workers this year as it ramps up its AI strategy.
Amazon CEO Andy Jassy last year announced an effort to reduce managers (memo).
The “Big Beautiful Budget Bill” appears headed for passage with cuts to Medicaid and potentially Medicare likely elements.
The economy is slowing, with a mild recession a possibility as consumer confidence drops, the housing market slows and uncertainty about tariffs mounts.
And partisan brinksmanship in state and federal politics has made political hostages of public and rural health safety net programs as demand increases for their services.
Last Wednesday, amidst mounting anxiety about the aftermath of U.S. bunker-bombing in Iran and escalating conflicts in Gaza and Ukraine, the Centers for Medicare and Medicaid Services (CMS) released its report on healthcare spending in 2024 and forecast for 2025-2033:
“National health expenditures are projected to have grown 8.2% in 2024 and to increase 7.1% in 2025, reflecting continued strong growth in the use of health care services and goods.
During the period 2026–27, health spending growth is expected to average 5.6%, partly because of a decrease in the share of the population with health insurance (related to the expiration of temporarily enhanced Marketplace premium tax credits in the Inflation Reduction Act of 2022) and partly because of an anticipated slowdown in utilization growth from recent highs. Each year for the full 2024–33 projection period, national health care expenditure growth (averaging 5.8%) is expected to outpace that for the gross domestic product (GDP; averaging 4.3%) and to result in a health share of GDP that reaches 20.3% by 2033 (up from 17.6% in 2023) …
Although the projections presented here reflect current law, future legislative and regulatory health policy changes could have a significant impact on the projections of health insurance coverage, health spending trends, and related cost-sharing requirements, and they thus could ultimately affect the health share of GDP by 2033.”
As has been the case for 20 years, spending for healthcare grew faster than the overall economy in 2024. And it is forecast to continue through 2033:
2024Baseline
2033Forecast
% Nominal Chg.2024-2033
National Health Spending
$5,263B
$8,585B
+63.1%
US Population
337,2M
354.8M
+5.2%
Per capita personal health spending
$13,227
$20,559
+55.7%
Per capita disposable personal income
$21,626
$31,486
+45.6%
NHE as % of US GDP
18.0%
20.3%
+12.8%
In its defense, industry insiders call attention to the uniqueness of the business of healthcare:
‘Healthcare is a fundamental need: the health system serves everyone.’
‘Our aging population, chronic disease prevalence and socioeconomic disparities are drive increased demand for the system’s products and services.’
‘The public expects cutting edge technologies, modern facilities, effective medications and the best caregivers and they’re expensive.’
‘Burdensome regulatory compliance costs contribute to unnecessary spending and costs.’
And they’re right.
Critics argue the U.S. health system is the world’s most expensive but its results (outcomes) don’t justify its costs. They acknowledge the complexity of the industry but believe “waste, fraud and abuse” are pervasive flaws routinely ignored. And they remind lawmakers that the health economy is profitable to most of its corporate players (investor-owned and not-for-profits) and its executive handsomely compensated.
Healthcare has been hit by a perfect storm at a time when a majority of the public associates it more with corporatization and consolidation than caring. This coalition includes Gen Z adults who can’t afford housing, small employers who’ve cut employee coverage due to costs and large, self-insured employers who trying to navigate around the 10-20% employee health cost increase this year, state and local governments grappling with health costs for their public programs and many more. They’re tired of excuses and think the health system takes advantage of them.
As a percentage of the nation’s GDP and household discretionary spending, healthcare will continue to be disproportionately higher and increasingly concerning. Spending will grow faster than other industries until lawmakers impose price controls and other mechanisms like at least 8 states have begun already.
Most insiders are taking cover and waiting ‘til the storm passes. Some are content to cry foul and blame others. Others will emerge with new vision and purpose centered on reality.
Storm damage is rarely predictable but always consequential. It cannot be ignored. The Perfect has Hit U.S. healthcare. Its impact is not yet known but is certain to be a game changer.
“We urge the Administration to consider the timing of these policies in the context of the broader scope of requirements and challenges facing the industry that require significant system changes.”
AHIP, March 13, 2023 (in a letter to CMS Administrator Chiquita Brooks-LaSure responding to CMS’s proposed rule on Advancing Interoperability and Improving Prior Authorization Processes, proposed Final Rule, CMS-0057-P)
“Health insurance plans today announced a series of commitments to streamline, simplify and reduce prior authorization – a critical safeguard to ensure their members’ care is safe, effective, evidence-based and affordable.”
After lobbying aggressively to delay implementation of the PA reforms proposed by the previous administration (successfully delayed one year and counting), AHIP, the big PR and lobbying group for health insurers, now claims the mantle of reformer, announcing a set of voluntary commitments to streamline prior authorization.
So naturally, the industry’s “commitments” deserve closer scrutiny. Let’s unpack them. As a former health insurance industry executive, I speak their language, so allow me to translate. AHIP, which has no enforcement power, by the way, claims that 48 large insurers will:
Develop and implement standards for electronic prior authorization using Fast Healthcare Interoperability Resources Application Programming Interfaces (FHIR APIs).Translation:CMS is already requiring all insurers to do this by 2027. We might as well take credit preemptively.
Reduce the volume of in-network medical authorizations. Translation:We already demand hundreds of millions of unnecessary prior authorizations for thousands of procedures and services, so cutting a few (who knows how many?) should be a layup and won’t cut into profits.
Enhance continuity of care when patients change health plans by honoring a PA decision for a 90-day transition period starting in 2026.Translation:We’re already required to do this in Medicare Advantage. And since we delayed implementation of e-authorization until 2027, we’re in the clear until then anyway.
Improve communications by providing members with clear explanations for authorization determinations and support for appeals. Translation:We’re already required by state and federal law to do this. We’ll double-check our materials.
Ensure 80% of prior authorizations are processed in real time and expand new API standards to all lines of business. Translation:We had to promise to hold ourselves accountable to at least one measurable goal. We will set the denominator – we’ll decide which procedures and medications require PA – so we’ll hit this goal, no problem, and we might even use more non-human AI algorithms to do it.
6. Ensuring medical review of non-approved requests. Translation:People will be relieved we’re not using robots. And we’ll avoid having Congress insist that reviews must be done by a same-specialty physician, as proposed in the Reducing Medically Unnecessary Delays in Care Act of 2025 (H.R. 2433).
Of course, I wasn’t in the room when AHIP drafted these commitments, so take my translations with a grain of salt. But let’s be honest: These promises are thin on specifics, short on accountability, and devoid of measurable impact.
It’s also rich coming from an industry still reliant on something called the X12 transaction standard – technology that is now over 40 years old – to process prior authorization requests, while simultaneously pointing the finger at providers for outdated technology and being slow to adopt modern systems. Many insurers did not start accepting electronic submissions of prior authorization until roughly 2019, nearly 20 years after clinicians started using online portals such as MyChart in their regular practice. The claim that providers are the ones behind on technology is another ploy by insurers to dodge scrutiny for their schemes.
We shouldn’t settle for incremental fixes when the system itself is the problem. Nor should we allow the industry that created this problem – and perpetuates it in its own self-interest – to dictate the pace or terms of reforming it.
As we argued in our recent piece, Congress should act to significantly curtail the use of prior authorization, limiting it to a narrow, evidence-based set of high-risk use cases. Insurers should also be required to rapidly adopt smarter, lower-friction cost-control methods, like gold-carding trusted clinicians (if it can be implemented with integrity and fairness), without compromising patient access or clinical autonomy.
Letting the fox design the hen house’s security perimeter won’t protect the hens. It’s time for Congress to build a better fence.
Health insurers and their lobbying arms have spent $476.5 million since 2020 to block reform, protect profits, and mislead the public — and it’s coming straight from our premiums and tax dollars.
AHIP, the big PR and lobbying outfit for most health insurers, undoubtedly believes the praise it got from Trump administration officials and some members of Congress this week – when it announced changes insurers presumably will make voluntarily to alleviate the burden of prior authorization demands on patients and health care providers – has taken the heat off insurers. AHIP’s message to Washington politicos: You don’t need to pass any new laws to make us do the right thing. You can trust us, despite our decades of engaging in untrustworthy behavior to maximize profits.
After all, AHIP is nothing more than a PR and lobbying shop with millions of our dollars to play with. It has zero ability to force insurers to do what AHIP claims they will do. I know this because I worked closely with AHIP during my 20 years in the industry and represented Cigna on its strategic communications committee.
From Fox to “Fixer”?
AHIP pulled off its big show on Monday – and got plenty of generally fawning press coverage – because of all the money it and affiliated insurers throw around Washington every year to protect what has become an incredibly profitable status quo.
Collectively, the seven biggest for-profit insurers reported $70 billion in profits last year.
(Beleauered UnitedHealth alone reported $34.4 million in operating earnings.) And that’s just seven among dozens. One way they make that kind of dough, for their shareholders and top executives, is by using prior authorization to avoid paying for patients’ medically necessary care. Many people die as a result, while investors get richer. It’s that simple and that cold.
So just how much money does AHIP and the insurance industry spend to bamboozle members of Congress and the White House every year? We’re talking stupid money. And orders of magnitude more than nonprofits that advocate for reforms that would benefit patients instead of shareholders.
Nearly Half a Billion Ways They Tip the Scale
To find out just how much, I turned to OpenSecrets and did some math. OpenSecrets, as a reminder, is the well-named organization that keeps tabs on campaign contributions and lobbying expenses.
What I discovered is that AHIP has spent almost $65 million lobbying Congress and the Biden and Trump administrations since 2020. Its cousin, the Blue Cross Blue Shield Association, has spent even more. More than twice as much more.
And that, folks, is just the tip of the iceberg, and it doesn’t even include the tens of millions the industry spends on massive advertising campaigns inside the DC beltway that it’s not required to report. Or the dark money ads and advocacy the industry bankrolls.
But just the lobbying totals are mind-blowing. When you factor in the money spent by the big seven insurers and the other PR and lobbying groups that insurers funnel money to, the total grows to almost $500 million. You read that right: nearly half a billion dollars.
Most of that spending was during the Biden administration, but the industry is on track to break spending records during the first year of the current Trump administration. They are lobbying not only to beat back new laws and regulations that could constrain their prior authorization practices but also to protect their biggest cash cows: Medicare Advantage and their pharmacy benefit managers (PBMs).
Three PBMs – owned by Cigna, CVS/Aetna and UnitedHealth –control 80% of the pharmacy benefit market and determine which drugs we’ll have access to and how much we have to pay out of pocket even with insurance.
The Big Number
$476.5 million – That’s the amount of money health insurance corporations and four of their PR and lobbying groups – AHIP, BCBSA (which includes contributions from Elevance/Anthem as well as numerous other BCBS companies), the Pharmaceutical Care Management Association and the Better Medicare Alliance – have collectively spent on lobbying Congress and federal regulators between January 1, 2020, and March 31, 2025.
Keep in mind that that money is not coming out of executives’ paychecks. It’s coming out of our pockets. Insurers skim money from our premiums and taxes to finance their propaganda and lobbying efforts to keep the gravy train rolling. And it’s in addition to all the campaign cash they dole out every year, which I tabulated recently.
This is not to say that reform is impossible. Scrappy advocacy groups with a tiny fraction of that total have scored important victories over the years. But it is why progress is so slow and setbacks are so frequent.
But just imagine how all that money could be put to better use to ensure that all Americans, including those with insurance, are able to get the care they need when they need it. It’s clear that in addition to reforming our health care system, we need political reforms that make it more difficult for big corporations and their trade groups to influence elections and public policy.
New Medicaid funding rules proposed by Congress this week would halt efforts at the state level to better fund rural hospitals and deliver services to the most vulnerable populations in those areas. You can be certain that the administrators and staff of those hospitals, as well as leaders of the communities they serve, are watching closely to see if the cuts are enacted.
Lawmakers at the federal level are trying to make deeper cuts to Medicaid spending in an effort to lower the amount of deficit spending that would be created by President Trump’s spending plan. Trump has dubbed the plan his “big beautiful bill.”
Feds Would Strip Rural Hospitals of Lifeline Funds
Republican members of the Senate Finance Committee this week released their version of the bill that would drain funding for rural hospitals, which rely heavily on Medicaid funds to treat patients. It’s estimated that 25 to 40 percent of services provided by such hospitals are funded by Medicaid.
The federal government and states share the up-front medical costs for Medicaid patients. The federal government then reimburses states up to 50 percent of their Medicaid spending every year.
Many states fund their portion of the cost by taxing entities that provide those services to Medicaid patients.
The latest proposal in Congress would not only restrict how many patients could receive benefits, but it would also stop states from implementing those provider tax programs to help fund Medicaid services provided to residents.
At the federal level, the thinking is that if states keep taxing providers to fund Medicaid services, then the federal government will have to keep reimbursing states a portion of those costs.
The downside to that is many experts, along with several Republicans in Congress, namely Sens. Susan Collins of Maine, Lisa Murkowski of Alaska and Josh Hawley of Missouri, have predicted it will decimate rural hospitals.
West Virginia Republican Sen. Jim Justice went a step further, saying that the plan to limit states’ use of provider taxes will “really hurt a lot of folks.” Despite that statement, Justice said he is OK with the freeze.
State Lawmakers Sound the Alarm
There are 39 states with at least three or more provider taxes used to help fund Medicaid services. Alaska is the only state with no such tax.
Some states, such as Ohio, have set up a new rural hospital fund using provider taxes to help rural hospitals deliver Medicaid services to patients.
Ohio Governor Mike DeWine and the Republican-led state legislature set up a pilot program called the Rural Ohio Hospital Tax Pilot Program. The measure would allow counties to levy a tax on their local hospitals that would then be used to fund Medicaid services.
DeWine said the pilot program would help ease the financial stress rural hospitals face in Ohio. The plan contained in Ohio House Bill 96 has the blessing of the Ohio Hospital Association.
A group of Republican state lawmakers recently sent a letter to their federal counterparts pleading with them to remove the bill language because it would “torpedo” plans to keep rural hospitals functioning.
The American Hospital Association, a 130-year-old trade group of more than 5,000 hospitals and health care providers, this month released the impact on rural hospitals if this plan went into effect.
More than $50 billion would be lost by 2034, and more than 1.8 million rural Americans would lose health benefits.
Kentucky residents would be impacted the most, with 143,000 losing benefits, followed by 135,000 Californians. More than 86,000 Ohioans would lose Medicaid coverage under the plan by 2034, making it the third most impacted state.
To blunt the effects of the cuts, Collins reportedly is proposing the establishment of a $100 billion relief fund that could provide financial support to affected providers, rural hospitals in particular. Whether that or a similar but smaller fund will wind up in the final draft of the legislation apparently will be decided this weekend. Meanwhile, the Senate parliamentarian has ruled against many of the provisions of the Senate version of the bill, including the Finance Committee’s provider tax framework, which puts the whole thing in flux.
Senate leaders say they plan a long series of votes on amendments of the bill on Sunday. The “vote-arama” likely will go on throughout Sunday night and into Monday. If the Senate does pass its version of the bill, it will have to go back to the House. Lawmakers are under a self-imposed deadline to get the legislation to Trump by the July 4 holiday.
Medicaid serves as a vital source of health insurance coverage for Americans living in rural areas, including children, parents, seniors, individuals with disabilities, and pregnant women. Congressional lawmakers are currently considering more than $800 billion in cuts to the Medicaid program, which would reduce Medicaid funding and terminate coverage for vulnerable Americans.
The proposed changes would also result in a significant reduction in Medicaid reimbursement that could result in rural hospital closures.
The National Rural Health Association recently partnered with experts from Manatt Health to shed light on the potential impacts of those cuts on rural residents and the hospitals that care for them over the next decade.
NRHA held a press conference on June 24 that can be accessed with passcode MBTZf4$H. NRHA chief policy officer Carrie Cochran-McClain discussed the findings with Manatt Health partner and former deputy administrator at CMS Cindy Mann and the real world implications of the details of this report with three NRHA member hospital and health system leaders
Report findings provide insight into the impact on rural America at a critical moment in the Congressional debate over the future of the reconciliation package.
The report shows the significant impact from coverage losses that rural communities will face given:
Medicaid plays an outsized role in rural America, covering a larger share of children and adults in rural communities than in urban ones.
Nearly half of all children and one in five adults in small towns and rural areas rely on Medicaid or CHIP for their health insurance.
Medicaid covers nearly one-quarter of women of childbearing age and finances half of all births in these communities.
According to Manatt’s estimates, rural hospitals will lose 21 cents out of every dollar they receive in Medicaid funding due to the One Big Beautiful Bill Act. Total cuts in Medicaid reimbursement for rural hospitals—including both federal and state funds—over the ten-year period outlined in the bill would reach almost $70 billion for hospitals in rural areas.
Reductions in Medicaid funding of this magnitude would likely accelerate rural hospital closures and reduce access to care for rural residents, exacerbating economic hardship in communities where hospitals are major employers.
As a key insurer in rural communities, Medicaid provides a financial lifeline for rural health care providers — including hospitals, rural health clinics, community health centers, and nursing homes—that are already facing significant financial distress. These cuts may lead to more hospitals and other rural facility closures, and for those rural hospitals that remain open, lead to the elimination or curtailment of critical services, such as obstetrics.
“Medicaid is a substantial source of federal funds in rural communities across the country. The proposed changes to Medicaid will result in significant coverage losses, reduce access to care for rural patients, and threaten the viability of rural facilities,” said Alan Morgan, CEO of the National Rural Health Association.
“It’s very clear that Medicaid cuts will result in rural hospital closures resulting in loss of access to care for those living in rural America.”
A media briefing will be held on Tuesday, June 24, from noon to 1:00 PMEST to provide more information about the analysis. This event will feature representatives from NRHA, Manatt Health, and rural hospital leaders across the country. Questions may be submitted in advance, as well as during the press conference. To register for and join the media briefing, click on the Zoom link here.
NRHA is a non-profit membership organization that provides leadership on rural health issues with tens of thousands of members nationwide. Our membership includes nearly every component of rural America’s health care, including rural community hospitals, critical access hospitals, doctors, nurses, and patients. We work to improve rural America’s health needs through government advocacy, communications, education, and research. Learn more about the association at RuralHealth.US.
About Manatt Health
Manatt Health is a leading professional services firm specializing in health policy, health care transformation, and Medicaid redesign. Their modeling draws upon publicly available state data including Medicaid financial management report data from the Centers for Medicare and Medicaid Services, enrollment and expenditure data from the Medicaid Budget and Expenditure System, and data from the Medicaid and CHIP Payment and Access Commission. The Manatt Health Model is tailored specifically to rural health and has been reviewed in consultation with states and other key stakeholders.