The coronavirus pandemic has torn through the global economy, suppressing consumer demand and industrial production. As countries look to an eventual recovery, but in a very different environment characterized by continuing distancing measures and loss of public confidence, businesses in many sectors, such as hospitality and retail, are asking how they can adapt to survive these new economic conditions. Yet perhaps surprisingly, those feeling threatened include independent primary care practices in the United States. Despite the USA being one of the most expensive healthcare systems in the world, many primary care practices are now facing financial collapse. Some estimates suggest that primary care practices will lose up to $15 billion during 2020 as a consequence of the coronavirus pandemic.
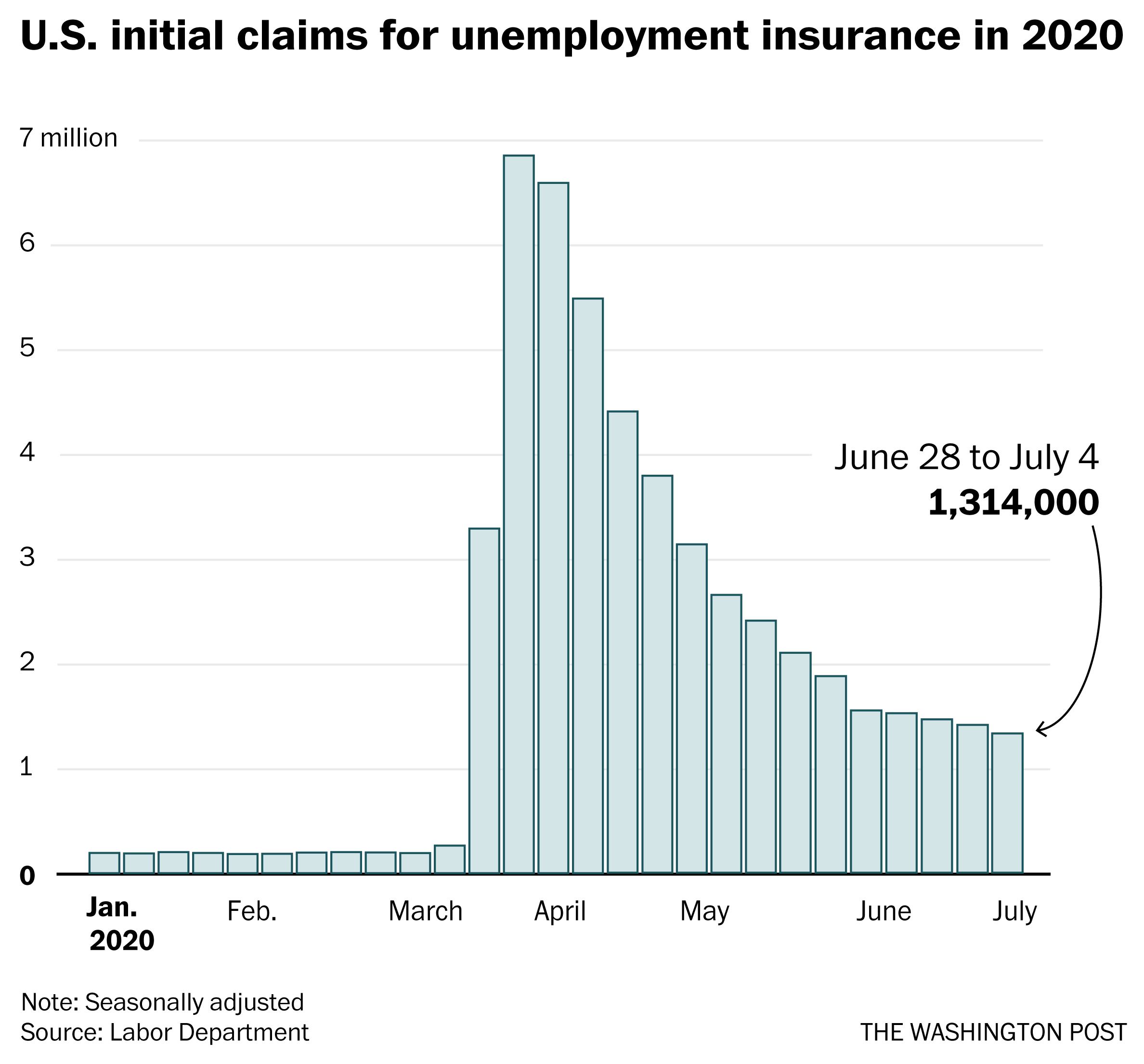
Covid-19 has highlighted a fundamental weakness in how primary care is paid for in the USA. Many practices are financed by fee-for-service (FFS) reimbursement. Put bluntly, providers make money from office visits, diagnostic tests, and procedures. This has long been criticized for encouraging an expansion of what is considered disease and overtreatment, contributing to the high cost of the American health system. However, it can only work as long as patients keep coming, and they are no longer doing so, at least not in sufficient numbers for many primary care practices to remain viable. The imposition of social distancing policies has seen a severe reduction in office visits, and with it a substantial decline in revenue. The pandemic has taught Americans that the financial model that underpins primary care needs to be reformed. It needs to move from a per-visit reimbursement to a per-patient reimbursement, in other words primary care capitation, as used in many other countries, including the UK.
If the existing reimbursement model is not reformed, the clinical and financial implications for struggling primary care practices, which could play a key role in the continuing coronavirus pandemic, will be far-ranging. From a clinical standpoint, primary care practices that need to lay off staff or close will not be able to respond effectively to an influx of patients who have been delaying care since the pandemic began. Given that primary care is often the entry point into the healthcare system, this could lead to severe reductions in access to routine health care as well as referrals to specialty providers for advanced complaints. From a financial standpoint, many of these independent practices may consider consolidation with larger health systems, something that has been shown to increase prices without improving quality in the long run.
To overcome these issues, insurers and primary care practices could work together to construct capitated payment models. In capitated contracts, providers are paid a risk-adjusted sum for each patient enrolled in the practice. Payment to providers is not reliant on volume of office visits, but rather delivering cost-effective care focused on the health of primary care patients.
As we noted above, this system is already widely used internationally, but there are also good examples in the USA. For example, Iora Health is a venture-backed primary care company that partners with insurers to obtain a flat $150 per-member-per-month (PMPM) fee for taking care of its patients. They also receive bonuses for reducing total cost of care (TCOC). As a result, they have been able to use their dollars for health-related interventions, such as hiring health coaches. They have also demonstrated significant reductions in hospitalizations and health spending along with high patient satisfaction scores. Most importantly, they were able to quickly adapt to the needs of their patient population in the pandemic using alternative models of care, such as online consultations, without the added stress of losing revenue.
There are also many other promising examples of both public and private payers designing capitated contracts for independent primary care practices. In the public sector, the Centers for Medicare and Medicaid Services (CMS) introduced the multi-payer Primary Care First (PCF) Model. Under PCF, primary care practices will receive a risk-adjusted population-based payment for patients as well as a flat fee for any office visits performed. In addition, there are bonuses for practices to limit hospitalizations, an expensive component of delivering care. However, this is still an experimental program that is supposed to begin in 2021, which may be too late for primary care practices that are already facing financial strain from the pandemic.
In the private sector, Blue Cross Blue Shield of North Carolina (BCBS NC) has created the Accelerate to Value program for independent primary care practices. Through this program, BCBS NC is offering independent primary care practices a supplemental stabilization payment, based on the number of members a particular practice serves. In return, it is asking them to remain open for patients and deliver care appropriate to the circumstances created by the pandemic. In the longer term, it also asks them to join an accountable care organization (ACO) and consider accepting capitation for future reimbursement.
While CMS and BCBS can offer blueprints for a path towards primary care capitation, there will be challenges to implement capitation at scale across the nation’s primary care system. A key defining aspect of the US healthcare system is its multitude of payers, from commercial to Medicaid to Medicare. For primary care capitation to succeed, practices will need to pursue multi-payer contracts that cover a critical mass of the patients they serve. Independent practices will also have to adapt to a fixed budget model where excess healthcare utilization could actually lead to financial losses, unlike in fee-for-service.
Ultimately, it is important to recognize that no payment model will be a panacea for healthcare providers during the pandemic and afterwards. However, the coronavirus pandemic has highlighted clear deficiencies in the American fee for service system that have existed for almost a century. Covid-19 has created an opportunity for policymakers and providers to look anew at a model that is already implemented widely in other countries, and in parts of the US. At some point there will have to be an inquiry into the many failures that have characterized the American response to covid-19. Given the magnitude of the catastrophe that has befallen the US, in stark contrast to the relative successes achieved in many other countries, it will be essential to challenge many things once taken for granted. One must be the fee for service system that has so clearly undermined the resilience of the US health system. Covid-19 has provided an almost unprecedented opportunity to create a healthcare system that rewards providers caring for patients in a coordinated manner, rather than prioritizing expensive and often wasteful healthcare provision.





%2Farc-anglerfish-washpost-prod-washpost%2FKH6QH7FVNYI6VGQ52PNRZPQHZY.jpg&w=908)