State governments are building armies of contact tracers in a new phase of the battle against the coronavirus pandemic, returning to a fundamental practice in public health that can at once wrestle the virus under control and put hundreds of thousands of newly jobless people back to work.
California is already conducting contact tracing in 22 counties, and it eventually plans to field a force of 10,000 state employees, who will be given basic training by University of California health experts.
Massachusetts and Ohio have partnered with Partners in Health, a global health nonprofit originally established to support programs in Haiti, to field teams of contact tracers. Maryland will partner with the University of Chicago and NORC, formerly the National Opinion Research Center, to quadruple its contact tracing capacity.
Washington, West Virginia, Iowa, North Dakota and Rhode Island are using their National Guards to trace contacts of those who have been infected with the coronavirus. In Kansas, 400 people have volunteered to trace contacts; in Utah, 1,200 state employees have raised their hands.
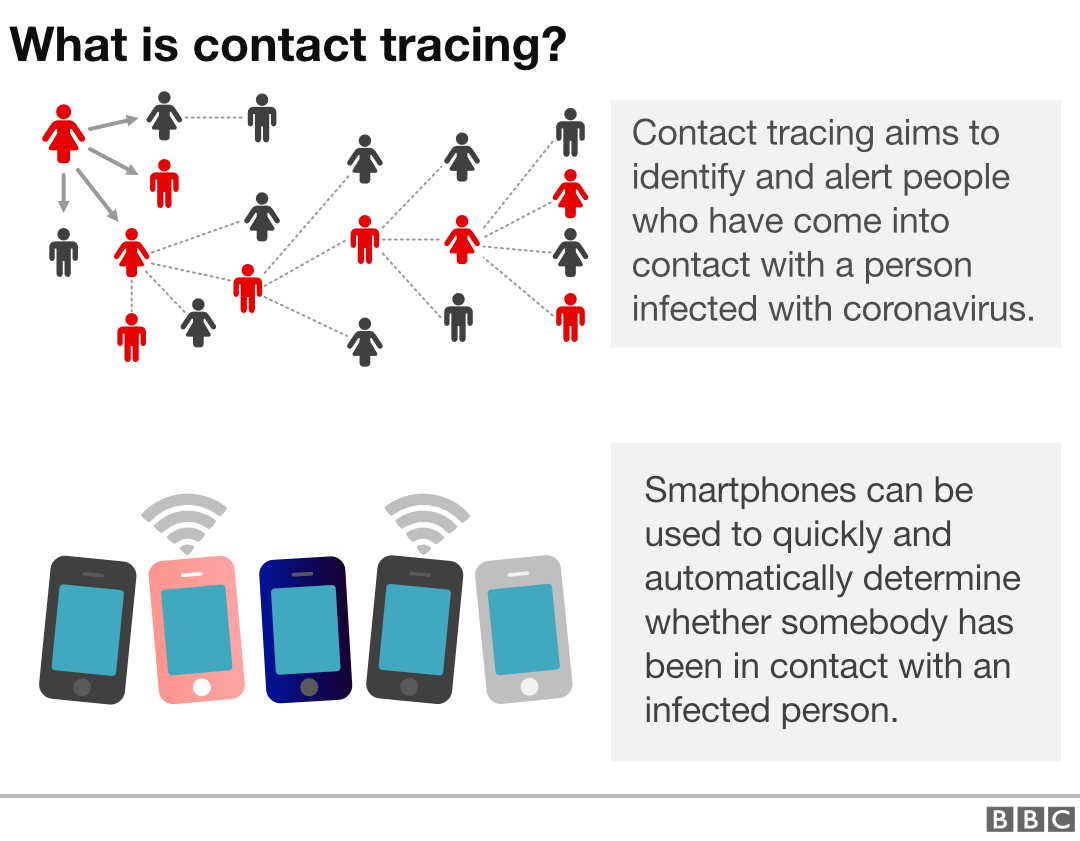
Contact tracing is a pillar of basic public health, a critical element in battling infectious disease around the globe. The goal is to identify those who have been infected with a virus and those with whom the infected person has come into contact.
If those contacts then come down with the virus, they can be quickly isolated so they do not spread it further. They can also be treated, making it less likely they develop the most severe symptoms.
The practice works even in areas where health systems are thin at best and nonexistent at worst.
Tracking down those who had the Ebola virus in Guinea, Liberia and Sierra Leone, three of the poorest nations on Earth, was critical to ending the world’s largest outbreak of the deadly hemorrhagic fever in 2015. World Health Organization trackers and health officials in Congo have tracked as many as 25,000 people at a time during an Ebola outbreak that is still simmering in an eastern province, even as they face the threat of what is an almost active war zone.
“Our ability to suppress transmission relates to our ability to detect the virus,” Maria Van Kerkhove, the American who leads the World Health Organization’s technical team studying the coronavirus, told reporters last week.
The focus on contact tracing comes as public health experts warn that the coronavirus will not end as a threat to humankind until so many people have become infected that the virus has nowhere else to turn — a terrifying prospect that conjures images of overwhelmed health systems and death on a mass scale — or until scientists develop and distribute an effective vaccine to billions of people across the globe.
There are more than 100 vaccines in some stage of testing, though determining their effectiveness is still months away, and production at a mass scale is months beyond that. Anthony Fauci, director of the National Institute of Allergy and Infectious Diseases and the country’s most well-known infectious disease expert, has estimated that a vaccine could be as close as 18 months away, though he has acknowledged that would blow the old record for speedy development out of the water.
“We have to fundamentally do everything possible to get a safe and effective vaccine as quickly as possible. At the same time, we have to assume that it’s not around the corner,” said Tom Frieden, former director of the Centers for Disease Control and Prevention who now runs Resolve to Save Lives, a global health nonprofit.
In the meantime, the federal government has largely left it up to the states to build their contact tracing capacity.
Sen. Elizabeth Warren (D-Mass.) and Rep. Andy Levin (D-Mich.) have proposed adding a massive nationwide federal contact tracing program to the next round of coronavirus-related relief funding. In a nod to the New Deal-style scale such a program would require, they call the program the Coronavirus Containment Corps.
“Establishing a nationwide contact tracing program is the only way we can truly know the progress we’ve made in containing the virus, and how far we have left to go before we can transition back to normal life,” Levin said in a statement.
But contact tracing can work only if the number of new cases the United States confirms every day begins to bend down to a manageable number. The number of cases confirmed in the United States has grown by at least 25,000 on all but two of the first eight days of May.
And tracing will become an effective tool only when those who are conducting the tracing have the ability to test people broadly and to get the results of those tests back quickly. The Food and Drug Administration said Friday it had approved both the first diagnostic test that could be conducted using home-collected saliva samples and the first antigen test, a type of test that delivers results much faster than others on the market.
The lack of available tests at the earliest stages of the coronavirus outbreak has hidden the true extent of the virus’s spread around the United States. While some countries have the capacity to test huge percentages of their population on a given day, the United States is still testing only about 250,000 people per day, a level far short of the capacity necessary to conduct widespread contact tracing.
“Right from the start there has been a tremendous undercounting of cases, and that had to do with our now infamous slow testing rollout,” said Paul Sax, clinical director of the division of infectious diseases at Brigham and Women’s Hospital in Boston.
President Trump has touted the raw number of tests performed — he rightly claims that the United States conducts more tests on a given day than any other country. But on a per capita basis, the United States is testing fewer of its residents than countries such as the United Kingdom, Italy and Estonia.
Until that changes, public health experts worry the United States will be stuck at a dangerous plateau.
“We’re doing deeply inadequate testing and functionally no tracing,” said Jeremy Konyndyk, a former head of the Office of Foreign Disaster Assistance at the U.S. Agency for International Development and now a senior fellow at the Center for Global Development. “We’re not going to half-ass our way out of a pandemic, and that’s where we are, and that’s why we’re stuck.”