Nearly 12 million people would lose their health insurance under President Trump’s “big, beautiful bill,” an erosion of the social safety net that would lead to more unmanaged chronic illnesses, higher medical debt and overcrowding of hospital emergency departments.
Why it matters:
The changes in the Senate version of the bill could wipe out most of the health coverage gains made under the Affordable Care Act and slash state support for Medicaid and SNAP.
“We are going back to a place of a lot of uncompensated care and a lot of patchwork systems for people to get care,” said Ellen Montz, a managing director at Manatt Health who oversaw the ACA federal marketplace during the Biden administration.
The big picture:
The stakes are huge for low-income and working-class Americans who depend on Medicaid and subsidized ACA coverage.
Without health coverage, more people with diabetes, heart disease, asthma and other chronic conditions will likely go without checkups and medication to keep their ailments in check.
Those who try to keep up with care after losing insurance will pay more out of pocket, driving up medical debt and increasing the risk of eviction, food insecurity and depleted savings.
Uninsured patients have worse cancer survival outcomes and are less likely to get prenatal care. Medicaid also is a major payer of behavioral health counseling and crisis intervention.
Much of the coverage losses from the bill will come from new Medicaid work reporting requirements, congressional scorekeepers predict. Work rules generally will have to be implemented for coverage starting in 2027, but could be earlier or later depending on the state.
Past experiments with Medicaid work rules show that many eligible people fall through the cracks verifying they’ve met the requirements or navigating new state bureaucracies.
Often, people don’t find out they’ve lost coverage until they try to fill a prescription or see their doctor. States typically provide written notices, but contacts can be out of date.
Nearly 1 in 3 adults who were disenrolled from Medicaid after the COVID pandemic found out they no longer had health insurance only when they tried to access care, per a KFF survey.
Zoom out:
The Medicaid and ACA changes will also affect people who keep their coverage.
The anticipated drop-off in preventive care means the uninsured will be more likely to go to the emergency room when they get sick. That could further crowd already bursting ERs, resulting in even longer wait times.
Changes to ACA markets in the bill, along with the impending expiration of enhanced premium subsidies, may drive healthier people to drop out, Montz said, skewing the risk pool and driving up premiums for remaining enrollees.
States will likely have to make further cuts to their safety-net programs if the bill passes in order to keep state budgets functioning with less federal Medicaid funding.
The other side:
The White House and GOP proponents of the bill say the health care changes will fight fraud, waste and abuse, and argue that coverage loss projections are overblown.
Conservative health care thinkers also posit that there isn’t strong enough evidence that public health insurance improves health.
Reality check:
Not all insurance is created equally, and many people with health coverage still struggle to access care. But the bill’s impact would take the focus off ways to improve the health system, Montz said.
“This is taking us catastrophically backward, where we don’t get to think about the things that we should be thinking about how to best keep people healthy,” she said.
The bottom line:
The changes will unfold against a backdrop of Health Secretary Robert F. Kennedy Jr.’s purported focus on preventive care and ending chronic illness in the U.S.
But American health care is an insurance-based system, said Manatt Health’s Patricia Boozang. Coverage is what unlocks access.
Scrapping millions of people’s health coverage “seems inconsistent with the goal of making America healthier,” she said.
Last Thursday, the Make America Healthy Again Commission released its 68-page report “Making America’s Children Healthy Again Assessment” featuring familiar themes—the inadequacy of attention to chronic disease by the health system, the “over-medicalization” of patient care vis a vis prescription medicines et al, the contamination of the food-supply by harmful ingredients, and more.
HHS Secretary Kennedy, EPA Administrator Zeldin and Agriculture Secretary Rollins pledged war on the corporate healthcare system ‘that has failed the public’ and an all-of-government approach to remedies for burgeoning chronic care needs.
Also Thursday, the House of Representatives passed its budget reconciliation bill by a vote of 215-214. The 1000-page bill cuts federal spending by $1.6 trillion (including $698 billion from Medicaid) and adds $2.3 trillion (CBO estimate/$3.4 to $5 trillion per Yale Budget Lab) to the national deficit over the next decade. It now goes to the Senate where changes to reduce federal spending to pre-pandemic level will be the focus.
With a 53-37 advantage and 22 of the 36 Senate seats facing mid-term election races in November, 2026, the Senate Republican version of the “Big Beautiful Bill” will include more spending cuts while pushing more responsibility to states for funding and additional cuts. The gap between the House and Senate versions will be wider than currently anticipated by House Republicans potentially derailing the White House promise of a final Big Beautiful Bill by July 4.
And, over the last week and holiday weekend, the President announced a new 25% tariff on Apple devices manufactured in India and new tariffs targeting the EU; threatened cuts to federal grants to Harvard and cessation of its non-citizen student enrollment, a ‘get-tougher’ policy on Russia to pressure an end of its Ukraine conflict, and a pledge to Americans on Memorial that it will double down on ‘peace thru strength’ in its Make America Great Again campaign.
These have 2 things in common:
1-They’re incomplete. None is a finished product.
The MAHA Commission, working with the Departments of Health & Human Services, Interior and Agriculture, is tasked to produce another report within 90 days to provide more details about a plan. The FY26 budgeting process is wrought with potholes—how to satisfy GOP deficit hawks vs. centrist lawmakers facing mid-term election, how to structure a bill that triggers sequestration cuts to Medicare (projected $490 billion/10 yrs. per CBO), how to quickly implement Medicaid work requirements and marketplace enrollment cuts that could leave insurance coverage for up to 14 million in limbo, and much more. And the President’s propensity to “flood the zone” with headline-grabbing Truth Social tweets, Executive Orders and provocative rhetoric on matters at home and abroad will keep media occupied and healthcare spending in the spotlight.
2-They play to the MAGA core.
The MAGA core is primarily composed of older, white, Christian men driven by a belief that the United States has lost its exceptionalism through WOKE policies i.e. DEI in workplaces and government, open borders, globalization and excessive government spending and control. In the 2024 Presidential election, the MAGA core expanded incrementally among Black, Hispanic, and younger voters whose concerns about food, energy and housing prices prompted higher-than expected turnout. The MAGA core believes in meritocracy, nationalism, smaller government, lower taxes, local control and free-market policies that encourage private investment in the economy. The core is price sensitive.
The health system per se is not a concern but it’s the affordability and lack of price transparency are. They respect doctors and frontline caregivers but think executives are overpaid and prone to self-promotion. And the MAGA core think lawmakers have been complicit in the system’s lack of financial accountability largely beneficial to elites.
Looking ahead to the summer, a “Big Beautiful Bill” will pass with optics that allow supporters to claim fiscal constraint and lower national debt and opponents to decry insensitive spending cuts and class warfare against low-and-middle-class households.
Federal cuts to Medicaid and SNAP (Supplemental Nutrition Assistance Program) will be prominent targets in both groups—one a portrayal of waste, fraud and abuse and the other tangible evidence of societal inequity and lack of moral purpose. Each thinks the other void of a balanced perspective. Each thinks the health system is underperforming and in need of transformational change but agreement about how to get there unclear.
As MAHA promotes its agenda, Congress passes a budget and MAGA advances its anti-establishment agenda vis a vis DOGE et al, healthcare operators will be in limbo. The dust will settle somewhat this summer, but longer-term bets will be modified for most organizations as compliance risks change, state responsibilities expand, capital markets react and Campaign 2026 unfolds.
And in most households, concern about the affordability of medical care will elevate as federal and state funding cuts force higher out of pocket costs on consumers and demand for lower prices.
The summer will be busy for everyone in healthcare.
PS: Changes in the housing market are significant for healthcare: 36% of the CPI is based on shelter vs. 8% for medical services & products, 14% for food and 6% for energy/transportation. While the overall CPI increased 2.3% in the last 12 months, medical services prices increased 3.1%. contributing to heightened price sensitivity and delayed payments.
It has not escaped lawmaker attention: revenue cycle management business practices (debt collection) are being scrutinized in hospitals and community benefit declarations by not-for-profit hospitals re-evaluated. The economics of healthcare are not immune to broader market trends nor is spending for healthcare in households protected from day-to-day fluctuations in prices for other goods and services.
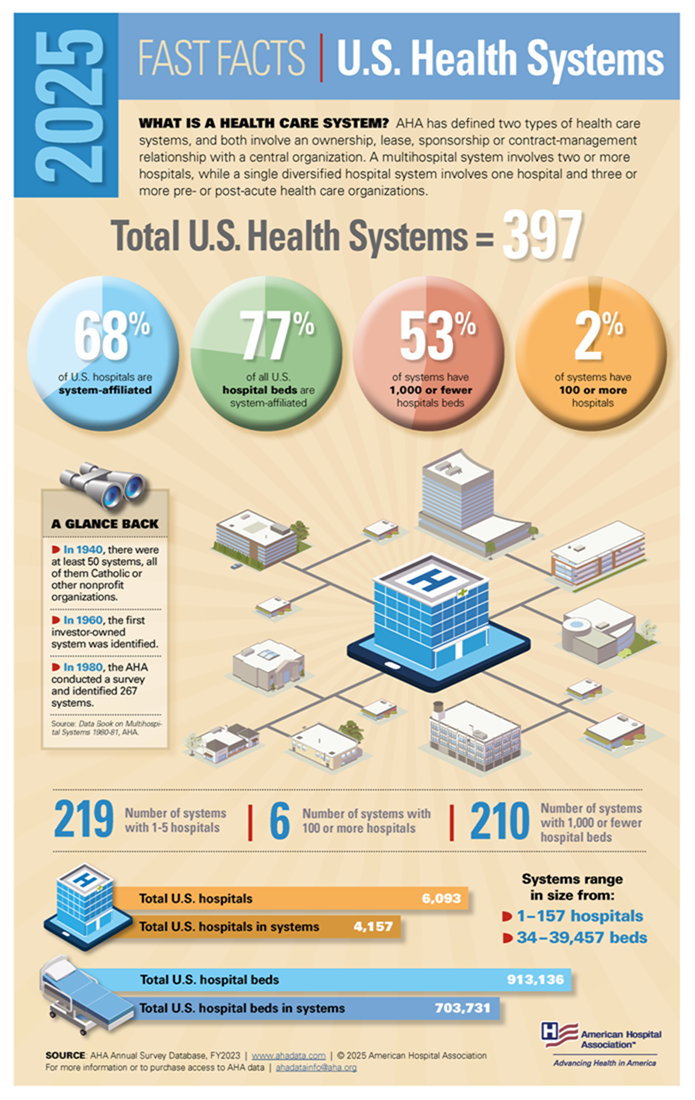
Medicaid is critical to our nation’s healthcare system, providing necessary care for more than 72 million Americans – including our neighbors and friends.
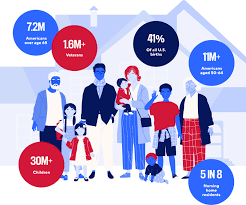
Who it Affects
Medicaid covers children, seniors in nursing homes, veterans, people with long-term chronic illnesses, those with mental health issues and working families.
The program helps keep Americans healthy at all stages of life, providing healthcare to families in need — especially as the country continues to recover from record-high inflation.
The Problem
Some policymakers are considering Medicaid cuts that would undermine coverage for countless patients and threaten Americans’ access to comprehensive, 24/7 hospital care.
Medicaid covers health services for patients who otherwise wouldn’t be able to pay for care. Coverage of services is essential for hospitals, and helps ensure all Americans have access to high-quality, 24/7 care, no matter where they live.
Who Medicaid covers
Providing Lifesaving Healthcare Services
Medicaid covers patients with complex and chronic illnesses in need of long-term care, as well as emergency services and prescription coverage.
As the nation faces a growing mental health crisis, Medicaid also ensures millions of Americans — including veterans — have access to mental healthcare and substance abuse services.
Without access to affordable mental healthcare through Medicaid, veterans often lack the long-term support they deserve, and are left to deal with complex health issues years after their service.
In these areas, where primary care providers are few and far between, hospitals become even more vital sites of care — and in some cases, the only sites of care available.
Rural hospitals, already more likely to be at risk of closure, rely on Medicaid funding to stay open and to continue providing lifesaving care to their patients. Nearly 150 rural hospitals have closed or converted since 2010 alone. Further cuts to care would eliminate a lifeline for Americans across the country — with devastating consequences for rural communities.
The Solution
Cuts to Medicaid funding will create irreparable harm for our nation’s most vulnerable communities, including millions of children, veterans, those with chronic illnesses, seniors in nursing homes, and working families. Medicaid helps provide security to these Americans, keeping them healthy at every stage of life.
Congress should vote against efforts to reduce Medicaid funding and instead focus on policies that strengthen access to 24/7 care, rather than take it away.
Most Americans believe their healthcare is private, and the majority prefers it that way. Gallup polling shows more Americans favor a system based on private insurance rather than government-run healthcare.
But here’s a surprising reality: 91% of Americans receive government-subsidized healthcare.
Unless you’re among the uninsured or the few who receive no subsidies, government dollars are helping pay your medical bills — whether your insurance comes from an employer, a privately managed care organization or the online marketplace.
Now, as lawmakers face mounting budget pressures, those subsidies (and your coverage) could be at risk. If the government scales back its healthcare spending, your medical costs could skyrocket.
Here’s a closer look at the five ways the U.S. government funds healthcare. If you have health insurance, you’re almost certainly benefiting from one of them:
Medicare, the government-run healthcare program for those 65 and older, covers 67 million Americans at a cost of more than $1 trillion annually. Approximately half of enrollees are covered through the traditional fee-for-service plan and the other half in privately managed Medicare Advantage plans.
Medicaid and CHIP provide health coverage for around 80 million low-income and disabled Americans, including tens of millions of children. Even though 41 states have turned over their Medicaid programs over to privately managed care organizations, the cost remains public. Total Medicaid spending is $900 billion annually — the federal government pays 70% with states footing the rest.
The online healthcare marketplace is for Americans whose employer doesn’t provide medical coverage or who are self-employed. This Affordable Care Act program offers federal subsidies to 92% of its 23 million enrollees, which help lower the cost of premiums and, for many, subsidize their out-of-pocket expenses. The Congressional Budget Office projects that a permanent extension of these subsidies, which are scheduled to end this year, would cost $383 billion over the next 10 years.
Veterans and military families also benefit from government healthcare through TRICARE and VA Care, programs covering roughly 16 million individuals at a combined cost of $148 billion for the federal government annually.
Employer-sponsored health insurance comes with a significant, yet often overlooked, government subsidy. For nearly 165 million American workers and their families, U.S. companies pay the majority of their health insurance premiums. However, those dollars are excluded from employees’ taxable income. This tax break, which originated during World War II and was formally codified in the 1950s, subsidizes workers at an annual government cost of approximately $300 billion. For a typical family of four, this translates into approximately $8,000 per year of added take-home pay.
With 91% of Americans receiving some form of government healthcare assistance, the idea that U.S. healthcare is predominantly “private” is an illusion.
Now, as the new administration searches for ways to rein in the growing federal deficit, all five of these programs (collectively funding healthcare for 9 in 10 Americans) will be in the crosshairs.
Twelve percent of the federal budget already goes toward debt interest payments, and this share is expected to rise sharply. Many of the bonds used to finance existing debt were issued back when interest rates were much lower. As those bonds mature and are refinanced at today’s higher rates, federal interest payments are projected to double within the next decade, according to the Congressional Budget Office.
With deficits mounting and borrowing costs soaring, most economists agree this trajectory is unsustainable. Lawmakers will eventually need to rein in spending, and healthcare subsidies will almost certainly be among the first targets. Policy experts predict Medicaid, which the House has already proposed cutting by $880 billion over the next decade, and ACA subsidies for out-of-pocket costs will likely be the first on the chopping block. But given the CBO’s projections, these cuts won’t be the last.
A Better Way: Three Solutions To Lower Healthcare Costs Without Cuts
Cutting some or all of these healthcare subsidies may seem like the simplest way to reduce the deficit. In reality, it merely shifts costs elsewhere, making medical care more expensive for everyone and increasing future government spending. Here’s why:
Eliminating subsidies doesn’t eliminate the need for care. Under the Emergency Medical Treatment and Labor Act (EMTALA), hospitals must treat emergency patients regardless of their ability to pay. When millions lose insurance, more turn to ERs for medical care they can’t afford. The cost of that uncompensated care doesn’t vanish. It gets passed on to state governments, hospitals and privately insured patients through higher taxes, inflated hospital bills and rising insurance premiums.
Delaying care drives up long-term costs. People who can’t afford doctor visits skip preventive care, screenings and early treatments. Manageable conditions like high blood pressure and diabetes then spiral into costly, life-threatening complications including heart attacks, strokes and kidney failures, which ultimately increase government spending.
The solution isn’t cutting coverage. It’s fixing the root causes of high healthcare costs. Here are three ways to achieve this:
1. Address The Obesity Epidemic
Obesity is a leading driver of diabetes, heart disease, stroke and breast cancer, which kill millions of Americans and cost the U.S. healthcare system hundreds of billions annually. Congress can take two immediate steps to reverse this crisis:
Tax high-calorie, highly processed foods and use the revenue to subsidize healthier options, making nutritious food more affordable for all Americans.
2. Enhance Chronic Disease Management With Technology
In every other industry, broad adoption of generative AI technology is already increasing quality while reducing costs. Healthcare could do the same by applying generative AI to more effectively manage chronic disease. According to the Centers for Disease Control and Prevention, improved control of these lifelong conditions could cut the frequency of heart attacks, strokes, kidney failures and cancers by up to 50%.
With swift and reasonable Food and Drug Administration approval, generative AI and wearable monitors would revolutionize how these conditions are managed, providing real-time updates on patient health and identifying when medications need adjustment. Instead of waiting months for their next in-office visit, patients with chronic diseases would receive continuous monitoring, preventing costly and life-threatening complications. Rather than restricting AI’s role in healthcare, Congress can streamline the FDA’s approval process and allocate National Institutes of Health funding to accelerate these advancements.
3. Reform Healthcare Payment Models
Under today’s fee-for-service system, doctors and hospitals are paid based on the how often they see patients for the same problem and the number of procedures performed. This approach rewards the volume of care, not the best and most effective treatments. A better alternative is a pay-for-value model like capitation, in which providers do best financially when they help keep patients healthy. To encourage participation, Congress should fund pilot programs and create financial incentives for insurers, doctors and hospitals willing to transition to this system. By aligning financial incentives with long-term health, this model would encourage doctors to prioritize prevention and effective chronic disease control, ultimately lowering medical costs by improving overall health.
The Time For Change Is Now
If Congress slashes healthcare subsidies this year, restoring them will be nearly impossible. Once the cuts take effect, the financial and political pressures driving them will only intensify, making reversal unlikely.
The voices shaping this debate can’t come solely from industry lobbyists. Elected officials need to hear from the 91% of Americans who rely on government healthcare assistance for some or all of their medical coverage. Now is the time to speak up.
Regular readers know I’ve long been curious about the forces driving one essential question in healthcare today:
Why is it so hard to run a hospital now? One area worth exploring is the interplay between the healthcare system and our nation’s changing demographics.
Baby Boomers have been displaced as the largest generation of adults in America.Millennialsnow hold that position, and Gen Z will likely outnumber Baby Boomers in the workplace sometime this year. Our nation is rapidly diversifying, as more than two-fifths of Americans identify as people of color.
It’s not just a matter of who we are as a nation that’s changing; how we live is evolving, too. The number of 40-year-olds who’ve never been married reached record highs in 2022, according to the Pew Research Center, dovetailing with a steadily growing trend since 1970 toward single living.
The U.S. Census published a report earlier this year showing that nearly 29% of American households include only one person. Further, the U.S. fertility rate is at an all-time low — and, according to a Pew survey, may not recover, given that 47% of those under 50 said they were unlikely to have children. That’s an increase of 10 percentage points since 2018.
The effects of this are starting to shape our broader culture. Solo living has been cited as a contributing factor to the housing crisis, and we’re starting to hear more about how people are grappling with the practical implications of retiring while living alone. This column in The New York Times is just one example.
As for the potential health effects of living alone, in 2023, U.S. Surgeon General Vivek Murthy raised an alarm with a report documenting the negative effects of social isolation on individual and public health. Murthy outlined a host of risks, including cardiovascular disease, hypertension, diabetes and increased susceptibility to infectious disease. Mental health is a major concern. A 2024 study published in National Health Statistics Reports found that people who live alone were more likely to be depressed, particularly if they lacked social or emotional support.
All of this adds up to an increasing burden on the U.S. healthcare system.
As providers who care for the socially isolated already know, it’s impossible to operate as usual if a patient lacks family support. Hospitals and the traditional American family structure are fundamentally intertwined. When family support is not available for a medical emergency, then the entire hospital episode becomes more fragile. Patient discharge procedures assume someone is available at home to help with care, assist in transporting patients for follow-up visits, and engage with the business office around billing and insurance.
Without this family safety net, the potential for readmission rises, harming patient outcomes, increasing costs and putting quality ratings at risk. The rise in younger people living alone also raises further financial implications, given that about 45% of Americans access health insurance through employer-sponsored programs. If someone living alone becomes too sick to work, patients may be less able to pay for care when they need it most.
This is just another in a long list of challenging hospital operational dilemmas. How best to respond to such profound change in the American demographic landscape? The right strategy may be to re-think consumer segmentation.
Consumer segmentation has become very popular at the clinical product level, but perhaps the next level of service segmentation is not among disease types but based on demographic characteristics.
As an increasing portion of the American population has less family support to navigate a hospital stay or chronic illness, it will become more important to identify these patients and determine which new and enhanced services need to be provided to them by the hospital. Social work programs will need to be more robust, and health systems should invest in community partnerships to help bridge the resource gap. But the wide-ranging nature of patients’ practical needs will likely require healthcare leaders to think creatively.
Consider the scope:
Care coordinators: Particularly for patients with complex conditions, it may be beneficial to designate a care coordinator to oversee healthcare planning.
Home health care: Without family members to help with day-to-day care, more nurses and aides will be needed to provide healthcare at home as well as help with day-to-day living. For patients with less demanding healthcare needs, adult day care may be useful.
Medication management: Patients need to understand how to take their medications, watch for potential side effects and interactions, and develop a system to make sure they take them on time. Further, they may need help navigating the pharmacy, either in getting prescriptions filled or with financial assistance programs.
Meal delivery: Nutrition is vital to a patient’s recovery, and ensuring patients have access to healthy options can help to reduce the likelihood of readmission.
Personal emergency response systems: Patients may need devices to call for help during an emergency as well as medical bracelets or other methods for communicating important information to first responders.
Housekeeping assistance: Hospitals may need to help connect patients with resources to maintain clean, safe homes.
Volunteer companions: While volunteer companions usually help elderly patients with social interaction and basic needs, it may be necessary to develop programs that target a wider range of ages.
Transportation services: Patients need help getting to and from follow-up visits.
Telehealth: Remote care will become increasingly important. Clinical services should consider whether care plans could be adjusted to reduce the number of in-person visits.
Beyond targeting resources, consumer segmentation also offers an opportunity to communicate with patients in a more effective and personalized way. This sort of engagement fosters trust and increases loyalty that’s particularly important, given the intimate nature of healthcare.
It’s long been true that the stronger the family system, the better off hospitals are. But as the concept of the American family shifts, and in this case, unwinds, healthcare leaders need to be attuned to new demands—and nimble enough to meet them. This requires making the most of the information you have today to plan for tomorrow.
Clinician burnout is a major problem. However, as I pointed out in a previous newsletter post, it is not a distinctly American problem.
A recent report from the Commonwealth Fund compared the satisfaction of primary care physicians in 10 high-income nations. Surprisingly, U.S. doctors ranked in the middle, reporting higher satisfaction rates than their counterparts in the U.K., Germany, Canada, Australia and New Zealand.
A Surprising Insight About Burnout
In self-reported surveys, American doctors link their dissatisfaction to problems unique to the U.S. healthcare system: excessive bureaucratic tasks, clunky computer systems and for-profit health insurance. These problems need to be solved, but to reduce clinician burnout we also need to address another factor that negatively impacts doctors around the globe.
Though national healthcare systems may vary greatly in their structure and financing, clinicians in wealthy nations all struggle to meet the ever-growing demand for medical services. And that’s due to the mounting prevalence and complications of chronic disease.
At the heart of the burnout crisis lies a fundamental imbalance between the volume and complexity of patient health problems (demand) and the amount of time that clinicians have to care for them (supply). This article offers a way to reverse both the surge in chronic illnesses and the ongoing clinician burnout crisis.
Supply vs. Demand: Reframing Burnout
When demand for healthcare exceeds doctors’ capacity to provide it, one might assume the easiest solution is to increase the supply of clinicians. But that outcome remains unlikely so long as the cost increases of U.S. medicine continue to outpace Americans’ ability to afford care.
Whenever healthcare costs exceed available funds, policymakers and healthcare commentators look to rationing. The Oregon Medicaid experiment of the 1990s offers a profound reminder of why this approach fails. Starting in 1989, a government taskforce brought patients and providers together to rank medical services by necessity. The plan was to provide only as many as funding would allow. When the plan rolled out, public backlash forced the state to retreat. They expanded the total services covered, driving costs back up without any improvement in health or any relief for clinicians.
Consumer Culture Can Drive Medical Culture
Ultimately, to reduce burnout, we will have to find a way to decrease clinical demand without raising costs or rationing care.
The best—and perhaps only viable—solution is to embrace technologies that empower patients with the ability to better manage their own medical problems.
American consumers today expect and demanded greater control over their lives and daily decisions. Time and again, technology has made this possible.
Take stock trading, for example. Once the sole domain of professional brokers and financial advisors, today’s online trading platforms give individual investors direct access to the market and a wealth of information to make prudent financial decisions. Likewise, technology transformed the travel industry. Sites like Airbnb and Expedia empowered consumers to book accommodations, flights and travel experiences directly, bypassing traditional travel agents.
Technology will soon democratize medical expertise, as well, giving patients unprecedented access to healthcare tools and knowledge. Within the next five to 10 years, as ChatGPT and other generative AI applications become significantly more powerful and reliable, patients will gain the ability to self-diagnose, understand their diseases and make informed clinical decisions.
Today, clinicians are justifiably skeptical of outsized AI promises. But as technology proves itself worthy, clinicians who embrace and promote patient empowerment will not only improve medical outcomes, but also increase their own professional satisfaction.
Here’s how it can happen:
Empowering Patients With Generative AI
In the United States, health systems (i.e., large hospitals and medical groups) that heavily prioritize preventive medicine and chronic-disease management are home to healthier patients and more satisfied clinicians.
In these settings, patients are 30% to 50% less likely to die from heart attack, stroke and colon cancer than patients in the rest of the nation. That’s because their healthcare organizations provide effective chronic-disease prevention programs and assist patients in managing their diabetes, hypertension, obesity and asthma. As a result, patients experience fewer complications like heart attacks, strokes, and cancer.
Most primary care physicians, however, don’t have the time to accomplish this by themselves. According to one study, physicians would need to work 26.7 hours per day to provide all the recommended preventive, chronic and acute care to a typical panel of 2,500 adult patients.
GenAI technologies like ChatGPT can help lessen the load. Soon, they’ll be able to offer patients more than just general advice about their chronic illnesses. They will give personalized health guidance. By connecting to electronic health records (EHR)—even when those systems are spread across different doctors’ offices—GenAI will be able to analyze a patient’s specific health data to provide tailored prevention recommendations. It will be able to remind patients when they need a health screening, and help schedule it, and even sort out transportation. That’s not something Google or any other online platform can currently do.
Moreover, with new tools (like doctor-designed plugins expected in future ChatGPT updates) and data from fitness trackers and home health monitors, GenAI will be capable of not just displaying patient health data, but also interpreting it in the context of each person’s health history and treatment plans. These tools will be able to provide daily updates to patients with chronic conditions, telling them how they’re doing based on their doctor’s plan.
When the patient’s health data show they’re on the right track, there won’t be a need for an office visit, saving time for everyone. But if something seems off—say, blood pressure readings remain excessively high after the start of anti-hypertensive drugs—clinicians will be able to quickly adjust medications, often without the patient needing to come in. And when in-person visits are necessary, GenAI will summarize patient health information so the doctor can quickly understand and act, rather than starting from scratch.
ChatGPT is already helping people make better lifestyle choices, suggesting diets tailored to individual health needs, complete with shopping lists and recipes. It also offers personalized exercise routines and advice on mental well-being.
Another way generative AI can help is by diagnosing and treating common, non-life-threatening medical problems (e.g., musculoskeletal, allergic or viral issues). ChatGPT and Med-PaLM 2 have already demonstrated the capability in diagnosing a range of clinical issues as effectively and safely as most clinicians. Looking ahead, GenAI’s will offer even greater diagnostic accuracy. When symptoms are worrisome, GenAI will alert patients, speeding up definitive treatment. Its ability to thoroughly analyze symptoms and ask detailed questions without the time pressure doctors feel today will eradicate many of our nation’s 400,000 annual deaths from misdiagnosis.
The outcomes—fewer chronic diseases, fewer heart attacks and strokes and more medical problems solved without an office visit—will decrease demand, giving doctors more time with the patients they see. As a result, clinicians will leave the office feeling more fulfilled and less exhausted at the end of the day.
The goal of enhanced technology use isn’t to eliminate doctors. It’s to give them the time they desperately need in their daily practice, without further increasing already unaffordable medical costs. And rather than eroding the physician-patient bond, the AI-empowered patient will strengthen it, since clinicians will have the time to dive deeper into complex issues when people come to the office.
A More Empowered Patient Is Key To Reducing Burnout
AI startups are working hard to create tools that assist physicians with all sorts of tasks: EHR data entry, organizing office duties and submitting prior authorization requests to insurance companies.
These function will help clinicians in the short run. But any tool that fails to solve the imbalance between supply (of clinician time) and demand (for medical services), will be nothing more than a temporary fix.
Our nation is caught in a vicious cycle of rising healthcare demand, leading to more patient visits per day per doctor, producing higher rates of burnout, poorer clinical outcomes and ever-higher demand. By empowering patients with GenAI, we can start a virtuous cycle in which technology reduces the strain on doctors, allowing them to spend more time with patients who need it most. This will lead to better health outcomes, less burnout for clinicians and further decreases in overall healthcare demand.
Physicians and medical societies have the opportunity to take the lead. They’ll have to educate the public on how to use this technology effectively, assist in connecting it to existing data sources and ensure that the recommendations it makes are reliable and safe. The time to start this process is now.
Published this week in the Washington Post, this unsparing article packages a year of investigative reporting into a thorough accounting of why US life expectancy is undergoing a rapid decline.
After peaking in 2014, US life expectancy has declined each subsequent year, trending far worse than peer countries. In a quarter of US counties, working-age Americans are dying at the highest rates in 40 years, reversing decades of progress. While deaths from firearms and opioids play a role, chronic diseases remain our nation’s greatest killer, erasing more than double the years of life as all overdoses, homicides, suicides, and car accidents combined.
The drivers of this trend are too numerous to list, but experts suggest targeting “the causes of the causes”, namely social factors, as the death rate gap between the rich and poor has grown almost 15x faster than the income gap since 1980.
The Gist: This reporting is a sobering reminder of the responsibilities—and failures—borne by our nation’s healthcare system.
The massive death toll of chronic disease in this country is not an indictment of the care Americans receive, but of the care and other resources they cannot access or afford.
While it’s not the mandate of health systems to reduce systemic issues like poverty, there is no solution to the problem without health systems playing a key role in increasing access to care, while convening community resources in service of these larger goals.
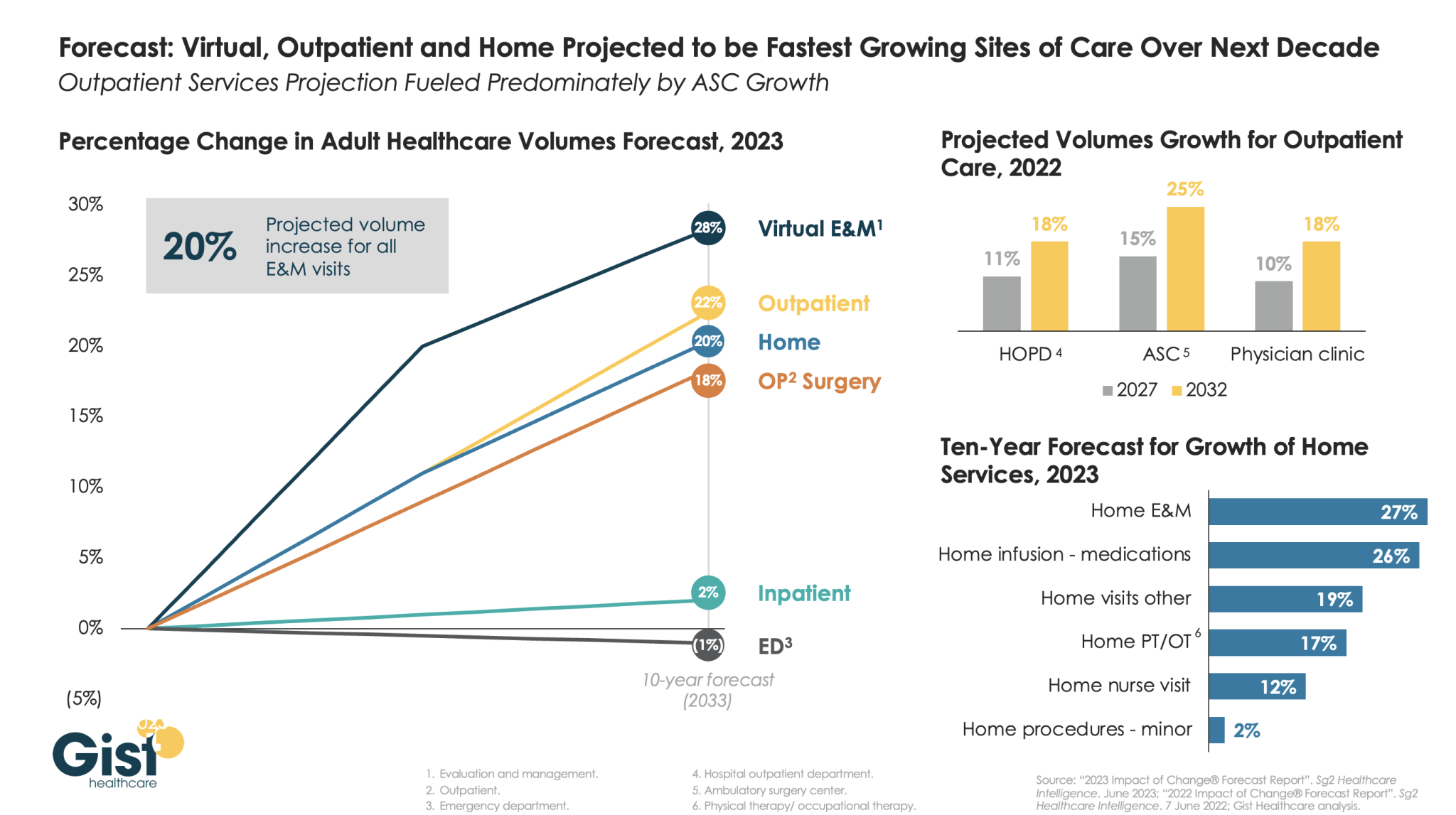
The pandemic accelerated the outpatient shift, which had been progressing steadily for decades, into a new gear, as safety-minded consumers avoided inpatient settings.
Using the latest forecasting data from strategic healthcare consulting firm Sg2, the graphic above illustrates how the outpatient shift will continue to accelerate in the coming years. With each projected to grow by 20 percent or more, outpatient, virtual, and home-based care services will continue far outpace growth in hospital-based care over the next decade.
Ambulatory surgery centers (ASCs) will be at the center of this care shift, reflected by a projected 25 percent rise in ASC volumes by 2032.
The breadth of care available at home will also expand as care delivery technology improves. With the population becoming older and sicker, higher incidence of chronic disease will be met by a rapid expansion of home evaluation and management services (E&M),reflecting a shift away from hospitals and doctors’ offices as hubs for complex care management.
Instead, the patients still coming to hospitals will present with increasingly acute conditions, driving up demand for resource-intensive critical care, as broader inpatient volume remains relatively flat.
At a recent meeting of physician leaders, we sat next to the head of the health system’s bariatric surgery program. Given the recent and rapid uptake of GLP-1 inhibitors like Ozempic and Wegovy, we asked how he thought these drugs, which can generate dramatic weight loss, would affect his practice.
He chuckled, “they’re really good drugs…they could put me out of business!
It’s too early to say if they’ll be effective over a lifetime, but there’s no doubt they’re going to have a huge impact on our work.” It got us thinking about the other reverberations this class of drugs could have on care needs, if a majority of obese Americans had access to them.
Some effects are obvious.
We could see significant declines in treatment needs for chronic diseases like obesity and heart failure, for which obesity is a strong risk factor. Given that obese patients are much more likely to need joint replacement surgery, we could see a big hit to that demand—although some patients who are poor candidates for surgery because of weight-related complications could become eligible.
Even longer-term, if American’s aren’t dying of chronic disease, we’ll still die of something, so expect diseases of advanced age, like Alzheimer’s and many cancers, to increase. Other pharmaceutical innovations, like the growth of immunotherapy and more targeted cancer treatments, also have the potential to radically alter how disease is managed.
We may be at the beginning of another wave of disruptive medical innovation on the order of the introduction of statins in the 1990s, which combined with minimally invasive catheterization, slashed the need for bypass surgery.
Given their sky-high prices, it’s too soon to tell how quickly the use of these new obesity drugs will grow, but innovations like these will serve to pull more care out of hospitals and into less invasive outpatient medical management.
As happened with cars in the 1960s, price competition among brand-name drugs is hard to find.
Before 1973, when the Arab oil embargo upended the U.S. auto industry, Americans witnessed an annual ritual by carmakers. In the late summer, the Big Three — Ford, Chrysler, and General Motors — would release sticker prices for their products, always showing increases, of course.
Almost always, the increases from each company for similar models were nearly identical. If one company’s was out of line — substantially bigger or smaller than its erstwhile competitors’ — it quickly made an adjustment. Explicit collusion to fix prices was never proven, but the effect for consumers was the same.
Now, researchers report that something very similar seems to be occurring for big-market brand-name drugs, including anti-diabetic medications and blood thinners.
Average wholesale prices for products in five classes — direct-acting oral anticoagulants (DOACs), P2Y12 inhibitors, glucagon-like peptide-1 (GLP-1) agonists, dipeptidyl dipeptidase-4 (DPP-4) inhibitors, and sodium-glucose transport protein-2 (SGLT-2) inhibitors — increased in “lock-step” each year from 2015 to 2020, according to Joseph Ross, MD, of Yale University in New Haven, Connecticut, and colleagues writing in JAMA Network Open.
These increases ranged from annual averages of 6.6% for DDP4 inhibitors to 13.5% for P2Y12 inhibitors — far outpacing not only inflation in general, but even the 2.1% average for all prescription drugs.
Within each class, Kendall τb correlation coefficients for average wholesale prices were as follows:
DOACs: 0.98
SGLT-2 inhibitors: 0.98
DPP-4 inhibitors: 0.96
GLP-1 agonists: 0.92
P2Y12 inhibitors: 0.75
“These results suggest there was little price competition among the sponsors of these products,” Ross and colleagues wrote.
Although the analysis came with significant limitations — it didn’t account for rebates or other discounts, for example — the researchers said some patients must suffer from these increases.
“Rebates, list prices, and net prices have been growing for brand-name medications, and rebate growth has been shown to positively correlate with list price growth, thereby impacting costs faced by patients paying a percentage of (or the full) list price,“ the group noted. “Therefore, the lock-step price increases of brand-name medications, without evidence of price competition, raise concerns and would be expected to adversely affect patient adherence to medications and thus clinical outcomes.”
For the car buyers, the solution to lock-step price increases was imposed from outside: soaring gas prices in the mid-1970s prompted demand for vehicles with better fuel economy than domestic makers were prepared to sell. That opened the market to Japanese cars that not only got better mileage, but were also more reliable and (in many cases) cheaper than Big Three products. Thus ended Detroit’s ability to set prices.
How to rein in Big Pharma is less clear. For their part, Ross and colleagues suggested policies to limit such lock-step price hikes, shortened patent exclusivity periods, and faster introduction of generic equivalents.