Providence, a 52-hospital system based in Renton, Wash., saw its operating loss hit $221.9 million in the first quarter, compared to an operating loss of $276.2 million recorded in the first quarter of 2020, according to financial documents released May 17.
“We’re turning a corner and seeing signs of renewal,” said Rod Hochman, MD, president and CEO of Providence. “Throughout this crisis, the caregivers of Providence have stepped up to respond to the needs of our communities, and we are incredibly grateful to everyone who has been serving on or supporting the front lines of care.”
The health system recorded revenue of $6.4 billion in the quarter ended March 31, up 1.6 percent from the same period in 2020. Providence said the growth was driven by 9 percent growth in capitation revenue and 57 percent growth in diversified revenue.
Operating expenses reached $6.7 billion in the first quarter, an increase of 1 percent from the same period last year. Providence said the expense increase was driven by costs to support caregivers and to serve patients, including labor and more personal protective gear and drugs.
After factoring in $306.5 million in nonoperating income, Providence ended the quarter with a net income of $84.6 million. In the same period last year, Providence recorded a net loss of $1.1 billion. Last year’s net loss was largely attributed to negative financial market forces.
Three Ascension hospitals in Texas agreed to pay $20.9 million for allegedly paying multiple physician groups above fair market value for services, according to a recent news release from the HHS’ Office of Inspector General.
The three Texas hospitals are Ascension’s Dell Seton Medical Center in Austin, Ascension Seton Medical Center Austin and Ascension Seton Williamson in Roundrock. Ascension self-disclosed the conduct to the inspector general.
The hospitals allegedly violated the Civil Monetary Penalties Law, including provisions related to physician self-referrals and kickbacks in seven instances, according to the April 30 news release.
Some of the allegations the report outlined include Dell Seton paying an Austin physician practice above fair market value for on-call coverage; Ascension Seton Austin paying an Austin practice above fair market value for transplant on-call coverage and administrative services; and Ascension Seton Williamson paying a practice above fair market value to lease the practice’s employed registered nurses and surgical technologists who assisted in surgeries at the hospital.
The release did not disclose the physician groups allegedly involved.
After posting a $1.4 billion net loss in the third quarter of fiscal year 2020, CommonSpirit, a 140-hospital system based in Chicago, saw improved finances in the third quarter of fiscal year 2021, according to financial documents released May 14.
CommonSpirit, formed in 2019 through the merger of San Francisco-based Dignity Health and Englewood, Colo.-based Catholic Health Initiatives, reported revenues of $8.8 billion in the third quarter of fiscal 2021, up from $7.8 billion recorded in the same quarter one year prior. The health system said the third quarter of fiscal 2021 was the first period to fully include results from Virginia Mason Fransican Health, an 11-hospital system that was formed in January and joined the CommonSpirit network.
The health system’s operating expenses also increased year over year. It reported total expenses of $8.3 billion in the third quarter of fiscal 2021, compared to about $8 billion recorded in the same period last year.
CommonSpirit ended the third quarter of fiscal 2021 with an operating income of $539 million, a figure that included federal relief aid and a pre-tax gain on the sale of joint venture shares. CommonSpirit said without the aid and pre-tax gain, the health system would have posted an operating loss of $117 million in the quarter ended March 31, “highlighting the continuing concerns around overall patient volumes and the ongoing impact of the pandemic.”
After factoring in $1.2 billion in non-operating income, including $636 million in investment income, CommonSpirit posted a net income of $1.7 billion in the quarter ending March 31. In the same quarter one year prior, CommonSpirit recorded a net loss of $1.5 billion.
“In many ways this quarter was similar to what we experienced over the last year, with a very challenging period followed by a robust recovery,” said CommonSpirit CFO Dan Morissette in a May 14 news release. “With vaccination rates rising and many people returning to their pre-pandemic routines, we expect to continue a strong path to recovery, while also recognizing that we will likely see operational impacts from the pandemic for quite some time.”
CommonSpirit said it also is working to strengthen its financial foundation by realizing operational synergies this year. The goal is to realize $350 million to $400 million in savings during fiscal 2021, and it is on track to meet or surpass that goal.
As we’ve talked to health system executives about the challenges of rolling out COVID vaccines in their communities, one topic keeps coming up: how difficult it’s been to get hospitals’ own workers fully vaccinated. One system told us recently that only 55 percent of their frontline caregivers have opted to get vaccinated, despite early and easy availability, and ongoing encouragement from the hospital’s leaders.
Healthcare workers, it turns out, are just like the general population, bringing the same diversity of perspectives and concerns about vaccination to work with them from their own communities. Vaccine hesitancy is not a new issue for hospital staffers; getting the workforce to take the flu vaccine is an annual struggle for many hospitals.
But given the risks of COVID-19, why not just mandate that hospital employees get the vaccine, as other employers have started to do? We commonly hear two concerns.
One is a labor relations worry: will mandating vaccination cause workers to quit, or make it harder to hire staff in an already difficult market for talent? And given growing concerns about unionization of healthcare workers, will mandatory vaccination become a flashpoint issue?
The second concern is medical liability: can we force workers to get a vaccine that hasn’t been fully approved by the FDA? Would that expose the hospital to legal challenges down the road, if there turn out to be long-term complications from the vaccine?
Our own view is that the first concern is overblown—we suspect vaccine mandates are going to become more and more common as the economy reopens. As to the second, we’re more sympathetic. But once the FDA does grant full approval for the vaccines, we’d hope hospitals will get tougher about vaccine mandates (with the necessary exemptions for health, religious, and other concerns).
At the end of the day, hospitals are in the patient care business, and they should view vaccine mandates—whether for COVID or for influenza—as a patient safety issue, not a workforce engagement issue.
Though consumers say they’re increasingly confident in returning to healthcare settings, hospital volume is not returning with the same momentum across the board. Using the most recent data from analytics firm Strata Decision Technology, covering the first quarter of this year, the graphic above shows that observation, inpatient, and emergency department volumes all remain below pre-COVID levels.
Consumers are still most wary about returning to the emergency department, with volume down nearly 20 percent across the past year. Meanwhile, hospital outpatient visits rebounded quickly, and have been growing steadily month over month, finishing March 2021 at 36 percent above the 2019 level.
Meanwhile, a recent report from the Commonwealth Fund shows that no ambulatory specialty fully made up for the COVID volume hit by the end of last year. But some areas, including rheumatology, urology, and adult primary care, have bounced back faster than others.
With continued success in rolling out vaccines and reducing COVID cases, we’d expect a continued recovery of most hospital visit volume. It may be, however, that some areas, such as the emergency department, will never fully recover to pre-COVID levels. To the extent those visits are now being replaced by more appropriate telemedicine and urgent care utilization, that’s welcome news.
But the continued lag of inpatient admissions indicates that some of the loss of emergency volume is more worrisome—warranting continued efforts on the part of providers to reassure patients it’s safe to use healthcare services. Stay tuned as our team continues to dig into this data.
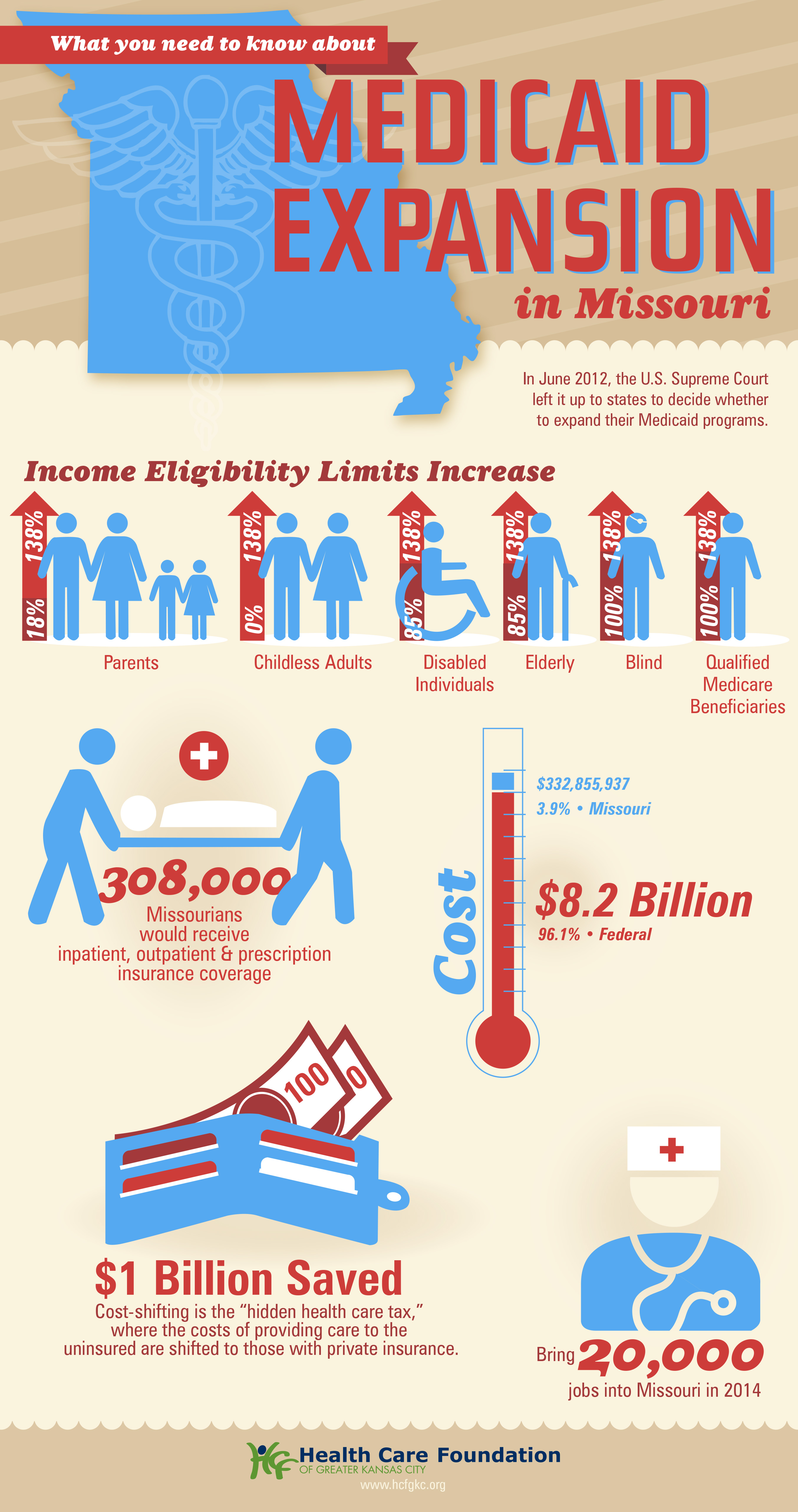
Missouri Gov. Mike Parson announced Thursday that his state would not expand Medicaid coverage to 275,000 residents who will become eligible on July 1st, despite a 2020 ballot initiative in which a majority of the state’s voters approved the expansion. Because the Missouri legislature has blocked funding for the expansion, Parson declared that the state’s Medicaid program, MO HealthNet, would run out of money if it moved forward.
The legislature’s decision to block funding was bolstered by an appeals court opinion last year, which challenged the expansion because the ballot initiative did not include a funding mechanism for widening coverage.
Under the Affordable Care Act (ACA), the federal government would have picked up 90 percent of the cost of expanding Medicaid in the state, in addition to boosting funding for existing Medicaid enrollees by 5 percent, thanks to a measure in the recent American Rescue Plan Act.
The governor’s decision leaves in place one of the strictest Medicaid eligibility standards in the nation: a family of three in Missouri must earn less than 21 percent of the federal poverty level—$5,400 per year—in order to qualify for coverage. The expansion measure would have opened the program to childless adults, and raised the eligibility limit to 138 percent of the federal poverty level.
The Missouri Hospital Association called the decision an “affront” to voters, pointing out that the state is currently running a budget surplus, and could easily allocate funds for the expansion. The status of Medicaid expansion in Missouri, which would become the 38th state to undertake expansion since the ACA’s passage, will ultimately be decided by court ruling, according to observers.
Meanwhile, like other states (mostly in the Southeast) that have resisted Medicaid expansion,Missouri will continue to see tax dollars flow out of the state to fund benefits in states that have expanded eligibility—despite the express will of voters. Given ample evidence that Medicaid expansion boosts access to care, health status, and health system sustainability,it’s nearly unfathomable that the politics of “Obamacare” continue to complicate the extension of this critical safety-net program.
Johns Hopkins University and Johns Hopkins Health System, both based in Baltimore, are boosting their minimum wage to $15 per hour, they said May 6.
The change will take effect July 1, in accordance with annual pay increases for university employees. For health system employees, including more than 300 at Johns Hopkins All Children’s Hospital in St. Petersburg, Fla., the change will take effect Jan. 1.
“Moving to a $15 minimum wage recognizes the hard work and sacrifices Hopkins employees make every day to advance our mission and serve our patients,” Johns Hopkins Health System President Kevin Sowers said in a news release. “We are proud to announce our adoption of a $15 per hour minimum wage even sooner than planned.”
Johns Hopkins said the minimum wage boost includes full-time temporary workers, student workers and contract employees.
Overall, the increase affects more than 6,000 Maryland workers, in addition to the more than 300 Johns Hopkins All Children’s workers in Florida.
Hospitals lost 5,800 jobs in April, marking the fourth month of job loss this year, according to the latest jobs report from the U.S. Bureau of Labor Statistics.
Overall, healthcare lost 4,100 jobs last month — compared to 11,500 jobs added in March — and employment in the industry is down by 542,000 since February 2020.
Within ambulatory healthcare services, dentist offices saw 3,700 added jobs; physician offices saw 11,300 job gains; and home healthcare services lost 6,700 jobs in April.
Nursing and residential care facilities lost 19,500 jobs last month, compared to 3,200 jobs lost the month prior.
The U.S. gained 266,000 in April after gaining 916,000 jobs in March. The unemployment rate was 6.1 percent last month, compared to 6 percent in March.
Trenton, N.J.-based St. Francis Medical Center, owned by Trinity Health, has signed a letter of intent to explore joining Pennington, N.J.-based Capital Health.
With the letter of intent signed, the two organizations enter a period of due diligence. The process will determine how best to combine and serve the community.
The deal would require approval from state and federal officials. Although St. Francis Medical Center is a Catholic hospital, it would lose that designation under the deal.
“As a safety-net hospital, ensuring the community has access to care is the heart of our mission,” said Joseph Youngblood, PhD, chair of St. Francis Medical Center’s board, in a May 6 news release. “In response to a broad national transformation of healthcare, we look to combine our strengths with those of Capital, a healthcare leader and grow services for our residents.
Workers at three Tenet Healthcare hospitals in Southern California will hold a rally May 6 to highlight their concerns about staffing, wages and benefits during the COVID-19 pandemic, according to the union that represents them.
The rally comes as the National Union of Healthcare Workers is in negotiations with Dallas-based Tenet for more than 600 direct Tenet employees at Fountain Valley Regional, including respiratory therapists, nursing assistants and X-ray technicians. The union is also in negotiations with the Compass Group, a food and support services provider, for about 225 housekeepers and food service workers at Tenet California hospitals in Fountain Valley, Los Alamitos and Lakewood, who are subcontracted by Tenet and employees of Compass.
Union spokesperson Matt Artz told Becker’s workers contend Tenet has remained profitable during the pandemic, but it did not implement appropriate safety measures. He said Tenet also rejected proposals to better staff certain units, and it has rejected the union’s proposal to stop subcontracting out the housekeepers and food service workers who have struggled to afford healthcare.
The union said Tenet, a major for-profit hospital operator, has the financial means to address these issues. The company reported a $97 million profit in the first quarter of 2021. Tenet stock also recently hit a new 52-week high, according to an April 29 report from Zacks Equity Research.
“These profits are not helping workers or patients,” Christina Rodriguez, a respiratory therapist at Fountain Valley (Calif.) Regional Hospital, said in a May 5 news release. “They’re being made at the expense of patient care and the people who have put their health on the line to help patients during this pandemic. At the height of the surge, I would go home crying that we didn’t have enough staff to help patients struggling to survive.”
Tenet contends the issue is not about Tenet but rather about negotiations between Compass and the union. Tenet said it is focused on staff and patients.
“This matter is not about us. It’s about a negotiation strictly between the NUHW and the Compass Group, which is a vendor that provides a range of food, laundry and other support services to hospitals,” Tenet told Becker’s. “At all times, our main concern is the safety of our staff, the integrity of our facilities and the best possible outcomes for our patients, and we remain hopeful that the NUHW and Compass will reach a positive outcome at the conclusion of their respective negotiations.”
But the union said Tenet can decide whether to bring the subcontracted housekeepers and food service workers in-house, which would benefit them in terms of wages and health benefits.
Meanwhile, Compass said it will continue to negotiate in good faith, with union members.
“Our hardworking team members are at the heart of what we do, and their determination to provide best-in-class care and service is inspiring,” a Compass spokesperson told Becker’s.“We take pride in paying competitive wages and providing affordable benefits and continue to uphold our agreement with the NUHW. We have a long history of listening to our employees, working productively with unions, and will continue to meet and negotiate — always in good faith.”
Respiratory therapists, housekeepers, nursing assistants, medical technicians, dietary workers and others represented by the union said they plan to rally from 11 a.m. to noon May 6 outside Fountain Valley Regional.
The rally, scheduled after Tenet’s shareholders meeting, includes workers from Los Alamitos (Calif.) Medical Center and Lakewood (Calif.) Regional Medical Center. Union workers whose jobs are subcontracted to Compass will speak during the rally, the union said.


:max_bytes(150000):strip_icc()/GettyImages-477514725-c4271ad485734ba6b84cae22be7833cf.jpg)