COVID-19 hospitalizations are at record high numbers nationwide, though some parts of the country are seeing cases plateau or fall, Surgeon General Vivek Murthy, MD, said Jan. 16 on CNN‘s “State of the Union.”
In New York and other parts of the Northeast, “we are starting to see a plateau and, in some cases, an early decline in cases,” Dr. Murthy said. Daily average cases in New York have fallen 27 percent in the last 14 days, according to Jan. 18 data tracked by The New York Times. New Jersey, Maryland and Washington, D.C., have also seen cases fall in recent days.
“The omicron wave started later in other parts of the country. So we shouldn’t expect a national peak in the next coming days,” Dr. Murthy said. “The next few weeks will be tough.”
As of Jan. 17, a record 154,335 people were hospitalized with COVID-19 nationwide, HHS data shows. Hospitalizations had previously peaked at 142,273 on Jan. 14, 2021.
Two other forecasts to know:
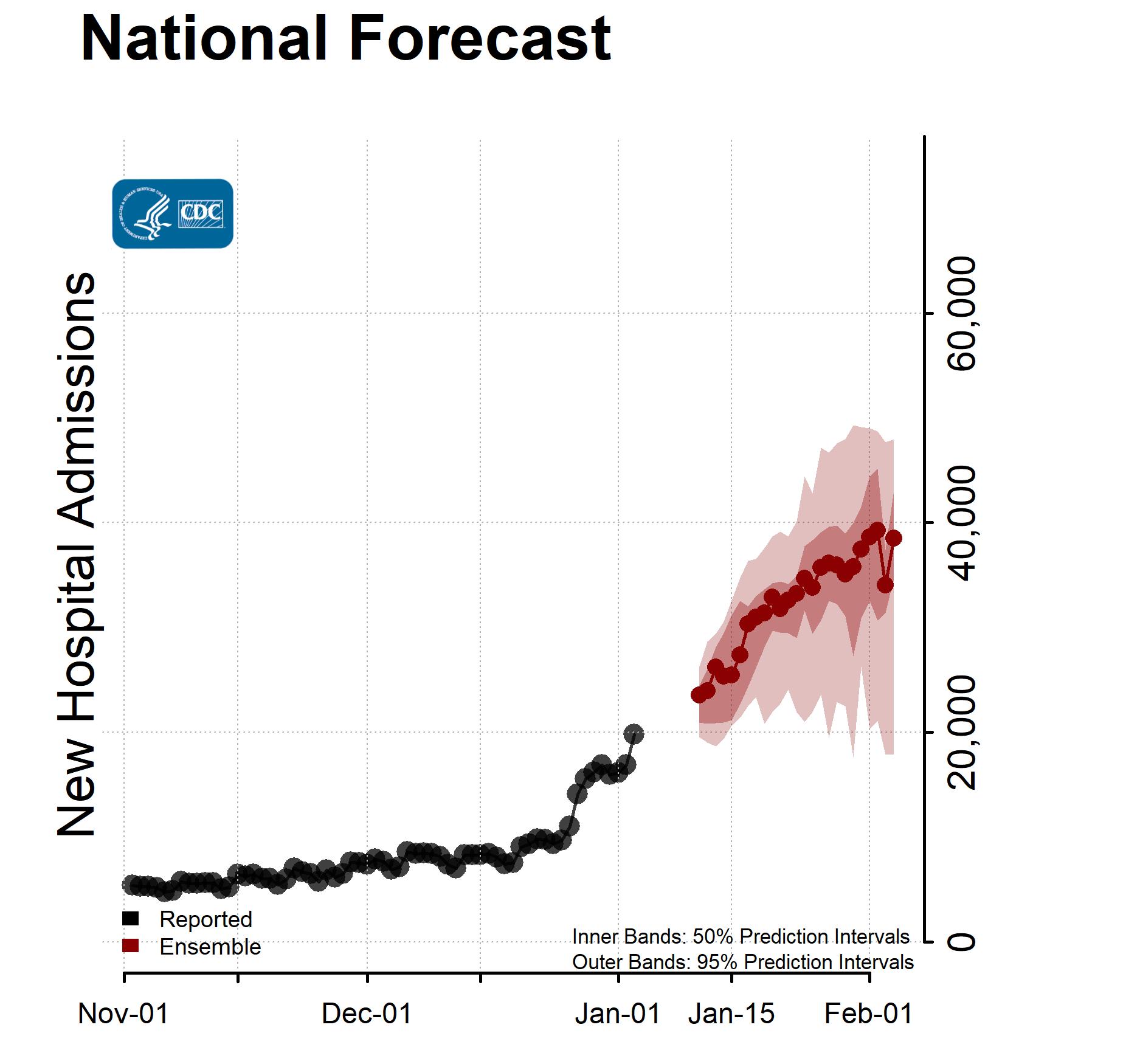
1. Daily COVID-19 hospital admissions will increase over the next four weeks, with 17,900 to 48,000 new admissions likely reported on Feb. 4, according to ensemble forecasts the CDC published Jan. 12. For context, the current seven-day hospitalization average for Jan. 5-11 is 20,637, a 24.5 percent increase from the previous week’s average.
2. CDC forecasting predicts COVID-19 deaths will increase nationwide over the next month, with 10,400 to 31,000 deaths likely reported in the week ending Feb. 5. Current forecasts should be interpreted with caution, the CDC said, as they may not fully account for omicron’s rapid spread or changes in reporting during the holidays.
New daily COVID-19 hospitalization rates in the U.S. have risen 54 percent over the last two weeks, with all 50 states and the District of Columbia seeing hospitalization rates trend upward, according to data tracked byThe New York Times.
Data is taken from HHS and was last updated Jan. 18. States are listed in order of hospitalization rate percent increase over the last two weeks.
Alabama 14-day change: 133% increase Hospitalizations per 100,000 people: 50
Louisiana 14-day change: 120% increase Hospitalizations per 100,000 people: 41
California 14-day change: 118% increase Hospitalizations per 100,000 people: 35
Mississippi 14-day change: 109% increase Hospitalizations per 100,000 people: 47
Florida 14-day change: 105% increase Hospitalizations per 100,000 people: 53
Hawaii 14-day change: 102% increase Hospitalizations per 100,000 people: 25
South Carolina 14-day change: 102% increase Hospitalizations per 100,000 people: 43
Washington 14-day change: 99% increase Hospitalizations per 100,000 people: 31
Alaska 14-day change: 89% increase Hospitalizations per 100,000 people: 15
Texas 14-day change: 86% increase Hospitalizations per 100,000 people: 45
Arkansas 14-day change: 81% increase Hospitalizations per 100,000 people: 43
Nevada 14-day change: 81% increase Hospitalizations per 100,000 people: 57
Vermont 14-day change: 77% increase Hospitalizations per 100,000 people: 19
Massachusetts 14-day change: 76% increase Hospitalizations per 100,000 people: 46
Georgia 14-day change: 71% increase Hospitalizations per 100,000 people: 57
Tennessee 14-day change: 70% increase Hospitalizations per 100,000 people: 47
North Carolina 14-day change: 65% increase Hospitalizations per 100,000 people: 46
Oregon 14-day change: 64% increase Hospitalizations per 100,000 people: 21
Virginia 14-day change: 58% increase Hospitalizations per 100,000 people: 46
Rhode Island 14-day change: 57% increase Hospitalizations per 100,000 people: 51
Utah 14-day change: 57% increase Hospitalizations per 100,000 people: 22
Wyoming 14-day change: 57% increase Hospitalizations per 100,000 people: 18
Montana 14-day change: 52% increase Hospitalizations per 100,000 people: 20
Oklahoma 14-day change: 51% increase Hospitalizations per 100,000 people: 41
Idaho 14-day change: 50% increase Hospitalizations per 100,000 people: 22
South Dakota 14-day change: 46% increase Hospitalizations per 100,000 people: 39
Colorado 14-day change: 45% increase Hospitalizations per 100,000 people: 31
Connecticut 14-day change: 44% increase Hospitalizations per 100,000 people: 57
Missouri 14-day change: 44% increase Hospitalizations per 100,000 people: 61
New York State 14-day change: 40% increase Hospitalizations per 100,000 people: 67
Kentucky 14-day change: 39% increase Hospitalizations per 100,000 people: 51
New Jersey 14-day change: 39% increase Hospitalizations per 100,000 people: 69
District of Columbia 14-day change: 37% increase Hospitalizations per 100,000 people: 125
Kansas 14-day change: 37% increase Hospitalizations per 100,000 people: 43
West Virginia 14-day change: 35% increase Hospitalizations per 100,000 people: 52
Pennsylvania 14-day change: 34% increase Hospitalizations per 100,000 people: 63
Arizona 14-day change: 33% increase Hospitalizations per 100,000 people: 44
Maryland 14-day change: 32% increase Hospitalizations per 100,000 people: 60
Wisconsin 14-day change: 32% increase Hospitalizations per 100,000 people: 43
Maine 14-day change: 28% increase Hospitalizations per 100,000 people: 34
Nebraska 14-day change: 28% increase Hospitalizations per 100,000 people: 35
Iowa 14-day change: 24% increase Hospitalizations per 100,000 people: 31
Illinois 14-day change: 21% increase Hospitalizations per 100,000 people: 56
Delaware 14-day change: 20% increase Hospitalizations per 100,000 people: 64
Minnesota 14-day change: 20% increase Hospitalizations per 100,000 people: 31
New Mexico 14-day change: 19% increase Hospitalizations per 100,000 people: 31
North Dakota 14-day change: 19% increase Hospitalizations per 100,000 people: 34
Michigan 14-day change: 17% increase Hospitalizations per 100,000 people: 48
New Hampshire 14-day change: 14% increase Hospitalizations per 100,000 people: 33
Ohio 14-day change: 13% increase Hospitalizations per 100,000 people: 59
Indiana 14-day change: 8% increase Hospitalizations per 100,000 people: 49
The Omicron variant doesn’t cause as much severe illness as other variants have, but its “mild” symptoms can still be pretty unpleasant.
The big picture: The way health care professionals and doctors differentiate between “mild” and “severe” illness may not align with a layperson’s understanding of those terms.
“To a health care professional, ‘mild’ means you’re not getting hospitalized,” said Megan Ranney, academic dean at the Brown University School of Public Health.
But, she said: “Omicron symptoms can range from absolutely no symptoms to a really mild cold to something where you are in bed with shakes and chills, and have a horrible cough and are fatigued and headachy for weeks. Those are all ‘mild.'”
A “severe,” illness means you’d likely have symptoms such as very low oxygen levels, kidney damage and heart impairment, she said.
What we’re watching: Omicron is causing a lot less severe illness than previous variants, but a “mild” case can still require about a week away from work, especially in front-line jobs.
And because so many people have gotten infected in such a short time, it’s leaving schools, airlines, and other businesses — including, critically, hospitals — with large numbers of workers out sick simultaneously, The Atlantic reported.
Then there’s the matter of long COVID. A study published Thursday in Nature Immunology found ongoing, sustained inflammatory responses following even mild-to-moderate COVID-19 cases.
What they’re saying: “It’s going to be a messy few weeks. I don’t think there’s any way around it,” said Joseph Allen, a professor of public health at Harvard, per The Atlantic.
We’ve been having “year ahead” discussions with our health system members over the past few weeks, although it’s been difficult for some to carve out time for planning in the midst of the Omicron surge.
One common theme is that, from a financial perspective, 2022 is expected to be a more difficult year. For many systems, despite the trying COVID situation, the past two years have been financial record-setters. In 2020, systems benefited from a massive infusion of COVID relief funding from the government, and in 2021, they continued to enjoy enhanced reimbursement due to COVID, plus had a resurgence of volume as patients sought care that was previously postponed.
2022 looks to be a more “normal” year—meaning a return to the financial pressures of pre-pandemic times. Those include mounting price compression from payers, an accelerating shift of care from inpatient to outpatient settings, and increasing competition for patients from disruptors and others. At the same time, patient acuity will continue to rise, with patients presenting sicker and with more comorbidities. The cost of caring for those patients will escalate, as the workforce shortage drives labor costs higher and supply chain woes persist.
We’d anticipate a year or more of belt-tightening among many health systems, as they adjust to the post-pandemic environment.
As COVID hospitalizations surge to new highs, healthcare workers have become the rate-limiting factor for most hospitals’ ability to deliver care. Using self-reported data collected by the Department of Health and Human Services, the graphic above shows that hospital staffing concerns reached an all-time high this month, with nearly one in three hospitals reporting a critical shortage. (Anecdotal evidence from our conversations with hospital leaders suggests that the actual number in crisis may be even higher, with every system we’ve spoken to in the past month reporting severe staffing challenges.)
During previous surges, COVID hospitalizations and reported staffing shortages have ebbed and flowed together. However, staffing challenges and case numbers became decoupled during the Delta surge, as the percentage of hospitals reporting staffing shortages did not go down as the Delta wave subsided.
With a growing number of nurses and other staff choosing early retirement or looking for jobs in other sectors, health systems are navigating the Omicron spike with a smaller pool of workers. And now the high transmissibility of the Omicron variant is forcinghealthcare workers to quarantine in droves.
As shown on the map, this is playing out both in highly vaccinated states like Vermont and California, and less-vaccinated places like West Virginia and Wyoming. That’s leading some state health officials and health systems to allow COVID-positive staff who are asymptomatic or experiencing mild symptoms to continue working—a policy which is being sharply criticized by nurses.
While the end of the Omicron surge should bring some relief, longer-term staffing challenges will surely remain for most health systems.
Biden administration’s vaccine mandate for healthcare workers is a go, but its mandate for large employers and at-home testing plan face roadblocks. The US Supreme Court ruled Thursday that the vaccine mandate for the nation’s healthcare workers at facilities participating in Medicare and Medicaid can go forward while lower courts hear legal challenges. But it said that the Occupational Safety and Health Administration (OSHA) did not have the authority to enforce the broader vaccine-or-test mandate for businesses over 100 employees, which would have covered more than 80 million private sector workers.
Meanwhile, private insurers are required to begin covering eight at-home tests per beneficiary per month starting tomorrow. The roughly half of Americans with private insurance coverage stand to benefit, if they’re lucky enough to get their hands on rapid tests, which have been in increasingly scarce supply.
The Gist: Health systems that were early to issue vaccine mandates will have a leg up on others who paused requirements amid ongoing legal challenges. Lagging facilities now have a little over a month to start enforcement amid troublesome staffing shortages.
Also, the use of the private insurance system to cover at-home tests not only excludes nearly 40 million seniors on traditional Medicare, as well as the uninsured, but means that the cost of tests will ultimately be borne by consumers and employers through higher insurance premiums.
While Omicron’s rapid spread is causing COVID hospitalizations to surge once again, the impact on consumer confidence may be different this time around. Drawing on the most recent data from analytics firm Strata Decision Technology, the graphic above shows how hospital volumes have fluctuated throughout the pandemic. Hospital volumes mostly returned to pre-COVID levels early last summer, until the Delta surge caused patients to begin avoiding care across all settings once again.
It remains to be seen if the forty percent of consumers who said they were less likely to seek non-emergency care during the Delta surge feel similarly about the Omicron spike. So far, consumer sentiment seems to be holding steady at last summer’s levels, though we’re still a few weeks away from Omicron’s expected peak.
As the pandemic enters its third year, it’s also likely that consumers who have been delaying care will simply be unwilling or unable to hold off any longer. But even if Omicron doesn’t dissuade consumers from seeking non-COVID care, health systems will be hard pressed to accommodate both COVID and non-COVID care amid worrisome staffing shortages.
Hospitals across the U.S. are feeling the wrath of the omicron variant and getting thrown into disarray that is different from earlier COVID-19 surges.
This time, they are dealing with serious staff shortages because so many health care workers are getting sick with the fast-spreading variant. People are showing up at emergency rooms in large numbers in hopes of getting tested for COVID-19, putting more strain on the system. And a surprising share of patients — two-thirds in some places — are testing positive while in the hospital for other reasons.
At the same time, hospitals say the patients aren’t as sick as those who came in during the last surge. Intensive care units aren’t as full, and ventilators aren’t needed as much as they were before.
The pressures are nevertheless prompting hospitals to scale back non-emergency surgeries and close wards, while National Guard troops have been sent in in several states to help at medical centers and testing sites.
Nearly two years into the pandemic, frustration and exhaustion are running high among health care workers.
“This is getting very tiring, and I’m being very polite in saying that,” said Dr. Robert Glasgow of University of Utah Health, which has hundreds of workers out sick or in isolation.
About 85,000 Americans are in the hospital with COVID-19, just short of the delta-surge peak of about 94,000 in early September, according to the Centers for Disease Control and Prevention. The all-time high during the pandemic was about 125,000 in January of last year.
But the hospitalization numbers do not tell the whole story. Some cases in the official count involve COVID-19 infections that weren’t what put the patients in the hospital in the first place.
Dr. Fritz François, chief of hospital operations at NYU Langone Health in New York City, said about 65% of patients admitted to that system with COVID-19 recently were primarily hospitalized for something else and were incidentally found to have the virus.
At two large Seattle hospitals over the past two weeks, three-quarters of the 64 patients testing positive for the coronavirus were admitted with a primary diagnosis other than COVID-19.
Joanne Spetz, associate director of research at the Healthforce Center at the University of California, San Francisco, said the rising number of cases like that is both good and bad.
The lack of symptoms shows vaccines, boosters and natural immunity from prior infections are working, she said. The bad news is that the numbers mean the coronavirus is spreading rapidly, and some percentage of those people will wind up needing hospitalization.
This week, 36% of California hospitals reported critical staffing shortages. And 40% are expecting such shortages.
Some hospitals are reporting as much as one quarter of their staff out for virus-related reasons, said Kiyomi Burchill, the California Hospital Association’s vice president for policy and leader on pandemic matters.
In response, hospitals are turning to temporary staffing agencies or transferring patients out.
University of Utah Health plans to keep more than 50 beds open because it doesn’t have enough nurses. It is also rescheduling surgeries that aren’t urgent. In Florida, a hospital temporarily closed its maternity ward because of staff shortages.
In Alabama, where most of the population is unvaccinated, UAB Health in Birmingham put out an urgent request for people to go elsewhere for COVID-19 tests or minor symptoms and stay home for all but true emergencies. Treatment rooms were so crowded that some patients had to be evaluated in hallways and closets.
As of Monday, New York state had just over 10,000 people in the hospital with COVID-19, including 5,500 in New York City. That’s the most in either the city or state since the disastrous spring of 2020.
New York City hospital officials, though, reported that things haven’t become dire. Generally, the patients aren’t as sick as they were back then. Of the patients hospitalized in New York City, around 600 were in ICU beds.
“We’re not even halfway to what we were in April 2020,” said Dr. David Battinelli, the physician-in-chief for Northwell Health, New York state’s largest hospital system.
Similarly, in Washington state, the number of COVID-19-infected people on ventilators increased over the past two weeks, but the share of patients needing such equipment dropped.
In South Carolina, which is seeing unprecedented numbers of new cases and a sharp rise in hospitalizations, Gov. Henry McMaster took note of the seemingly less-serious variant and said: “There’s no need to panic. Be calm. Be happy.”
Amid the omicron-triggered surge in demand for COVID-19 testing across the U.S., New York City’s Fire Department is asking people not to call for ambulance just because they are having trouble finding a test.
In Ohio, Gov. Mike DeWine announced new or expanded testing sites in nine cities to steer test-seekers away from ERs. About 300 National Guard members are being sent to help out at those centers.
In Connecticut, many ER patients are in beds in hallways, and nurses are often working double shifts because of staffing shortages, said Sherri Dayton, a nurse at the Backus Plainfield Emergency Care Center. Many emergency rooms have hours-long waiting times, she said.
“We are drowning. We are exhausted,” Dayton said.
Doctors and nurses are complaining about burnout and a sense their neighbors are no longer treating the pandemic as a crisis, despite day after day of record COVID-19 cases.
“In the past, we didn’t have the vaccine, so it was us all hands together, all the support. But that support has kind of dwindled from the community, and people seem to be moving on without us,” said Rachel Chamberlin, a nurse at New Hampshire’s Dartmouth-Hitchcock Medical Center.
Edward Merrens, chief clinical officer at Dartmouth-Hitchcock Health, said more than 85% of the hospitalized COVID-19 patients were unvaccinated.
Several patients in the hospital’s COVID-19 ICU unit were on ventilators, a breathing tube down their throats. In one room, staff members made preparations for what they feared would be the final family visit for a dying patient.
One of the unvaccinated was Fred Rutherford, a 55-year-old from Claremont, New Hampshire. His son carried him out of the house when he became sick and took him to the hospital, where he needed a breathing tube for a while and feared he might die.
If he returns home, he said, he promises to get vaccinated and tell others to do so too.
“I probably thought I was immortal, that I was tough,” Rutherford said, speaking from his hospital bed behind a window, his voice weak and shaky.
But he added: “I will do anything I can to be the voice of people that don’t understand you’ve got to get vaccinated. You’ve got to get it done to protect each other.”
Many people around the world kicked off 2022 by searching for more information about “flurona,” after Israel reported that two young pregnant women had tested positive for both the coronavirus and the flu.
Doctors have long been concerned about the potential impact of a “twindemic” — with influenza cases rising as covid-19 cases threaten to overwhelm hospitals — and called on people to get flu shots and coronavirus vaccinations. On the other hand, “flurona” refers to when one person has both respiratory infections at the same time — which health officials say is a possibility as cases of the highly contagious omicron variant of the coronavirus surge this winter across the world.
Here’s what we know so far.
Are cases of flurona new?
After two young pregnant women tested positive for both the coronavirus and influenza in Israel, many local and global media outlets dubbed it “flurona” in headlines. The Sun, a British tabloid, swiftly branded the co-infection “double trouble.”
While the word is relatively new and rising in popularity, cases of flu and coronavirus co-infections are not. And flurona is not a distinct disease but refers to when a person has been infected with both viruses. Flurona instances have been detected in countries including the United States, Israel, Brazil, the Philippines and Hungary, some even before the term was coined.
Instances of the co-infection were reported in the United States almost two years ago, according to a report from the Atlantic. In February 2020, a man entered a New York hospital with a severe cough and fever. At the time, the city had not officially reported any cases of the coronavirus. The patient tested positive for influenza and was then tested for the coronavirus. Weeks later, results confirmed that he, along with threefamily members, had contracted both viruses.
Where has flurona been reported?
There have been other recent occurrences in the United States.A Houston teenager spent Christmas Day isolating in his bedroom after contracting the coronavirus and the flu at the same time. Alec Zierlein, who had been vaccinated against the coronavirus but not the flu, was also tested for strep throat, but results confirmed he had only the former two infections, which he described as being “like a mild cold.” After his diagnosis, Zierlein told ABC News that he was not aware the coronavirus and the flu could stack “up on one another” and that he would, in the future, get a flu shot as a precaution.
A health official in the Philippines has also said that such co-infections are not unusual. Edsel Salvana, a member of a technical advisory group to the national health department, said the country’s first covid-related death stemmed from a joint case in early 2020.Salvana told reporters that the early pandemic patient, a Chinese national, had covid-19 and influenza B, as well as streptococcus pneumonia, according to local outlet ABS-CBN.
An initial case report showed that the patient, who was the world’s first known covid-19 death outside of China, had a fever, cough and chills. “It’s an unfortunate confluence of events that you are exposed to two pathogens,” said Salvana, who reminded the public to get vaccinated for the flu and pneumonia.
Hungary has also identified at least two flurona instances in recent weeks, broadcaster RTL reported Monday. As was the case in Israel, both patients were described as about 30 years old.
And Brazil is battling an out-of-season flu outbreak just as omicron cases are starting to rise. Health officials there have confirmed six instances of flurona across three states. Rio de Janeiro’s municipal health secretary, Daniel Soranz, told Spanish news agency EFE that 17 more cases were also under investigation. In one occurrence, a 16-year-old tested positive for both viruses but had light symptoms, which his mother attributed to his being fully vaccinated against both viruses, she told Brazilian media.
Is flurona more common this year?
In Israel’s Beilinson Hospital, where doctors recently diagnosed the two pregnant women with both infections, cases of the coronavirus are rising amid the omicron outbreak along with cases of influenza A, according to Arnon Vizhnitser, the director of gynecology.
In an interview with The Washington Post, Vizhnitser said that while cases of the flu were scarce last year, perhaps because of more stringent lockdown measures and social distancing, they are roaring back.
“This year is different from last year. Now we have another challenge,”he said, predicting that co-infections would probably continue to occur.
Some countries are on track to be hit much harder by the flu this year, while strict measures to control the spread of the coronavirus appeared to have largely prevented the “twindemic” scenario in 2020.
That’s the case in the United States, which had record lows as covid surged last winter but is now seeing rising flu cases. Europe’s flu season is also just starting — and likewise expected to be worse this year.
Vizhnitser said both pregnant women had the same symptoms and were given treatment to reduce their fevers. Both were immediately placed in isolation before they eventually returned home with healthy babies. According to Vizhnitser, only one of the women had been vaccinated against the coronavirus. She had also been boosted. The other patient had not received any form of inoculation against either virus.
Pregnant patients visiting Beilinson, the Israeli hospital, are being tested for both viruses if they have symptoms on arrival. Some medical workers, along with people older than 60, in Israel, which is aggressively ramping up its vaccination program, are being offered a second booster.
Are flu and covid together more dangerous?
While many countries track coronavirus and flu cases, there appears to be little data on how many people have them at the same time. As more reports surface about co-infections, health experts and doctors stress that coronavirus and flu vaccines remain the best way to protect against severe infections.
“If you are vaccinated, the disease is very mild,” Vizhnitser said ofboth the coronavirus and flu. “Women who were not vaccinated [against the coronavirus] were very sick.”
It’s also a possibility that some patients will not be offered tests for both infections, with hospitals around the world using different approaches to treating and diagnosing patients.
What are the symptoms of flurona?
The coronavirus and influenza are respiratory infections, which can cause similar symptoms such as fever, coughing, fatigue, runny nose, sore throat and diarrhea, along with muscle and body aches. Both infections can be fatal, although the severity of each diagnosis depends largely on an individual’s immune system. Health workers, the elderly and those with underlying health conditions are more at risk for each virus.
The World Health Organization notes that the viruses are also transmitted in similar ways, through droplets and aerosols that can be passed on by coughing, sneezing, speaking, singing or breathing — which is why masking to protect others is widely encouraged by officials.
While the word is relatively new and rising in popularity, cases of flu and coronavirus co-infections are not. And flurona is not a distinct disease.