LIMA, Peru — The doctor watched the patients stream into his intensive care unit with a sense of dread.
For weeks, César Salomé, a physician in Lima’s Hospital Mongrut, had followed the chilling reports. A new coronavirus variant, spawned in the Amazon rainforest, had stormed Brazil and driven its health system to the brink of collapse.Now his patients, too, were arriving far sicker, their lungs saturated with disease, and dying within days. Even the young and healthy didn’t appear protected.
The new variant, he realized, was here.
“We used to have more time,” Salomé said. “Now, we have patients who come in and in a few days they’ve lost the use of their lungs.”
The P.1 variant, which packs a suite of mutations that makes it more transmissible and potentially more dangerous, is no longer just Brazil’s problem. It’s South America’s problem — and the world’s.
In recent weeks, it has been carried across rivers and over borders, evading restrictive measures meant to curb its advance to help fuel a coronavirus surge across the continent. There is mounting anxiety in parts of South America that P.1 could quickly become the dominant variant, transporting Brazil’s humanitarian disaster — patients languishing without care, a skyrocketing death toll — into their countries.
“It’s spreading,” said Julio Castro, a Venezuelan infectious-disease expert. “It’s impossible to stop.”
In Lima, scientists have detected the variant in 40 percent of coronavirus cases. In Uruguay, it’s been found in 30 percent. In Paraguay, officials say half of cases at the border with Brazil are P.1. Other South American countries — Colombia, Argentina, Venezuela, Chile — have discovered it in their territories. Limitations in genomic sequencing have made it difficult to know the variant’s true breadth, but it has been identified in more than two dozen countries, from Japan to the United States.
Hospital systems across South America are being pushed to their limits. Uruguay, one of South America’s wealthiest nations and a success story early in the pandemic, is barreling toward a medical system failure. Health officials say Peru is on the precipice, with only 84 intensive care beds left at the end of March. The intensive care system in Paraguay, roiled by protests last month over medical shortcomings, has run out of hospital beds.
“Paraguay has little chance of stopping the spread of the P.1 variant,” said Elena Candia Florentín, president of the Paraguayan Society of Infectious Diseases.
“With the medical system collapsed, medications and supplies chronically depleted, early detection deficient, contact tracing nonexistent, waiting patients begging for treatment on social media, insufficient vaccinations for health workers, and uncertainty over when general and vulnerable populations will be vaccinated, the outlook in Paraguay is dark,” she said.
How P.1 spread across the region is a distinctly South American story. Nearly every country on the continent shares a land border with Brazil. People converge on border towns, where crossing into another country can be as simple as crossing the street. Limited surveillance and border security have made the region a paradise for smugglers. But they have also made it nearly impossible to control the variant’s spread.
“We share 1,000 kilometers of dry border with Brazil, the biggest factory of variants in the world and the epicenter of the crisis,” said Gonzalo Moratorio, a Uruguayan molecular virologist tracking the variant’s growth. “And now it’s not just one country.”
The Brazilian city of Tabatinga, deep in the Amazon rainforest, where officials suspect the virus crossed into Colombia and Peru, is emblematic of the struggle to contain the variant. The city of 70,000 was swept by P.1 earlier this year. Many in the area have family ties in several countries and are accustomed to crossing borders with ease — canoeing across the Amazon River to Peru or walking into Colombia.
“People ended up bringing the virus from one side to the other,” said Sinesio Tikuna Trovão, an Indigenous leader. “The crossing was free, with both sides living right on top of one another.”
Now that the variant has infiltrated numerous countries, stopping its spread will be difficult. Most South American countries, with the exception of Brazil, adopted stringent containment measures last year. But they have been undone by poverty, apathy, distrust and exhaustion. With national economies battered and poverty rising sharply, public health experts fear more restrictions will be difficult to maintain. In Brazil, despite record death numbers, many states are lifting restrictions.(SOUND FAMILIAR)
That has left inoculation as the only way out. But coronavirus vaccines are South America’s white whale: often discussed, but rarely seen. The continent hasn’t distributed its own vaccine or negotiated a regional agreement with pharmaceutical companies. It’s one of the world’s hardest-hit regions but has administered only 6 percent of the world’s vaccine doses, according to the site Our World in Data. (The outlier is Chile, which is vaccinating residents more quickly than anywhere in the Americas — but still suffering a surge in cases.)
“We should not only blame the policy response,” said Luis Felipe López-Calva, the United Nations Development Program’s regional director for Latin America and the Caribbean. “We have to understand the vaccine market.”
“And there is a failure in the market,” he said.
The vaccine has become so scarce, López-Calva said, that officials are imposing restrictions on information. It’s nearly impossible to know how much governments are paying for doses. Some regional blocs, such as the African Union and the European Union, have negotiated joint contracts. But in South America, it has been every country for itself — diminishing the bargaining power for each one.
“This has been harmful for these countries, and for the whole world to stop the virus,” López-Calva said. “Because it’s never been more clear that no one is protected until everyone is protected.”
Paulo Buss, a prominent Brazilian scientist, said it didn’t have to be like this. He was Brazil’s health representative to the Union of South American Nations, which negotiated several regional deals with pharmaceutical companies before the coronavirus pandemic. But that union came apart amid political differences just before the arrival of the virus.
“It was the worst possible moment,” Buss said. “We’ve lost capacity and our negotiation attempts have been fragmented. Multi-lateralism was weakened.”
Vaccine scarcity has led to line-jumping scandals all over South America, but particularly in Peru. Hundreds of politically connected people, including cabinet ministers and former president Martín Vizcarra, snagged vaccine doses early. Now people are calling for criminal charges.
As officials bicker and the vaccination campaign is delayed, the variant continues to spread. P.1 accounts for 70 percent of cases in some parts of the Lima region, according to officials. Last week, the country logged the highest daily case count since August — more than 11,000. On Saturday, the country recorded 294 deaths, the most in a day since the start of the pandemic.
Peruvians have been stunned by how quickly the surge overwhelmed the health-care system. Public health analysts and government officials had believed Peru was prepared for a second wave. But it wasn’t ready for the variant.
“We did not expect such a strong second wave,” said Percy Mayta-Tristan, director of research at the Scientific University of the South in Lima. “The first wave was so extensive. The presence of the Brazilian variant helps explain why.”
Stephanie Nana, an evangelical Christian in Edmond, Okla., refused to get a Covid-19 vaccine because she believed it contained “aborted cell tissue.”
Nathan French, who leads a nondenominational ministry in Tacoma, Wash., said he received a divine message that God was the ultimate healer and deliverer:“The vaccine is not the savior.”
Lauri Armstrong, a Bible-believing nutritionist outside of Dallas, said she did not need the vaccine because God designed the body to heal itself, if given the right nutrients. More than that, she said, “It would be God’s will if I am here or if I am not here.”
The deeply held spiritual convictions or counterfactual arguments may vary. But across white evangelical America, reasons not to get vaccinated have spread as quickly as the virus that public health officials are hoping to overcome through herd immunity.
The opposition is rooted in a mix of religious faith and a longstanding wariness of mainstream science, and it is fueled by broader cultural distrust of institutions and gravitation to online conspiracy theories. The sheer size of the community poses a major problem for the country’s ability to recover from a pandemic that has resulted in the deaths of half a million Americans. And evangelical ideas and instincts have a way of spreading, even internationally.
There are about 41 million white evangelical adults in the U.S. About 45 percent said in late February that they would not get vaccinated against Covid-19, making them among the least likely demographic groups to do so, according to the Pew Research Center.
“If we can’t get a significant number of white evangelicals to come around on this, the pandemic is going to last much longer than it needs to,” said Jamie Aten, founder and executive director of the Humanitarian Disaster Institute at Wheaton College, an evangelical institution in Illinois.
As vaccines become more widely available, and as worrisome virus variants develop, the problem takes on new urgency.Significant numbers of Americans generally are resistant to getting vaccinated, but white evangelicals present unique challenges because of their complex web of moral, medical, and political objections.The challenge is further complicated by longstanding distrust between evangelicals and the scientific community.
“Would I say that all public health agencies have the information that they need to address their questions and concerns? Probably not,” said Dr. Julie Morita, the executive vice president of the Robert Wood Johnson Foundation and a former Chicago public health commissioner.
No clear data is available about vaccine hesitancy among evangelicals of other racial groups. But religious reasoning often spreads beyond white churches.
Many high-profile conservative pastors and institutional leaders have endorsed the vaccines. Franklin Graham told his 9.6 million Facebook followers that Jesus would advocate for vaccination. Pastor Robert Jeffress commended it from an anti-abortion perspective on Fox News. (“We talk about life inside the womb being a gift from God. Well, life outside the womb is a gift from God, too.”) The president of the Southern Baptist Convention, J.D. Greear, tweeted a photo of himself receiving a shot.
But other influential voices in the sprawling, trans-denominational movement, especially those who have gained their stature through media fame, have sown fears.Gene Bailey, the host of a prophecy-focused talk show on the Victory Channel, warned his audience in March that the government and “globalist entities” will “use bayonets and prisons to force a needle into your arm.” In a now-deleted TikTok post from an evangelical influencer’s account that has more than 900,000 followers, she dramatized being killed by authorities for refusing the vaccine.
Dr. Simone Gold, a prominent Covid-19 skeptic who was charged with violent entry and disorderly conduct in the Jan. 6 Capitol siege, told an evangelical congregation in Florida that they were in danger of being “coerced into taking an experimental biological agent.”
The evangelical radio host Eric Metaxas wrote “Don’t get the vaccine” in a tweet on March 28 that has since been deleted. “Pass it on,” he wrote.
Some evangelicals believe that any Covid restrictions — including mask mandates and restrictions on in-person church worship — constitute oppression.
And some have been energized by what they see as a battle between faith and fear, and freedom and persecution.
“Fear is the motivating power behind all of this, and fear is the opposite of who God is,” said Teresa Beukers, who travels throughout California in a motor home. “I violently oppose fear.”
Ms. Beukers foresees severe political and social consequences for resisting the vaccine, but she is determined to do so. She quit a job at Trader Joe’s when the company insisted that she wear a mask at work. Her son, she said, was kicked off his community college football team for refusing Covid testing protocols.
“Go ahead and throw us in the lions’ den, go ahead and throw us in the furnace,” she said, referring to two biblical stories in which God’s people miraculously survive persecution after refusing to submit to temporal powers.
Jesus, she added, broke ritual purity laws by interacting with lepers. “We can compare that to people who are unvaccinated,” she said. “If they get pushed out, they’ll need to live in their own colonies.”
One widespread concern among evangelicals is the vaccines’ ties to abortion.In reality, the connection is remote: Some of the vaccines were developed and tested using cells derived from the fetal tissue of elective abortions that took place decades ago.
The vaccines do not include fetal tissue, and no additional abortions are required to manufacture them. Still, the kernel of a connection has metastasized online into false rumors about human remains or fetal DNA being an ingredient in the vaccines.
Some evangelicals see the vaccine as a redemptive outcome for the original aborted fetus.
Some Catholic bishops have expressed concerns about the abortion link, too. But the Vatican has concluded the vaccines are “morally acceptable,” and has emphasized the immediate danger posed by the virus. Just 22 percent of Catholics in America say they will not get the vaccine, less than half the share of white evangelicals who say that.
White evangelicals who do not plan to get vaccinated sometimes say they see no need, because they do not feel at risk. Rates of Covid-19 death have been about twice as high for Black, Hispanic, and Native Americans as for white Americans.
White pastors have largely remained quiet. That’s in part because the wariness among white conservative Christians is not just medical, but also political. If white pastors encourage vaccination directly, said Dr. Aten, “there are people in the pews where you’ve just attacked their political party, and maybe their whole worldview.”
Dr. Morita, of the Robert Wood Johnson Foundation, saidthe method to reach white evangelicals is similar to building vaccine confidence in other groups: Listen to their concerns and questions, and then provide information that they can understand from people they trust.
But a public education campaign alone may not be enough.
There has been a “sea change” over the past century in how evangelical Christians see science, a change rooted largely in the debates over evolution and the secularization of the academy, said Elaine Ecklund, professor of sociology and director of the Religion and Public Life Program at Rice University.
There are two parts to the problem, she said: The scientific community has not been as friendly toward evangelicals, and the religious community has not encouraged followers to pursue careers in science.
Distrust of scientists has become part of cultural identity, of what it means to be white and evangelical in America, she said.
For slightly different reasons, the distrust is sometimes shared by Asian, Hispanic and Black Christians, who are skeptical that hospitals and medical professionals will be sensitive to their concerns, Dr. Ecklund said.
“We are seeing some of the implications of the inequalities in science,” she said. “This is an enormous warning of the fact that we do not have a more diverse scientific work force, religiously and racially.”
Among evangelicals, Pentecostal and charismatic Christians may be particularly wary of the vaccine, in part because their tradition historically emphasizes divine health and miraculous healing in ways that can rival traditional medicine,said Erica Ramirez, a scholar of Pentecostalism and director of applied research at Auburn Seminary. Charismatic churches also attract significant shares of Black and Hispanic Christians.
Dr. Ramirez compares modern Pentecostalism to Gwyneth Paltrow’s Goop, with the brand’s emphasis on “wellness” and “energy” that infuriates some scientists: “It’s extra-medical,” she said. “It’s not anti-medical, but it decenters medicine.”
The Centers for Disease Control and Prevention and Dr. Anthony Fauci are not going to be able to persuade evangelicals, according to Curtis Chang, a consulting professor at Duke Divinity School who is leading an outreach project to educate evangelicals about the vaccine.
The project includes a series of short, shareable videos for pastors, answering questions like “How can Christians spot fake news on the vaccine?” and “Is the vaccine the Mark of the Beast?” The latter refers to an apocalyptic theory that the AntiChrist will force his sign onto everyone at the end of the world.
These are questions that secular public health entities are not equipped to answer, he said. “The even deeper problem is, the white evangelicals aren’t even on their screen.”
Mr. Chang said he recently spoke with a colleague in Uganda whose hospital had received 5,000 vaccine doses, but had only been able to administer about 400, because of the hesitancy of the heavily evangelical population.
“How American evangelicals think, write, feel about issues quickly replicates throughout the entire world,” he said.
At this critical moment, even pastors struggle to know how to reach their flocks. Joel Rainey, who leads Covenant Church in Shepherdstown, W.Va., said several colleagues were forced out of their churches after promoting health and vaccination guidelines.
Politics has increasingly been shaping faith among white evangelicals, rather than the other way around, he said. Pastors’ influence on their churches is decreasing. “They get their people for one hour, and Sean Hannity gets them for the next 20,” he said.
Mr. Rainey helped his own Southern Baptist congregation get ahead of false information by publicly interviewing medical experts — a retired colonel specializing in infectious disease, a church member who is a Walter Reed logistics management analyst, and a church elder who is a nurse for the Department of Veterans Affairs.
On the worship stage, in front of the praise band’s drum set, he asked them “all of the questions that a follower of Jesus might have,” he said later.
“It is necessary for pastors to instruct their people that we don’t always have to be adversaries with the culture around us,” he said. “We believe Jesus died for those people, so why in the world would we see them as adversaries?”
It seems pretty clear the path the United States is on. Within a few months, everyone who wants to be vaccinated against the coronavirus will be, save for those below the minimum age for which vaccines are available.For everyone else, the pandemic Wild West will continue, with the country hopefully somewhere near the level of immunity that will keep the virus from spreading wildly but with large parts of the population — again, including kids — susceptible to infection.
That really gets at one of the two outstanding questions: How many Americans won’t get the vaccine? If the figure is fairly low, the ability of the virus to spread will be far lower. If it’s high, we have a problem. And that’s the other outstanding question: How big of a problem will the virus be, moving forward?
We know that even as vaccines are being rolled out, cases are slowly climbing. While the number of new infections recorded each day is well off the highs seen in the winter, we’re still averaging more cases on a daily basis than we saw even a month into the third wave that began in September. A lot of people are still getting sick, and, even with most elderly Americans now protected with vaccine, a lot more people will probably die.
Data released by Gallup this week shows that both of the questions posed above share a common component. It is, as you probably suspected, those who are least willing to get vaccinated who are also least likely to take steps to contain the virus.
Gallup asked Americans about their vaccination status, finding that about a fifth had been fully vaccinated and an additional 13 percent partially vaccinated. More than a quarter of respondents, though, said they didn’t plan to get vaccinated. It was those in that latter group who were least likely to say that they were completely or mostly isolating in an effort to prevent the virus spreading.
It was also those skeptics who were least likely to say that, in the past seven days, they had avoided crowds, group gatherings or travel. If you’re not inclined to get vaccinated, it is at least consistent that you would be similarly disinclined to take other steps aimed at limiting the spread of the virus.
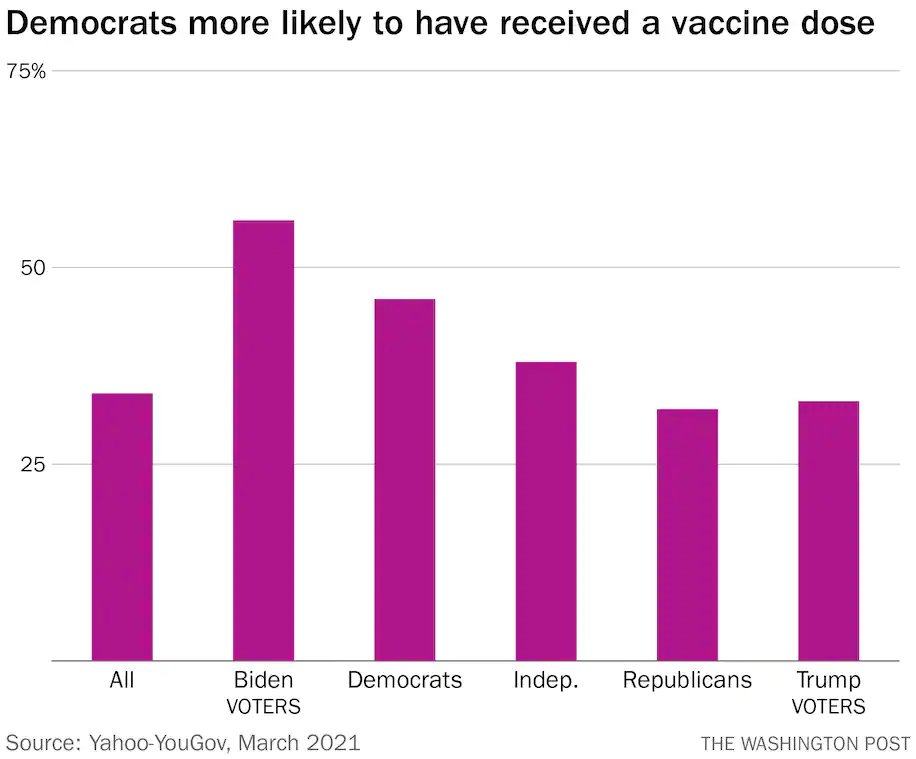
Gallup didn’t break out those groups by party, but it’s clear that few of them are Democrats. Data from YouGov, compiled on behalf of Yahoo News, shows that Democrats (and those who voted for Joe Biden in particular) are more likely to say that they have already received a vaccine dose.
Among those who hadn’t yet received a dose, Democrats were far more likely to indicate that they planned to do so as soon as possible. Among Republicans, half of those who haven’t been vaccinated say that they don’t have any plans to do so at all.
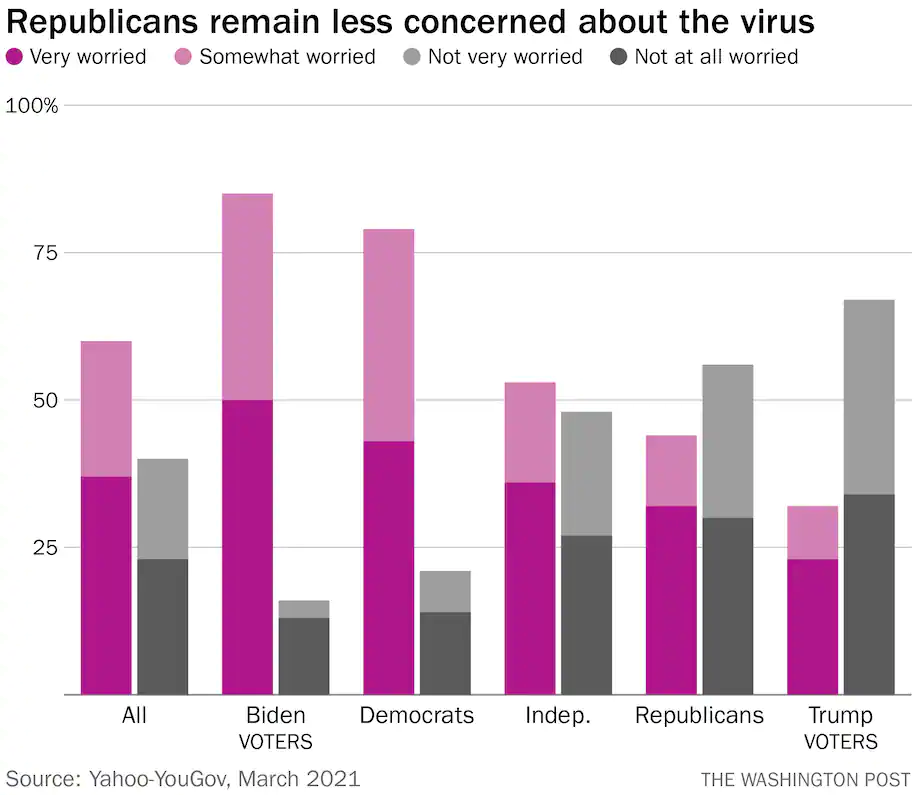
One reason is that Republicans are simply less worried about the virus. More than half say that they’re not very worried about it or not worried at all. Among those who voted for Donald Trump, the figure is over two-thirds. By contrast, more than three-quarters of Democrats say that they are at least somewhat worried about the virus.
In the YouGov polling, 60 percent of Republicans say that the worst of the pandemic is behind us. They’re also much more likely to say that restrictions aimed at preventing the spread of the virus — mask mandates, limits on indoor dining — should be lifted immediately.
As we mentioned Thursday, there are two ways to achieve herd immunity.One is fast and safe:widespread vaccinations. The other — people contracting the virus — is slow and dangerous. The path the United States is on will take us to a place where much of the country has opted for the first option and the rest, the latter.
So the question again becomes: How many people will die, both over the short term and the long term, as a result of those choices?
Houston Methodist will make the COVID-19 vaccine mandatory for employees, with the first phase including managers and new hires, the health system said March 31.
In an email, Marc Boom, MD, president and CEO, told managers new hires are already required to be vaccinated as a condition to joining Houston Methodist, and management is now also required to do the same.
“When we choose to be vaccinated against COVID-19, we are prioritizing safety by helping stop the spread of this deadly virus and keeping our patients, visitors and colleagues safe,” Dr. Boom wrote to managers. “As we move closer to announcing mandatory vaccinations for all employees, we need you to go first — to lead by example and show our employees how important getting vaccinated is.”
At Houston Methodist, 95 percent of management and all executives have already received at least one dose of a COVID-19 vaccine. Dr. Boom said managers who have not done this have until April 15 to receive at least one dose or get an approved exemption. Those who do not comply would first have a discussion with their supervisor, then could face suspension then termination.
All 26,000 Houston Methodist employees and employed physicians soon will be required to receive at least one shot.
Overall, about 83 percent of the health system’s employees have been vaccinated.