When COVID volumes waned in the spring and early summer, most health systems “de-escalated” dedicated COVID testing and triage facilities. But with the Delta variant surging across the country, consumers are now once again looking for services like drive-through testing, which is perceived as more convenient and safer.
One physician leader told us patients in the ED are asking why the hospital got rid of the “COVID tent”, which provided a separate pathway for patients with respiratory and other COVID symptoms—and a highly visible signal that the rest of the department was as COVID-free as possible.
Another system is now fielding questions from the media about whether they’ll bring back their dedicated COVID hospital: “We spent a lot of time last year convincing the community that the dedicated hospital was key to safely managing care during the pandemic. Now we’ve got almost as many COVID admissions spread across our hospitals.”
Over the past year, providers have learned how to safely manage COVID care and prevent spread in healthcare settings—but consumers may perceive the lack of dedicated facilities as a decline in safety.
Unlike last year, hospitals are full of non-COVID patients, as those who delayed care reemerge. And with the current surge likely to continue into flu season, emergency rooms will only get more crowded, necessitating a new round of communication describing how hospitals are keeping patients safe, and reassuring patients that healthcare settings remain one of the safest places to visit in the community.
There’s been a lot of hand wringing over the ongoing feeding frenzy among private equity (PE) firms for physician practice acquisition, which has caused health system executives everywhere to worry about the displacement effect on physician engagement strategies (not to mention the inflationary impact on practice valuations).
While we’ve long believed that PE firms are not long-term owners of practices, instead playing a roll-up function that will ultimately end in broader aggregation by vertically-integrated insurance companies, a recent conversation with one system CEO reframed the phenomenon in a way we hadn’t thought of before. It’s all about ademographic shift, she argued.
There’s a generation of Boomer-aged doctors who followed their entrepreneurial calling and started their own practices, and are now nearing retirement age without an obvious path to exit the business. Many didn’t plan for retirement—rather than a 401(k), what they have is equity in the practice they built.
What the PE industry is doing now is basically helping those docs transition out of practice by monetizing their next ten years of income in the form of a lump-sum cash payout. You could have predicted this phenomenon decades ago.
The real question is what happens to the younger generations of doctors left behind, who have another 20 or 30 years of practice ahead of them? Will they want to work in a PE-owned (or insurer-owned) setting, or would they prefer health system employment—or something else entirely?
The answer to that question will determine the shape of physician practice for decades to come…at least until the Millennials start pondering their own retirement.
The US now has more job openings than any time in history—and the mismatch in workforce supply and demand in the broader economy is even more acute in the healthcare sector. While the industry saw significant job losses in April 2020, employment in many healthcare subsectors quickly rebounded to slightly below pre-pandemic levels, according to data from the Bureau of Labor Statistics.
While ambulatory and hospital employment has mostly recovered, employment in nursing and residential care facilities has continued to decline.
Healthcare’s sluggish return to pre-pandemic employment levels is not for lack of demand. The number of job listings has grown nearly 30 percent since the second quarter of 2020, to nearly 4.5M openings, while new hires have flatlined, resulting in over half of healthcare job listings remaining unfilled as of Q2 2021.
In a recent McKinsey & Company survey of over 100 large US hospitals, health system executives ranked workforce shortages among nurses and clinical staff as their greatest barrier to increasing capacity.
Amid the current COVID surge, many systems are offering sizeable bonuses to attract new employees. These strategies will be critical across the next year, as systems look to reduce spending on costly travel nurses, manage COVID surges while continuing to offer elective care, and forestall further burnout.
But longer term, rethinking job functions, integrating new technology and finding ways to educate and upskill critical clinical talent will be key to winning the war for talent.
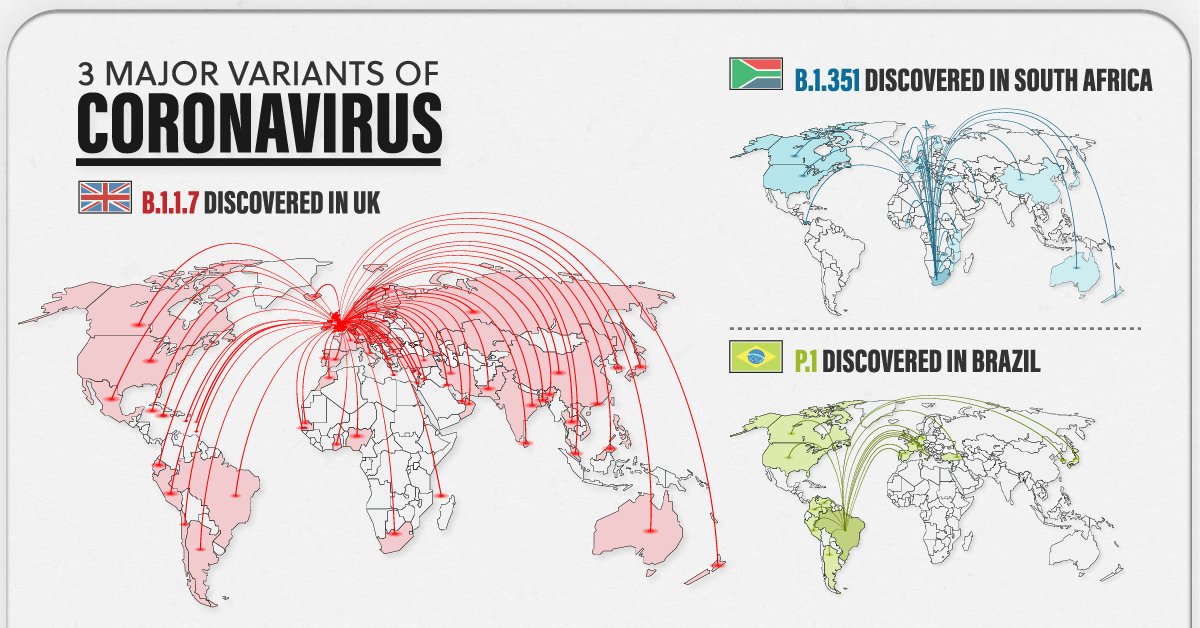
As billions of people gear up for widespread vaccination against COVID-19, another issue has reared its head. Three major COVID-19 variants have emerged across the globe—and preliminary research suggests these variants may be cause for concern.
But what makes them different from the original strain?
The following visualizations answer some key questions, including when these variants were first discovered, how far they’ve spread worldwide, and most importantly, their potential impact on the population.
Some Context: What is a Variant?
Before diving in, it’s important to understand why viruses mutate in the first place.
To infect someone, a virus takes over a host cell and uses it to replicate itself. But nature isn’t perfect, and sometimes, mistakes are made during the replication process—those mistakes are called mutations.
A virus with one or more mutations is referred to as a variant. Most of the time, variants do not affect a virus’s physical structure, and in those instances, they eventually disappear. However, there are certain cases when a mutation impacts part of a virus’s genetic makeup that does change its behavior.
According to the U.S. Centers for Disease Control (CDC) a change in behavior can alter:
Rate of transmission
Deadliness
Ability to potentially infect someone with natural or vaccine-induced immunity
Preliminary research has detected some of these changes in the three major COVID-19 variants—B.1.1.7, B.1.351, and P.1.
The 3 Major COVID-19 Variants
The three major variants emerged at different times, and in different parts of the world. Here’s an overview of each variant, when they were discovered, and how far they’ve spread so far.
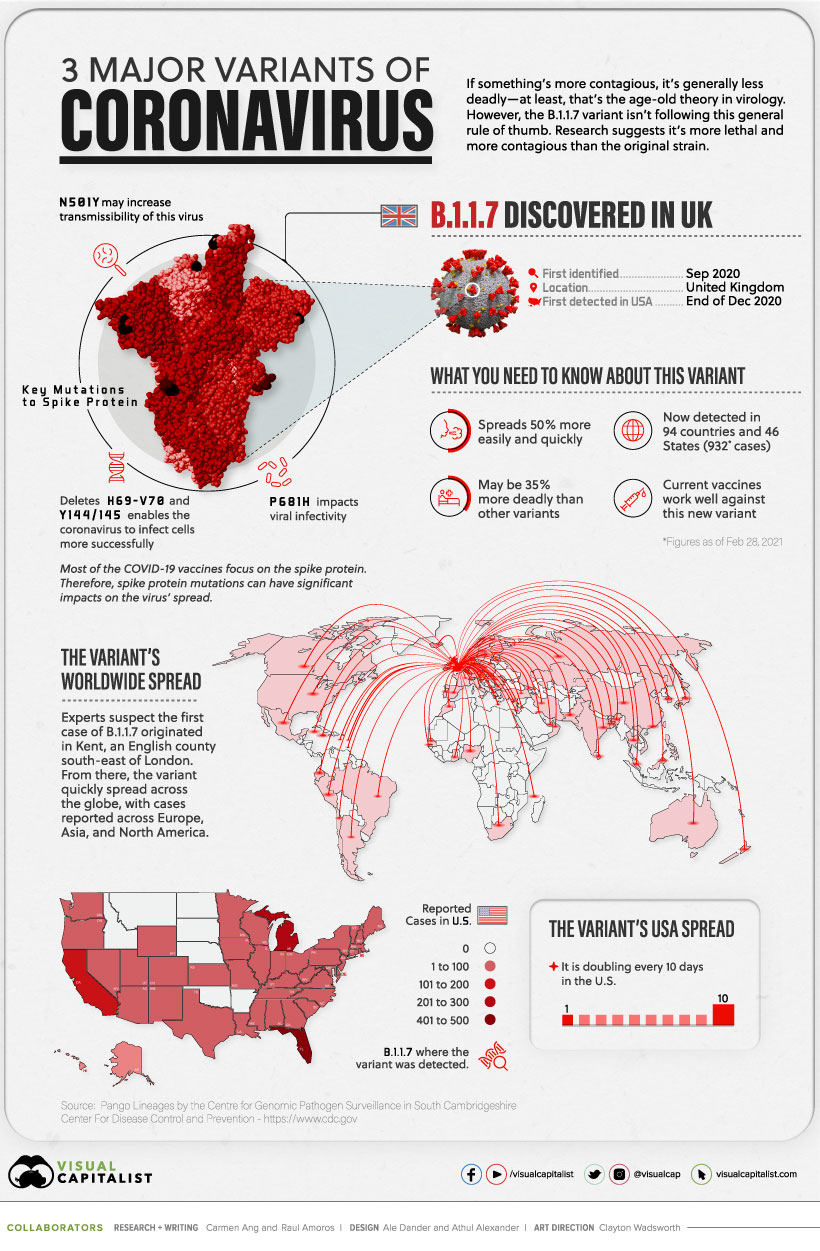
B.1.1.7
The B.1.1.7 variant was detected in the UK in the fall of 2020. By December 2020, it had spread across the globe, with cases emerging across Europe, North America, and Asia.
Currently, the variant has been reported in roughly 94 countries.
Early research suggests it’s 50% more transmissible than other variants, and potentially 35% more deadly than the standard virus. Luckily, studies suggest that some of the existing vaccines work well against it.
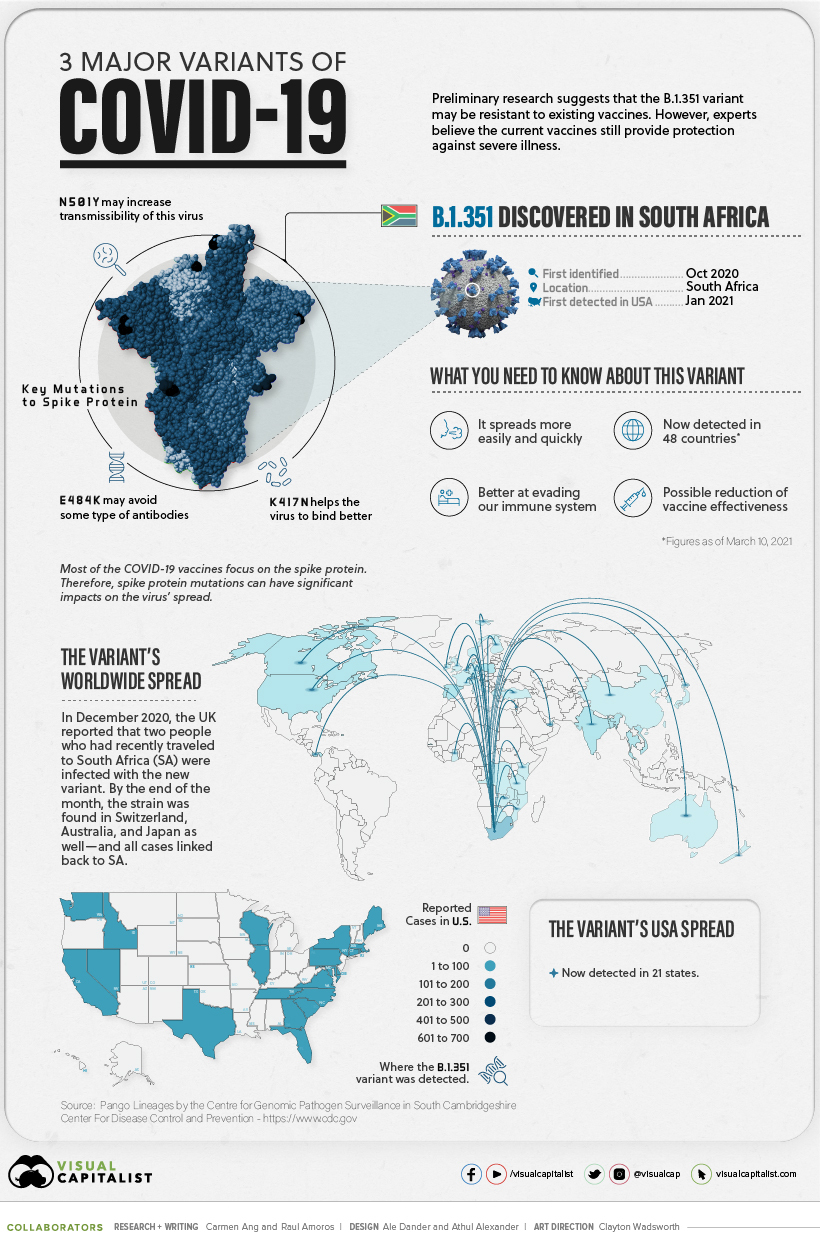
B.1.351
In October 2020, the second major variant was discovered—B.1.351. It was first identified in South Africa, but by end of the year, it had spread to the UK, Switzerland, Australia, and Japan.
There are approximately 48 countries with reported cases, and research suggests several of the existing COVID-19 vaccines may not be as effective against this variant.
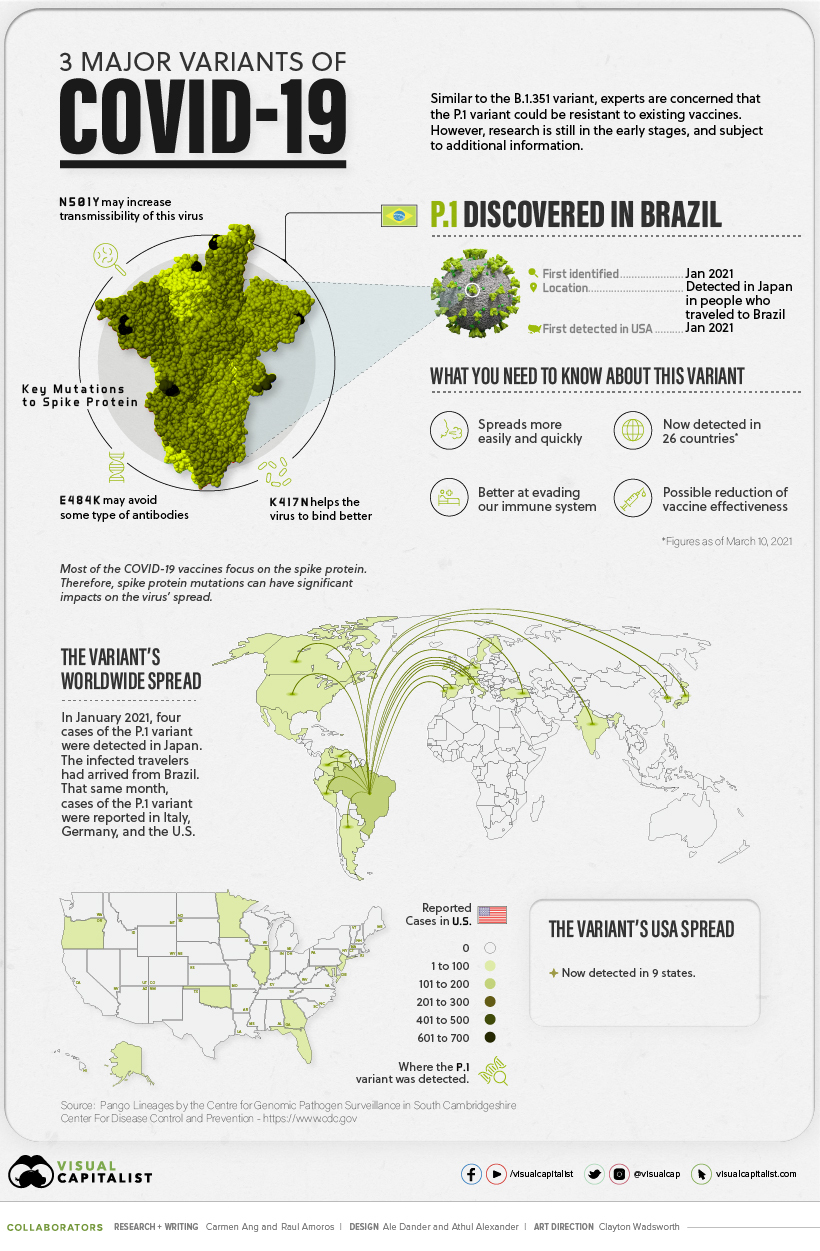
P.1
The P.1 variant was the last to arrive on the scene.
It was first discovered in January 2021, when Japan reported four cases of the variant, which was found in travelers who had arrived from Brazil.
Approximately 25 countries have reported cases of the P.1 variant, and early research suggests this variant is not only more contagious, but could also have the ability to infect people with natural immunity who had already recovered from the original strain.
Still Early Days
While there have been preliminary studies showing a dip in vaccine effectiveness, some experts emphasize that it’s too early to tell for certain. More data is needed to gain a deeper and more accurate understanding.
In the meantime, experts are emphasizing the importance of following our current public health strategies, which include physical distancing, vaccination, washing your hands, and using masks.