The nation’s largest retailer and its largest insurer announced a 10-year partnership to bring together the collective expertise of both companies to provide affordable healthcare to potentially millions of Americans. Set to start next year with 15 Walmart Health locations in Georgia and Florida, the collaboration will initially focus on seniors and Medicare Advantage (MA) beneficiaries, and will include a co-branded MA plan in Georgia. Walmart Health Virtual Care will also be in-network for some UnitedHealthcare beneficiaries. Plans for future years involve expanding the collaboration across commercial and Medicaid plans, as well as including pharmacy, dental, and vision services.
The Gist: We have long wondered if this powerhouse pairing was in the works, as this kind of partnership makes a lot of sense for both parties. While Walmart has reportedly been considering an insurance company acquisition for years, and more recently been dabbling in its own insurance efforts, partnering with UHG provides the retailer with a share of the upside potential of getting into the insurance market without having to fully commit to entering that complex business. And given that 90 percent of Americans live within 10 miles of a Walmart store, and more than half of Americans visit a store every week, Walmart provides UHG with low-cost healthcare access points all over the country, especially important in markets where United’s own Optum physician network is not (yet) present.
Here are 14 health systems with strong operational metrics and solid financial positions, according to reports from Fitch Ratings and Moody’s Investors Service.
1. Advocate Aurora Health has an “AA” rating and stable outlook with Fitch. The health system, dually headquartered in Milwaukee and Downers Grove, Ill., has a strong financial profile and a leading market position over a broad service area in Illinois and Wisconsin, Fitch said. The health system’s fundamental operating platform is strong, the credit rating agency said.
2. AnMed Health has an “AA-” rating and stable outlook with Fitch. The Anderson, S.C.-based system has a leading market share in most service lines, strong operating performance and very solid EBITDA margins, Fitch said.
3. Banner Health has an “AA-” rating and stable outlook with Fitch. The Phoenix-based health system’s core hospital delivery system and growth of its insurance division combine to make it a successful highly integrated delivery system, Fitch said. The credit rating agency said it expects Banner to maintain operating EBITDA margins of about 8 percent on an annual basis, reflecting the growing revenues from the system’s insurance division and large employed physician base.
4. Bon Secours Mercy Health has an “AA-” rating and stable outlook with Fitch. The Cincinnati-based health system has a broad geographic footprint as one of the five largest Catholic health systems in the U.S., a good payer mix and a leading or near leading market share in eight of its eleven markets in the U.S., Fitch said.
5. Lincoln, Neb.-based Bryan Health has an “AA-” rating and stable outlook with Fitch. The health system has a leading and growing market position, very strong cash flow and a strong financial position, Fitch said. The credit rating agency said Bryan Health has been resilient through the COVID-19 pandemic and is well-positioned to accommodate additional strategic investments.
6. Franciscan Alliance has an “AA” rating and stable outlook with Fitch. The Mishawaka, Ind.-based health system has a very strong cash position and maintains leading market shares in seven of its nine defined primary service areas, Fitch said. The health system benefits from a good payer mix, the credit rating agency said.
7. Gundersen Health System has an “AA-” rating and stable outlook with Fitch. The La Crosse, Wis.-based health system has strong balance sheet metrics and a leading market position and expanding operating platform in its service area, Fitch said. The credit rating agency expects the health system to return to strong operating performance as it emerges from disruption related to the COVID-19 pandemic.
8. Hackensack Meridian Health has an “AA-” rating and stable outlook with Fitch. The Edison, N.J.-based health system has shown consistent year-over-year increases in market share and has a solid liquidity position, Fitch said.
9. Falls Church, Va.-based Inova Health System has an “Aa2” rating and stable outlook with Moody’s. The health system has a consistently strong operating cash flow margin and ample balance sheet resources, Moody’s said. Inova’s financial excellence will remain undergirded by its favorable regulatory and economic environment, the credit rating agency said.
10. Salt Lake City-based Intermountain Healthcare has an “Aa1” rating and stable outlook with Moody’s. The health system has exceptional credit quality, which will continue to benefit from its leading market position in Utah, Moody’s said. The credit rating agency said the health system’s merger with Broomfield, Colo.-based SCL Health will give Intermountain greater geographic reach.
11. Omaha-based Nebraska Medicine has an “AA-” rating and stable outlook with Fitch. The health system has a strong market position and is the only public academic provider in Nebraska with high acuity services, Fitch said. The health system continues to generate positive operating cash flow levels, and it has modest flexibility to absorb additional debt, according to the credit rating agency.
12. Fort Wayne, Ind.-based Parkview Health has an “Aa3” rating and stable outlook with Moody’s. The health system has a leading market position with expansive tertiary and quaternary clinical services in northeastern Indiana and northwestern Ohio, Moody’s said. The credit rating agency said the stable outlook reflects management’s ability to generate strong operating performance during the pandement and with less favorable reimbursement rates.
13. UnityPoint Health has an “AA-” rating and stable outlook with Fitch. The Des Moines, Iowa-based health system has strong leverage metrics and cash position, Fitch said. The credit rating agency expects the health system’s balance sheet and debt service coverage metrics to remain robust.
14. Yale New Haven (Conn.) Health has an “AA-” rating and stable outlook with Fitch. The health system’s turnaround efforts, brand recognition and market presence will help it return to strong operating results, Fitch said.
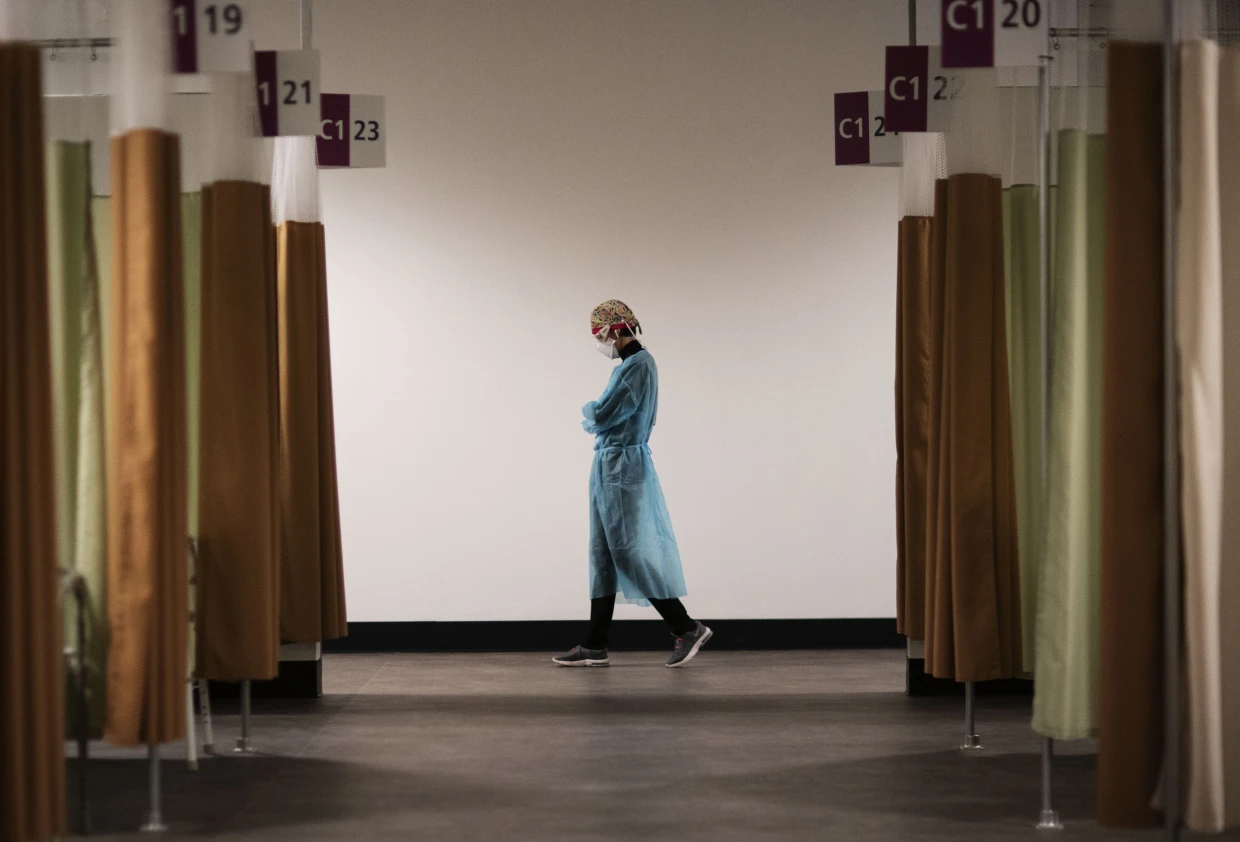
Working as a travel nurse in the early days of the Covid pandemic was emotionally exhausting for Reese Brown — she was forced to leave her young daughter with her family as she moved from one gig to the next, and she watched too many of her intensive care patients die.
“It was a lot of loneliness,” Brown, 30, said. “I’m a single mom, I just wanted to have my daughter, her hugs, and see her face and not just through FaceTime.”
But the money was too good to say no. In July 2020, she had started earning $5,000 or more a week, almost triple her pre-pandemic pay. That was the year the money was so enticing that thousands of hospital staffers quit their jobs and hit the road as travel nurses as the pandemic raged.
Two years later, the gold rush is over. Brown is home in Louisiana with her daughter and turning down work. The highest paid travel gigs she’s offered are $2,200 weekly, a rate that would have thrilled her pre-pandemic. But after two “traumatic” years of tending to Covid patients, she said, it doesn’t feel worth it.
“I think it’s disgusting because we went from being praised to literally, two years later, our rates dropped,” she said. “People are still sick, and people are still dying.”
The drop in pay doesn’t mean, however, that travel nurses are going to head back to staff jobs. The short-lived travel nurse boom was a temporary fix for a long-term decline in the profession that predates the pandemic. According to a report from McKinsey & Co., the United States may see a shortage of up to 450,000 registered nurses within three years barring aggressive action by health care providers and the government to recruit new people. Nurses are quitting, and hospitals are struggling to field enough staff to cover shifts.
Nine nurses around the country, including Brown, told NBC News they are considering alternate career paths, studying for advanced degrees or exiting the profession altogether.
“We’re burned out, tired nurses working for $2,200 a week,” Brown said. People are leaving the field, she said, “because there’s no point in staying in nursing if we’re expendable.”
$124.96 an hour
Travel nursing seems to have started as a profession, industry experts say, in the late 1970s in New Orleans, where hospitals needed to add temporary staff to care for sick tourists during Mardi Gras. In the 1980s and the 1990s, travel nurses were often covering for staff nurses who were on maternity leave, meaning that 13-week contracts become common.
By 2000, over a hundred agencies provided travel contracts, a number that quadrupled by the end of the decade. It had become a lucrative business for the agencies, given the generous commissions that hospitals pay them. A fee of 40 percent on top of the nurse’s contracted salary is not unheard of, according to a spokesperson for the American Health Care Association, which represents long-term care providers.
Just before the pandemic, in January 2020, there were about 50,000 travel nurses in the U.S., or about 1.5 percent of the nation’s registered nurses, according to Timothy Landhuis, vice president of research at Staffing Industry Analysts, an industry research firm. That pool doubled in size to at least 100,000 as Covid spread, and he says the actual number at the peak of the pandemic may have far exceeded that estimate.
By 2021, travel nurses were earning an average of $124.96 an hour, according to the research firm — three times the hourly rate of staff nurses, according to federal statistics.
That year, according to the 2022 National Health Care Retention & RN Staffing Report from Nursing Solutions Inc., a nurse recruiting firm, the travel pay available to registered nurses contributed to 2.47% of them leaving hospital staff jobs.
But then, as the rate of deaths and hospitalizations from Covid waned, the demand for travel nurses fell hard, according to industry statistics, as did the pay.
Demand dropped 42 percent from January to July this year, according to Aya Healthcare, one of the largest staffing firms in the country.
That doesn’t mean the travel nurses are going back to staff jobs.
Brown said she’s now thinking about leaving the nursing field altogether and has started her own business. Natalie Smith of Michigan, who became a travel nurse during the pandemic, says she intends to pursue an advanced degree in nursing but possibly outside of bedside nursing.
Pamela Esmond of northern Illinois, who also became a travel nurse during the pandemic, said she’ll keep working as a travel nurse, but only because she needs the money to retire by 65. She’s now 59.
“The reality is they don’t pay staff nurses enough, and if they would pay staff nurses enough, we wouldn’t have this problem,” she said. “I would love to go back to staff nursing, but on my staff job, I would never be able to retire.”
The coronavirus exacerbated issues that were already driving health care workers out of their professions, Landhuis said. “A nursing shortage was on the horizon before the pandemic,” he said.
According to this year’s Nursing Solutions staffing report, nurses are exiting the bedside at “an alarming rate” because of rising patient ratios, and their own fatigue and burnout. The average hospital has turned over 100.5% of its workforce in the past five years, according to the report, and the annual turnover rate has now hit 25.9%, exceeding every previous survey.
There are now more than 203,000 open registered nurse positions nationwide, more than twice the number just before the pandemic in January 2020, according to Aya Healthcare.
An obvious short-term solution would be to keep using travel nurses. Even with salaries falling, however, the cost of hiring them is punishing.
LaNelle Weems, executive director of Mississippi Hospital Association’s Center for Quality and Workforce, said hospitals can’t keep spending like they did during the peak of the pandemic.
“Hospitals cannot sustain paying these exorbitant labor costs,” Weems said. “One nuance that I want to make sure you understand is that what a travel agency charges the hospitals is not what is paid to the nurse.”
Ultimately, it’s the patients who will suffer from the shortage of nurses, whether they are staff or gig workers.
“Each patient added to a hospital nurse’s workload is associated with a 7%-12% increase in hospital mortality,” said Linda Aiken, founding director of the University of Pennsylvania’s Center for Health Outcomes and Policy Research.
Nurses across the country told NBC News that they chose the profession because they cared about patient safety and wanted to be at the bedside in the first line of care.
“People say it’s burnout but it’s not,” Esmond said about why nurses are quitting. “It’s the moral injury of watching patients not being taken care of on a day-to-day basis. You just can’t take it anymore.”
A Kaiser Health News analysis of federal data published Sept. 9 highlights an increasing trend among hospitals — establishing independent, nonprofit health center “look-alikes” for primary care patients to improve their financial picture.
Federally qualified health center look-alikes, as designated by the federal government, deliver primary care services to underserved communities. They receive federally qualified health center prospective payment system reimbursement through CMS — a higher rate than if the sites were owned by the hospitals — as well as help with the recruitment and retention of primary care providers via HHS’ National Health Service Corps.
However, they don’t receive health center program funding from HHS to cover operational expenses.
Some hospitals increasingly view look-alikes as a strategy to help with their financial picture, since they can divert primary care patients without urgent needs to look-alike clinics from expensive emergency rooms, according to Kaiser Health News.
The Kaiser Health News analysis published Sept. 9 found that at least eight hospitals and health systems have converted or built new clinics designated as look-alikes from 2019 through 2022. This includes Mount Carmel, Ill.-based Wabash General Hospital, Beverly Hospital in Montebello, Calif., and Parrish Medical Center in Titusville, Fla., among others.
To read the full Kaiser Health News report, click here.
Survey responses from more than 161,000 employees were analyzed to determine the best workplaces in the healthcare industry. To be considered for the list, organizations were required to be Great Place to Work-Certified and be in the healthcare industry. Learn more about the methodology here.
Below are the nine best large health systems to work for, ordered by their corresponding number in the overall list of 30 organizations. Health systems with 1,000 or more employees were considered for the large category.
1. Texas Health Resources (Arlington)
3. Southern Ohio Medical Center (Portsmouth)
5. Northwell Health (New Hyde Park, N.Y.)
6. Baptist Health South Florida (Coral Gables)
7. OhioHealth (Columbus)
8. Scripps Health (San Diego)
9. WellStar Health System (Marietta, Ga.)
10. Atlantic Health System (Morristown, N.J.)
21. BayCare Health System (Clearwater, Fla.)
Fortune and Great Place to Work also released a list of the best small and medium healthcare organizations to work for. Organizations with up to 999 employees were considered for the small and medium category. No hospitals or health systems were listed in that category.
New York Gov. Kathy Hochul on Sept. 9 declared a state of emergency amid evidence that polio is spreading in communities around the state. The move unlocks federal resources to help the state respond and boost vaccination rates.
Under the declaration, pharmacists, emergency medical personnel and midwives can now administer polio vaccines. The executive order also requires providers to send polio vaccination data to the state’s health department.
“On polio, we simply cannot roll the dice,”said Mary Bassett, MD, health commissioner at the state’s health department. “If you or your child are unvaccinated or not up to date with vaccinations, the risk of paralytic disease is real. I urge New Yorkers to not accept any risk at all.”
The declaration came the same day state health officials reported that the virus had been detected in wastewater samples from Nassau County. Officials have also found the virus in sewage samples from New York City, Orange County, Sullivan County and Rockland County, where the nation’s first polio case in nearly a decade was confirmed July 21 in an unvaccinated man. Health officials have suggested the Rockland County case may just be the “tip of the iceberg” with hundreds of other cases potentially going undetected in the state.
The threat of polio’s resurgence is magnified by the many pockets of unvaccinated residents throughout the state. New York’s polio vaccination rate is 78.96 percent. That figure is lower in many of the counties where the virus has been detected in wastewater. In Rockland County, for example, the polio vaccination rate is 60.3 percent, state data shows. Nationwide, polio vaccination coverage sits at about 93 percent, according to the CDC.