So far, 2023 is shaping up to be a slightly better year for hospital performance, but it comes on the heels of unprecedented financial difficulties for the sector.
In the graphic above, we evaluated nearly 30 years of historical data from Kaufman Hall and the American Hospital Association to provide a broader perspective on hospital operating margins over time. 2020 and 2022 have been the only years in which a majority of hospitals—53 percent—posted a negative operating margin.
During the most comparable periods of recent economic hardship, the “dot-com bubble burst” of the late 1990s and the 2009 Great Recession, the share of hospitals with negative operating margins amounted to only 42 and 32 percent, respectively.
With this context, hospitals’ current financial distress is more severe than anything we’ve seen in the past three decades.
Healthcare is clearly no longer recession-proof: a four percent operating margin—the level needed for health systems to not only sustain operations but also invest in growth—feels even more elusive as labor costs remain high, surgical care continues to shift to outpatient settings, the second half of the Baby-Boom generation ages into Medicare, and deep-pocketed competitors compete for profitable services.
A detailed report, published by a group of organizations including the American Antitrust Institute, provides one of the highest-quality examinations of the growth of private equity (PE)-backed physician practices, and the impact of this growth on market competition and healthcare prices.
From 2012 to 2021, the annual number of practice acquisitions by private equity groups increased six-fold, and the number of metropolitan areas in which a single PE-backed practice held over 30 percent market share rose to cover over one quarter of the country. (Check out figure 3B at the bottom of page 20 in the report to see if you live in one of those markets.)
The study also found an association between PE practice acquisitions and higher healthcare prices and per-patient expenditures. In highly concentrated markets, certain specialties, like gastroenterology, saw prices rise by as much as 18 percent.
The Gist: As the report highlights, one of the greatest barriers to assessing PE’s impact on physician practices is the lack of transparency around acquisitions and ownership structures. This analysis brings us closer to understanding the scope of the issue, and makes a strong case for regulatory and legislative intervention.
Recent proposed changes to federal premerger disclosure requirements offer a good start, but many practice acquisitions are still too small to flag review, and slowing future acquisitions will do little to unwind the market concentration already emerging.
PE is also not the sole actor contributing to healthcare consolidation, and proposed remedies may target the activities of payers and health systems considered anti-competitive as well.
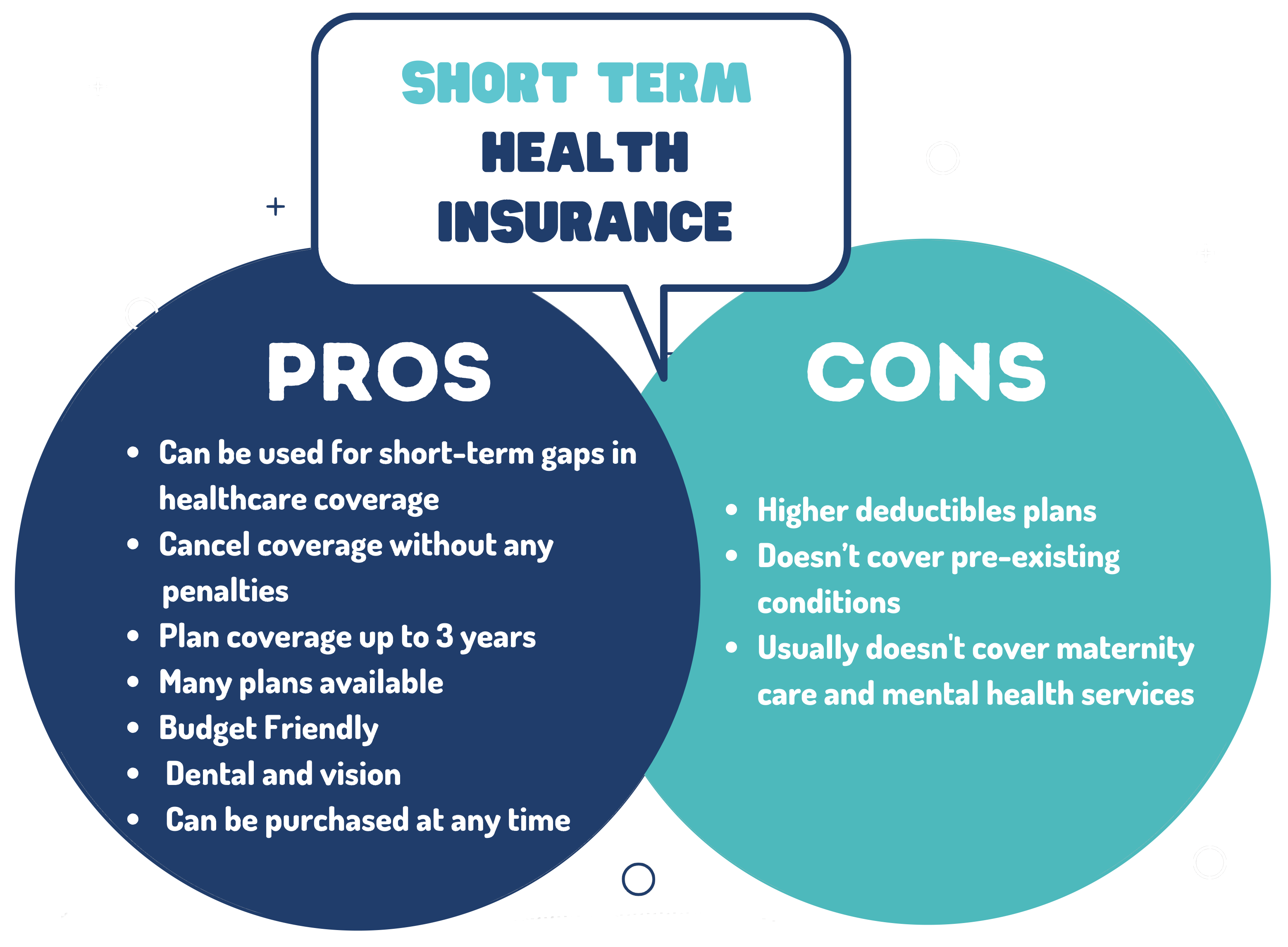
Last Friday, the Department of Health and Human Services, the Treasury Department, and the Department of Labor jointly issued several proposed rules to shore up consumer healthcare protections, including reversal of a Trump administration policy that allowed consumers to enroll in short-term health plans, which were intended to serve as limited coverage options during transitional periods, for up to three years. Approximately 3M people were enrolled in these plans in 2019.
A new rule would limit consumer access to these plans to just three months, with an optional one-month extension, while also requiring payers to disclose clearly how their plans fall short of comprehensive health insurance.
The Gist: In an expected move, theBiden administration continues its unwinding of the Trump-era policies it sees as undermining the Affordable Care Act’s (ACA’s) mission of guaranteeing robust, accessible insurance for all.
Short-term plans, which were granted an exemption from the ACA requirement that health plans cover ten essential health benefits, have been found to discriminate against people with pre-existing conditions, revoke coverage for enrollees retroactively, and generate excess surprise bills due to their limited networks.
Earlier this week, the Centers for Medicare and Medicaid Services (CMS) issued a proposal to remedy its four years of payment cuts to the more than 1,600 hospitals participating in the 340B Drug Pricing Program through one-time, lump-sum payments that will total roughly $9B.
In 2018, CMS reduced drug reimbursement to 340B covered-entity hospitals by nearly 30 percent, in an attempt to align reimbursement with hospitals’ actual drug acquisition costs. The Supreme Court overturned those cuts in 2022, ruling that the Department of Health and Human Services (HHS) had violated rulemaking procedure. As CMS rulemaking on Medicare payment must be budget-neutral, the agency will offset the remedy payments with a 0.5 percent cut to all hospitals for non-drug items and services covered under the Hospital Outpatient Prospective Payment System (OPPS) over the next 16 years. Stakeholders have until September 5th to comment on the proposed rule. Once the final rule is published later this year, CMS plans to repay 340B participant hospitals within 60 days of their application for remedy.
The Gist: After worries about how last year’s Supreme Court ruling would be implemented, 340B participant hospitals will be relieved to receive their payment corrections up front instead of over time, especially given current margin challenges.
But while this issue is now set to be resolved, other critical decisions about the 340B program’s fate are pending before courts. Earlier this year, Bayer and EMD Serono became the 20th and 21st drugmakers to restrict discounts to contract pharmacies, following an appellate court decision in January that sided with the pharmaceutical manufacturers.
Meanwhile, appellate courts in other jurisdictions are set to hear at least two more cases on the issue, amid conflicting rulings about whether HHS can enforce contract pharmacy discounts.
Pay attention to the media coverage around artificial intelligence, and it’s easy to get the sense that technologies such as chatbots pose an “existential crisis” to everything from the economy to democracy.
These threats are real, and proactive regulation is crucial. But it’s also important to highlight AI’s many positive applications, especially in health care.
Consider the Mayo Clinic, the largest integrated, nonprofit medical practice in the world, which has created more than 160 AI algorithms in cardiology, neurology, radiology and other specialties. Forty of those have already been deployed in patient care.
To better understand how AI is used in medicine, I spoke with John Halamka, a physician trained in medical informatics who is president of Mayo Clinic Platform. As he explained to me, “AI is just the simulation of human intelligence via machines.”
Halamka distinguished between predictive and generative AI. The former involves mathematical models that use patterns from the past to predict the future; the latter uses text or images to generate a sort of human-like interaction.
It’s that first type that’s most valuable to medicine today. As Halamka described, predictive AI can look at the experiences of millions of patients and their illnesses to help answer a simple question: “What can we do to ensure that you have the best journey possible with the fewest potholes along the way?”
For instance, let’s say someone is diagnosed with Type 2 diabetes. Instead of giving generic recommendations for anyone with the condition, an algorithm can predict the best care plan for that patient using their age, geography, racial and ethnic background, existing medical conditions and nutritional habits.
This kind of patient-centered treatment isn’t new; physicians have long been individualizing recommendations. So in this sense, predictive AI is just one more tool to aid in clinical decision-making.
The quality of the algorithm depends on the quantity and diversity of data. I was astounded to learn that the Mayo Clinic team has signed data-partnering agreements with clinical systems across the United States and globally, including in Canada, Brazil and Israel. By the end of 2023, Halamka expects the network of organizations to encompass more than 100 million patients whose medical records, with identifying information removed, will be used to improve care for others.
Predictive AI can also augment diagnoses. For example, to detect colon cancer, standard practice is for gastroenterologists to perform a colonoscopy and manually identify and remove precancerous polyps. But some studies estimate that 1 in 4 cancerous lesions are missed during screening colonoscopies.
Predictive AI can dramatically improve detection. The software has been “trained” to identify polyps by looking at many pictures of them, and when it detects one during the colonoscopy, it alerts the physician to take a closer look. One randomized controlled trial at eight centers in the United States, Britain and Italy found that using such AI reduced the miss rate of potentially cancerous lesions by more than half, from 32.4 percent to 15.5 percent.
Halamka made a provocative statement that within the next five years, it could be considered malpractice not to use AI in colorectal cancer screening.
But he was also careful to point out that “it’s not AI replacing a doctor, but AI augmenting a doctor to provide additional insight.” There is so much unmet need that technology won’t reduce the need for health-care providers; instead, he argued, “we’ll be able to see more patients and across more geographies.”
Generative AI, on the other hand, is a “completely different kind of animal,” Halamka said. Some tools, such as ChatGPT, are trained on un-curated materials found on the internet. Because the inputs themselves contain inaccurate information, the models can produce inappropriate and misleading text. Moreover, whereas the quality of predictive AI can be measured, generative AI models produce different answers to the same question each time, making validation more challenging.
At the moment, there are too many concerns over quality and accuracy for generative AI to direct clinical care. Still, it holds tremendous potential as a method to reduce administrative burden. Some clinics are already using apps that automatically transcribe a patient’s visit. Instead of creating the medical record from scratch, physicians would edit the transcript, saving them valuable time.
Though Halamka is clearly a proponent of AI’s use in medicine, he urges federal oversight. Just as the Food and Drug Administration vets new medications, there should be a process to independently validate algorithms and share results publicly. Moreover, Halamka is championing efforts to prevent the perpetuation of existing biases in health care in AI applications.
This is a cautious and thoughtful approach. Just like any tool, AI must be studied rigorously and deployed carefully, while heeding the warning to “first, do no harm.”
Nevertheless, AI holds incredible promise to make health care safer, more accessible and more equitable.
Here is a summary of recent credit downgrades and outlook revisions for hospitals and health systems.
The downgrades and downward revisions reflect continued operating challenges many nonprofit systems are facing, with multiyear recovery processes expected.
Downgrades:
Yale New Haven (Conn.) Health: Operating weakness and elevated debt contributed to the downgrade of bonds held by Yale New Haven (Conn.) Health, Moody’s said May 5. The bond rating slipped from “Aa3” to “A1,” and the outlook was revised to stable from negative.
The system saw a second downgrade as its default rating and that on a series of bonds were revised one notch to “A+” from “AA-” amid continued operating woes, Fitch said June 28.
Not only have there been three straight years of such challenges, but the operating environment continues to cast a pall into the second quarter of the current fiscal year, Fitch said.
UC Health (Cincinnati): The system was downgraded on a series of bonds, Moody’s said May 10.
The move, which involved a lowering from a “Baa2” to “Baa3” grade, refers to such bonds with an overall value of $580 million.
In February, UC Health suffered a similar downgrade from “A” to “BBB+” on its overall rating and on some bonds because of what S&P Global termed “significantly escalating losses.”
UNC Southeastern (Lumberton, N.C.): The system, which is now part of the Chapel Hill, N.C.-based UNC Health network, saw its ratings on a series of bonds downgraded to “BB” amid operating losses and sustained weakness in its balance sheet, S&P Global said June 23.
While UNC Southeastern reported an operating loss of $74.8 million in fiscal 2022, such losses have continued into fiscal 2023 with a $15 million loss as of March 31, S&P Global said. The system had earlier been placed on CreditWatch but that was removed with this downgrade.
Butler (Pa.) Health: The system, now merged with Greensburg, Pa.-based Excela Health to form Independence Health System, saw its credit rating downgraded significantly, falling from “A” to “BBB.”
The move reflects continued operating challenges and low patient volumes, Fitch said June 26.
Such operating challenges, including low days of cash on hand, could result in potential default of debt covenants, Fitch warned.
Outlook revisions:
Redeemer Health (Meadowbrook, Pa.): The system had its outlook revised to negative amid “persistent operating losses,” Fitch Ratings said June 14. The health system, anchored by a 260-bed acute care hospital, reported a $37 million operating loss in the nine months ending March 31, Fitch said.
Thomas Jefferson University (Philadelphia): The June 9 downward revision of its outlook, which includes both the health system and the university’s academic sector, was due to sustained operating weakness, S&P Global said.
IU Health (Indianapolis): While it saw ratings affirmed at “AA,” the 16-hospital system had its outlook downgraded amid persistent inflationary pressures and large capital expense, Fitch said May 31.
UofL Health (Louisville, Ky.): Slumping operating income and low days of cash on hand (42.8 as of March 31) contributed to S&P Global revising its outlook for the six-hospital system to negative May 24.
The latest CPI was a crowd-pleaser: Inflation has plunged from its peak, helping provide relief for consumers.
Beyond the headline, an underlying measure closely watched by economists and the Fed finally began to cool.
Why it matters:
The worst of the inflation crisis looks to be firmly behind us. Price gains appear to be on a path to returning to normal, but there is huge uncertainty around how long that will take, with plenty of hurdles still ahead.
What they’re saying:
“After a punishing stretch of high inflation that eroded consumer’s purchasing power, the fever is breaking,” Bill Adams, chief economist at Comerica Bank, wrote in a note.
While the Fed appears to be on track to tighten by a quarter percentage point two weeks from today, the promising news lowers the odds of further hikes this year.
Details:
Headline CPI rose 3% (or 2.97%, unrounded) in the 12 months through June, the smallest increase since March 2021. That reflects milder price gains for a slew of goods, including food — and outright deflation for other items consumers buy, like airline fares, which fell 8% in June.
The intrigue:
At the same time last year, headline prices skyrocketed by 9%. Now we’re lapping that period, which makes the comparison much more favorable.
Then, commodity prices soared on disruptions from Russia’s invasion of Ukraine. Those prices are sharply lower now, helping the headline figure cool rapidly. Gasoline, for instance, is down nearly 27%.
Those favorable effects will fade in the year-on-year numbers, so don’t be surprised if the headline CPI figure rebounds some in the coming months.
The most encouraging aspect was the core figure, which strips out volatile food and energy costs and is closely followed by policymakers. That rose by just 0.2% in June, the slowest monthly pace since February 2021.
In the past three months, core inflation has risen at a 4.1% annualized pace — down almost a full percentage point from May.
Under the hood, there was notable disinflation across a key sector of the economy monitored by the Fed: core services, excluding shelter. Prices in that category were flat last month, compared to a 0.2% rise in May.
That cooling is happening alongside a still-healthy labor market and solid wage gains (more on this below), which officials worried could stoke inflation in this category.
The Biden administration is eager to tout the progress. “The economy is defying predictions that inflation would not fall absent significant job destruction,” top White House economic adviser Lael Brainard is expected to say this afternoon at the Economic Club of New York, according to prepared remarks.
“Annual inflation has now declined every month for 12 months in a row,” she will say, “and inflation in the United States is now the lowest among G-7 nations … even as our economic recovery from the pandemic has been the strongest.”
The bottom line:
We have been head-faked before by what appeared to be remarkable progress on inflation, notably in the summer of 2001.
With expected cooling in other areas (including shelter, which makes up a big chunk of the index), there is reason to be hopeful this progress could be here to stay.
Today marks the 63rd anniversary of Harper Lee‘s “To Kill a Mockingbird” (1960) — a novel containing truths so universal that they bear repeating in 2023.
“You never really understand a person until you consider things from his point of view … Until you climb inside of his skin and walk around in it.”
“I wanted you to see what real courage is … It’s when you know you’re licked before you begin but you begin anyway and you see it through no matter what. You rarely win, but sometimes you do.”
“People generally see what they look for, and hear what they listen for.”
“The one thing that doesn’t abide by majority rule is a person’s conscience.”
“Sometimes the Bible in the hand of one man is worse than a whisky bottle in the hand of another … There are just some kind of men who — who’re so busy worrying about the next world they’ve never learned to live in this one, and you can look down the street and see the results.”