As the nation’s leading provider of retail healthcare, CVS Health partners with hospitals and health systems in many local markets.
The health systems assist providers at CVS MinuteClinic locations and accept referrals from patients needing a higher level of care. Here are CVS’ clinical affiliates, according to its website:
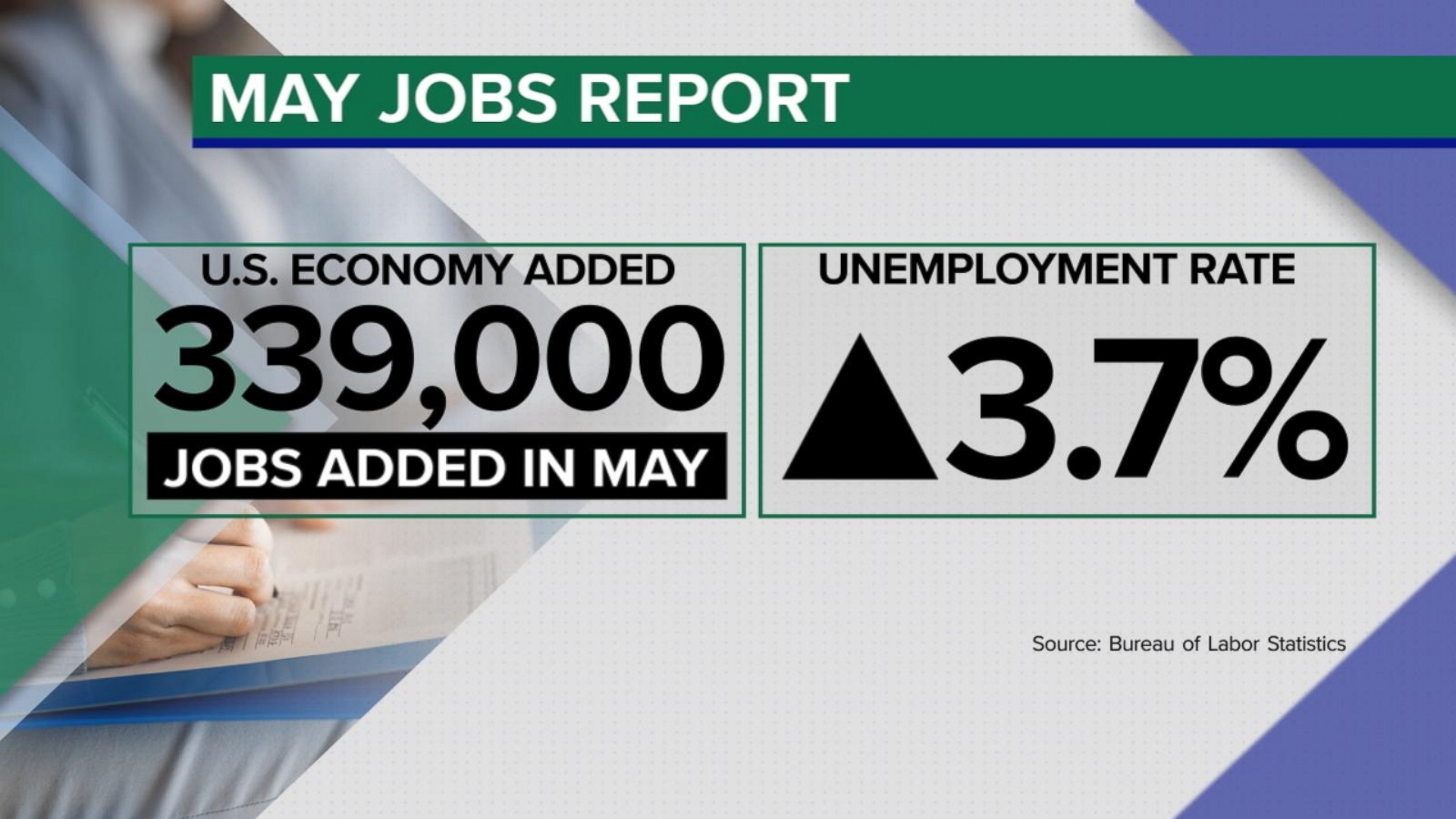
The U.S. economy added 339,000 jobs in May, while the unemployment rate jumped to 3.7% from 3.4%, the Labor Department said Friday.
Why it matters:
Job gains came in well above forecasters’ expectations — the latest sign that the economy is still underpinned by a hot labor market.
Economists expected a gain of 190,000 jobs last month. The May jobs figures are a pickup from the 294,000 added in April, which was revised up by 41,000. Job gains in March were revised up, too.
Details:
Economic policymakers have kept a close eye on other details from the payrolls report — whether more Americans are joining the workforce and how quickly pay is rising.
The labor force participation rate — the share of workers with a job or hunting for one — held at 62.6% in May.
Meanwhile, average hourly earnings, a measure of pay, rose by 0.3% in May. Compared to the same period a year ago, wages are up 4.3%.
What we’re watching:
The May jobs report is among the final data points Federal Reserve officials will consider before deciding whether to continue the interest rate hiking campaign that began more than a year ago.
Inflation remains too high, and there are concerns that rapid price gains are being fueled by the tight labor market and strong consumer demand.
Still, a top Fed official this week signaled the central bank may skip a rate hike at its meeting later this month.
A phenomenon that defined the pandemic-era labor market is over: the Great Resignation — workers furiously quitting for new, likely higher paying jobs — is a thing of the past.
Why it matters:
The historic surge of quitters was a symptom of an on-fire labor market, where demand for workers far outstripped supply of them.
Now the job market may be entering a different era — one that more closely resembles pre-pandemic times.
By the numbers:
The quits rate fell to 2.4% in April, according to the Job Openings and Labor Turnover Survey, released this morning.
That is just a tick (0.1 percentage point) higher than the quits rate in February 2020 — and roughly in line with the average quits rate in 2019.
Even leisure and hospitality workers, once the poster child for the quits boom, are returning to pre-pandemic norms: the quits rate in this segment hit 4.6% in April — very close to the January 2020 rate of 4.4%, and well-below the peak 5.8% recorded last summer.
What they’re saying:
“We are pretty much back to a strong, robust labor market, but one that is no longer overheating,” says Julia Pollak, an economist at ZipRecruiter.
“One that isn’t plagued by widespread labor shortages that are wreaking havoc across the economy, and causing firms to offer off-cycle wage increases and dispense of all hiring requirements. The deck isn’t totally stacked in jobseekers‘ favor anymore.”
Flashback:
At the height of the Great Resignation, the overall quits rate most recently peaked at 3% in April 2022, when there were roughly 4.5 million quits in a single month.
Turnover of that magnitude had never been seen before — at least not since the Labor Department started collecting the data in 2000.
Workers were in such high demand that they felt confident enough to ditch current gigs for new (likely higher paying) ones.
The bottom line:
Americans who did job hop over the past few years have seen heftier pay gains. But that phenomenon, too, is fading — another sign of some heat coming off the labor market.
Job-changers saw annual pay grow more than 13% in April, according to payroll professor ADP — more than double the annual rate of job-stayers.
Still that was the slowest pace of growth since November 2021.
More than a year after the regulation went into effect, compliance with the hospital price transparency rule remains low, as hospitals are hesitant to invest in necessary software and resources.
The Centers for Medicare and Medicaid Services (CMS) established the hospital price transparency rule to help individuals know the cost of a hospital item or service before receiving it.
CMS proposed the price transparency rule in the 2020 Medicare Outpatient Prospective Payment System (OPPS) and Ambulatory Surgical Center (ASC) Payment System Proposed Rule. The rule came in response to rising healthcare costs. Policymakers implemented regulations that give consumers more control over what they pay for healthcare services.
The rule went into effect on January 1, 2021, but hospitals have been slow to comply with the regulation. Without consistent compliance from hospitals and health systems, the rule does little to protect consumers from high healthcare prices.
WHAT IS THE PRICE TRANSPARENCY RULE?
The price transparency rule requires hospitals to publish the costs of their items and services on a publicly available website in two ways.
First, hospitals must have a single machine-readable digital file with standard charges for all their items and services. Standard charges include gross charges, discounted cash prices, payer-specific negotiated chargers, and de-identified minimum and maximum negotiated charges.
Hospitals must also display standard charges of at least 300 shoppable services that consumers can schedule in advance. That information must be displayed in a consumer-friendly format that includes plain language descriptions. Hospitals should also group the services with related ancillary services.
Hospitals may offer an online price estimator tool instead of publishing standard charges for the most common shoppable services. According to CMS, the price estimator tool must provide estimates for as many of the 70 CMS-specified shoppable services that the hospital offers and any additional shoppable services to reach a total of 300 services.
In addition, the tool must allow consumers to receive an estimate of the amount they will have to pay for a given service. Hospitals must display the price estimator tool on their websites and make it accessible to the public for free. Consumers also need to be able to access the tool without creating a user account.
CMS established an enforcement plan to ensure hospitals comply with the price transparency rule. The agency planned to evaluate complaints made by individuals or entities, review analyses of noncompliance, and audit hospital websites. However, more than one year after the regulation went into effect, hospitals are still not complying with the price transparency rule.
PRICE TRANSPARENCY RULE COMPLIANCE
The price transparency regulation received immediate pushback from hospital and provider groups. Before the policy went into effect, the American Hospital Association (AHA) sued HHS over the rule, stating that it would confuse consumers and increase prices.
The Kaiser Family Foundation (KFF) analyzed data from the two largest hospitals in each state and the District of Columbia and found similar trends. For example, 80 percent of the hospitals provided gross charge information on a price estimator tool and a machine-readable file, but only 35 of the 102 hospitals displayed payer-specific negotiated rates.
According to an Insights analysis from Xtelligent Healthcare Media, hospital networks frequently had inaccessible machine-readable files and shoppable services. In addition, many hospitals required patients to provide personally identifiable information in exchange for pricing data and had machine-readable files that lacked the required charges.
PatientRightsAdvocate.org has been tracking hospital compliance with the price transparency rule since May 2021. Between May and July, the organization found that out of 500 randomly selected US hospitals, only 5.6 percent were compliant with the rule.
Under the 2022 Medicare OPPS rule, CMS shared the penalties for not complying with the price transparency rule. Hospitals with less than 30 beds would receive penalties of $300 per day, while hospitals with 31 or more beds would receive a $10 per bed per day penalty, with a maximum daily fine of $5,500.
However, hospitals have not received any penalties for noncompliance as of February 2022. CMS has sent around 345 warning notices to noncompliant hospitals since the rule went into effect, the agency told Becker’s Hospital Review.
The threat of financial penalties does not seem to be enough to ensure compliance, though.
Shortly after the rule took effect, noncompliant hospitals said they were not fully complying due to resource constraints and a limited understanding of the rule. Some hospitals also mentioned that they were waiting to see how their competitors responded to the rule before achieving compliance.
More than one year later, in April 2022, financial leaders expressed similar concerns regarding compliance. Revenue cycle leaders told KLAS that a top barrier to achieving compliance was the confusing and complex regulations included in the rule.
Price transparency compliance also requires significant investment in software and outside resources, the KLAS report noted. As hospitals and health systems struggle financially due to the COVID-19 pandemic, investing in price transparency software may not be a top priority.
In addition, revenue cycle leaders reported experiencing difficulties with the software used to publish machine-readable files and a master list of prices online.
Until CMS starts delivering monetary penalties for noncompliance or adjusts the regulation to reduce the financial burden for health systems, hospital compliance with the price transparency rule will likely remain slim.
Inflation, labor pressures, and general economic uncertainty have created significant financial strain for hospitals in the wake of the COVID pandemic. Compressed operating margins and weakened liquidity have left many hospitals in a precarious economic situation, with some entities deciding to delay or even cancel planned capital expenditures or capital raising. Given these tumultuous times, hospital entities could look to the realm of the higher education sector for a playbook on how to leverage non-core assets to unlock significant unrealized value and strengthen financial positions, in the form of public-private partnerships.
These structures, also known as P3s, involve collaborative agreements between public entities, like hospitals, and private sector partners who possess the expertise to unlock the value of non-core assets. A special purpose vehicle (SPV) is created, with the sole purpose of delivering the responsibilities outlined under the project agreement. The SPV is typically owned by equity members. The private sector would be responsible for raising debt to finance the project, which is secured by the obligations of the project agreement (and would be non-recourse to the hospital). Of note, the SPV undergoes the rating process, not the hospital entity. Even more importantly, the hospital retains ownership of the asset while benefiting from the expertise and resources of the private sector.
Hospitals can utilize P3s to capitalize on already-built assets, in what is known as a “brownfield” structure. A brownfield structure would typically result in an upfront payment to the hospital in exchange for the right of a private entity to operate the asset for an agreed-upon term. These upfront payments can range from tens of millions to hundreds of millions of dollars.
Alternatively, hospitals can engage in “greenfield” structures where the underlying asset is either not yet built or needs significant capital investment. Greenfield structures typically do not result in an upfront payment to the hospital entity. Instead, (in the example of a new build) private partners would typically design, build, finance, operate and maintain the asset. The hospital still retains ownership of the underlying asset at the completion of the agreed upon term.
P3 structures can be individually tailored to suit the unique needs of the hospital entity, and the resulting benefits are multifaceted. Financially, hospitals can increase liquidity, lower operating expenses, increase debt capacity, and create headroom for financial covenants. These partnerships provide a means to raise funds without directly accessing the capital markets or undergoing the rating process. Upfront payments represent unrestricted funds and can be used as the hospital entity sees fit to further its core mission. Operationally, infrastructure P3s offer hospitals the opportunity to address deferred maintenance needs, which may have accumulated over time. Immediate capital expenditure on infrastructure facilities can enhance reliability and efficiency and contribute to meeting carbon reduction or sustainability goals. Furthermore, these structures provide a means for the hospital to transfer a meaningful amount of risk to private partners via operation and maintenance agreements.
For years, various colleges and universities have adopted the P3 model, which is emerging as a viable solution for hospitals as well. Examples of recent structures in the higher education sector include:
Fresno State University, which partnered with Meridiam (an infrastructure private equity fund) and Noresco (a design builder) to deliver a new central utility plant. The 30-year agreement involved long-term routine and major maintenance obligations from the operator, with provisions for key performance indicators and performance deductions inserted to protect the university. Fresno State is not required to begin making availability payments until construction is completed.
The Ohio State University, which secured a $483 million upfront payment in exchange for the right of a private party to operate and maintain its parking infrastructure. The university used the influx of capital to hire key faculty members and to invest in their endowment.
The University of Toledo, which received an approximately $60 million upfront payment in exchange for a 35-year lease and concession agreement to a private operator. The private team will be responsible for operating and maintaining the university’s parking facilities throughout the term of the agreement.
Ultimately, healthcare entities can learn from the successful implementation of infrastructure P3 structures in the higher education sector. The experiences of Fresno State, The Ohio State University, and the University of Toledo (among others) serve as compelling examples of the transformative potential of P3s in the healthcare sector. By unlocking the true value of non-core assets through partnerships with the private sector, hospitals can reinforce their financial stability, meet sustainability goals, reduce risk, and shift valuable focus back to the core mission of providing high-quality healthcare services.
Author’s note: Implementing P3 structures requires careful consideration and expert guidance. Given the complex nature of these partnerships, hospitals can greatly benefit from the support of experienced advisors to navigate the intricacies of the process. KeyBank and Cain Brothers specialize in guiding entities through P3 initiatives, providing valuable expertise and insight. For additional information, please refer to a recording of our recent webinar and associated summary, which can be accessed here: https://www.key.com/businesses-institutions/business-expertise/articles/public-private-partnerships-can-unlock-hospitals-hiddenvalue.html
Less than a month after CVS Health acquired Oak Street Health, the primary care provider plans to expand into four more states.
The company plans to open value-based primary care centers in Little Rock, Arkansas; Des Moines and Davenport, Iowa; Kansas City, Kansas and Richmond, Virginia, beginning this summer.
Oak Street Health will operate centers in 25 states by the end of the year.
The provider also aims to open new centers in existing markets this year with additional centers planned for Arizona, Colorado, Georgia, Illinois, Indiana, Louisiana, New York, Ohio and Pennsylvania.
CVS finalized its $10.6 billion acquisition of the Medicare-focused primary care company in early May, picking up, at the time, about 169 medical centers in 21 states.
The acquisition significantly broadens CVS Health’s primary care footprint and the retail pharmacy giant said the deal will improve health outcomes and reduce costs for patients, particularly for those in underserved communities.
The two deals will help advance the health giant’s push into value-based care and mark its latest moves to get further into healthcare services.
Oak Street specializes in treating Medicare Advantage patients and its network of clinics is expected to grow to over 300 centers by 2026.
The provider says it developed an integrated care model that incorporates behavioral healthcare and social determinants support and patients can access care in-center, in-home and through telehealth appointments.
Oak Street Health says it has reduced patient hospital admissions by approximately 51% compared to Medicare benchmarks, and driven a 42% reduction in 30-day readmission rates and a 51% reduction in emergency department visits.
“One of the most critical ways we advance our mission to rebuild healthcare as it should be is by bringing our high-quality primary care and unmatched patient experience to more older adults across the country,” said Mike Pykosz, Oak Street Health’s CEO. “We look forward to meeting and caring for new deserving patients in Arkansas, Iowa, Kansas and Virginia, as well as the opportunity to create meaningful jobs for those passionate about improving health outcomes for patients and bridging health equity gaps in their communities.”
The CVS-Oak Street Health deal marks the latest example of vertical integration in healthcare. In addition to operating thousands of pharmacies and MinuteClinics, CVS also is the parent company of major health insurer Aetna and pharmacy benefit manager CVS Caremark.
Despite a reasonably solid third quarter, Trinity Health is still operating at a loss in its 2023 fiscal year, according to a new filing.
The health system’s fiscal year began July 1, 2022, with the latest figures covering the first nine months. Its latest operating loss shrank to $263.1 million from the prior six months’ $298 million loss. Fiscal year 2023 operating revenue currently stands at $15.9 billion, up from the same period last year.
The nonprofit health system attributed its operating revenue growth to several acquisitions (MercyOne, North Ottawa Community Health System, Genesis Health System), which collectively added $1 billion of operating revenue. Net income for the last nine months was $856.3 million, compared to $43 million in the same period the prior year.
Though inpatient volumes are stabilizing to “a new normal,” management wrote in the latest filing, most of Trinity’s revenue comes from outpatient and other non-patient revenue. Operating expenses rose $1.1 billion compared to the same period in fiscal year 2022, mostly driven by the acquisitions.
Nonoperating income was $1.2 billion during the first nine months of fiscal year 2023, up from $264.6 million in the first six months. This hike was driven partly by a $629.3 million increase in investment returns.
The health system’s operating margin was 1.6%, per the latest filing, compared to 0.1% during the same period a year ago. Margins were affected by expenses outpacing revenue, primarily driven by premium labor rates and inflation impacting supplies as well as a $137 million reduction in CARES Act grant funding.
Trinity reports $10.2 billion in unrestricted cash and investments, including 180 days cash on hand compared to 211 days in fiscal year 2022, in its latest filing.
Trinity is focused on diversifying its business by shifting to ambulatory, home health, PACE, urgent care, specialty pharmacy and telehealth. The filing also noted the recent launch of a new care delivery model dubbed TogetherTeam, involving on-site and virtual nurses, that is expected to be implemented systemwide by the end of its 2024 fiscal year.
Salaries, wages and employee benefit costs rose 2.2%, offset by a reduction of $54.6 million in executive compensation and $39.7 million more pharmacy rebates than in the same period in fiscal year 2022. Same-facility contract labor costs decreased more than 40% to $193.9 million, reflecting “unprecedented” pandemic-related costs during the third quarter in 2022.
Trinity “continues to use strong cost controls over contract labor and other operational spending as colleague investment and utilization of its FirstChoice internal staffing agency promotes labor stabilization,” management wrote.
Trinity Health spans 88 acute care hospitals and hundreds of other care locations in 26 states and purports to have the second-largest Medicare PACE (Program of All-inclusive Care for the Elderly) program in the country. It provided services to 1.3 million people and reported a community benefit and charity of $1.4 billion in fiscal year 2022.
BJC HealthCare of St. Louis and Saint Luke’s Health System of Kansas City are exploring a merger that would yield a 28-hospital, $10 billion, integrated, academic health system, the nonprofits announced Wednesday.
The two have signed a nonbinding letter of intent and “are working toward reaching a definitive agreement in the coming months” with a targeted close before the end of the year, they said. The cross-market deal would be subject to regulatory review and other customary closing conditions.
“Together with Saint Luke’s, we have an exciting opportunity to reinforce our commitment to providing extraordinary care to Missourians and our neighboring communities,” BJC HealthCare President and CEO Richard Liekweg said in the announcement. “Amid the rapidly changing health care landscape, this is the right time to build on our established relationship with Saint Luke’s. With an even stronger financial foundation, we will further invest in our teams, advance the use of technologies and data to support our providers and caregivers and improve the health of our communities.”
Both systems are based in Missouri but “serve distinct geographic markets,” they said.
St. Louis-based BJC Healthcare’s footprint is spread across the greater St. Louis, southern Illinois and southeast Missouri regions. It comprises 14 hospitals including two (Barnes-Jewish and St. Louis Children’s) affiliated with Washington University School of Medicine. It also operates multiple health service organizations providing home health, long-term care, workplace health and other offerings.
Kansas City, Missouri-based Saint Luke’s is a faith-based system with 14 hospitals and more than 100 offices throughout western Missouri and parts of Kansas. It also provides home care and hospice, adult and children’s behavioral care and a senior living community.
Should the deal close, both systems would continue to serve their existing markets and maintain their branding. The joined organization would be run from dual headquarters with BJC’s Liekweg as CEO but an initial board chair hailing from Saint Luke’s.
The organizations said their combination will expand the services available to patients and provide an estimated $1 billion in annual community benefits. The arrangement would also fuel clinical and academic research while supporting greater workforce investment.
“Our integrated health system, with complementary expertise and team of world-class physicians and caregivers, will set a new national standard for medical education and research,” Saint Luke’s President and CEO Melinda Estes, M.D., said in the announcement. “Through our decade-long relationship as a member of the BJC Collaborative, we’ve established mutual trust and respect, so the opportunity to come together as a single integrated system that can accelerate innovation to better serve patients is a logical next step.”
Years of health system consolidation have led to increased scrutiny from regulators and lawmakers, who have worried that mergers can harm competition. To date, however, efforts to block announced deals have been limited to situations where the parties are operating in the same geographic markets.
Larger, cross-market deals like BJC and Saint Luke’s have become more common in the past year, potentially due to the opportunity to distribute operational risks with limited regulatory scrutiny, analysts have noted.
Multiple health policy researchers have warned that these deals are relatively understudied and, according to some prior analyses, very rarely translate to the quality and consumer cost savings often touted by health systems.
Last week, Marlee Stark and I published an op-ed in the Arkansas Democrat Gazette on why the Arkansas Department of Human Services (DHS) should press pause on its Medicaid unwinding process. Earlier this month, DHS released its first report laying out how many people lost coverage in April, as the state resumed its redetermination process.
As we write,
According to DHS’ recent report, over 50,000 people were disenrolled for procedural reasons, like failure to return paperwork or requested information, or because the state didn’t have their correct address on file. Only 15 percent of those who were disenrolled were confirmed truly ineligible or said they no longer needed their coverage, likely because they acquired another source of coverage during the pandemic.
In our piece, we argue that DHS should take a look at why so many people are losing coverage even though they may still be eligible—and outline some of the consequences the state may face if it chooses not to do so.