Cartoon – Leadership by Words


California Attorney General Xavier Becerra has conditionally approved Verity Health’s application to transfer ownership of St. Francis Medical Center to Prime Healthcare. The Attorney General’s decision follows an earlier decision by the U.S. Bankruptcy Court of the Central District of California granting Verity’s request to reject the existing collective bargaining agreements which impose legacy cost structures that it said contributed to bankruptcy.
Becerra noted that his approval of the sale of St. Francis to Prime Healthcare “protect(s) access to care for the Los Angeles communities served” by St. Francis.
“The COVID-19 public health crisis has brought home the importance of having access to lifesaving hospital care nearby in our communities,” he said. “St. Francis Medical Center is not just an asset, it is an indispensable neighbor, it is the workers who serve the patients, and the doctors who save lives. We conditionally approve this sale to keep it that way.”
Prime Healthcare has built a reputation for saving financially distressed hospitals across the U.S., touting improved clinical quality. Healthgrades said Prime had hospitals named among the nation’s 100 best 53 times, and has been the recipient of several Patient Safety Excellence Awards.
The Attorney General’s office conducted an exhaustive review of the transaction for the past several months and carefully considered public input on the proposed transaction. The Attorney General’s approval includes conditions for the sale which Prime is currently reviewing. Pending a final ruling by the Bankruptcy Court, the transaction is expected to be completed this summer.
THE LARGER TREND
In early April, the U.S. Bankruptcy Court approved the Asset Purchase Agreement for the sale of St. Francis Medical Center to Prime. Under the agreement, Prime will acquire St. Francis for a net consideration of over $350 million, including a $200 million base cash price and $60 million for accounts receivable. In addition, Prime has committed to invest $47 million in capital improvements and extend offers of employment to nearly all staff.
The court also recently granted Verity’s request to reject the existing collective bargaining agreements with two unions that represent associates at St. Francis Medical Center, SEIU and UNAC. The court noted that Prime Healthcare was the only party to submit a qualifying bid for St. Francis and that without rejecting the existing CBAs, “St. Francis would not continue to operate as a going concern, and all of the UNAC (and SEIU) represented employees would lose their jobs.”
The court also noted that Prime and Verity had made multiple efforts to negotiate in good faith with the unions, and the parties devoted “hundreds of hours to negotiations,” but ultimately were unable to agree on new CBAs. Further, the court determined that one of the reasons for the hospital’s bankruptcy was the “legacy cost structure imposed by the existing CBAs.”
It then staid that the proposals were rejected “without good cause” by the unions. Prime said it negotiated in good faith and proposed increasingly generous offers to UNAC and SEIU with wages far above its existing agreements at its Los Angeles-area hospitals. Prime’s latest offer to SEIU maintained existing wages for roughly 90% of SEIU members, and increased wages for some of them. Prime said these wages would be substantially higher than those recently voted by SEIU members at three of Prime’s Los Angeles hospitals.
ON THE RECORD
“Receiving conditional approval is an important step in ensuring Prime is able to preserve the St. Francis mission for the benefit of associates, members of the medical staff and most importantly the patients and Southeast Los Angeles community that has relied on St. Francis for 75 years,” said Rich Adcock, CEO of Verity Health.
“We are honored to be selected to continue the St. Francis legacy and are working to review the conditions and finalize the sale as quickly as possible,” said Dr. Sunny Bhatia, CEO, Region I and chief medical officer of Prime Healthcare. “St. Francis’ mission is especially critical during this pandemic and we honor the service of all caregivers. Prime has already started investments at St. Francis that will enhance patient care as we commit to continue every service line, community benefit program, charity care and expand new services to the community.”

One component of Blockbuster’s financial model was the late fees it charged to customers who did not return a video tape to the store in time. These fees accounted for up to 16% of its revenue. In 1997, Reed Hastings was one of the customers affected by these fees. After one late rental, he was charged a hefty $40 late fee. His frustration inspired him to help create a company that would have no late charges. This new company also had the audacious idea to send DVDs straight to the customer’s home for a flat monthly fee. The company that Reed Hastings co-founded was Netflix.
Over time, Netflix changed and adapted with new technology and shifting consumer preferences. It moved on from mailing DVDs to using a streaming platform. It developed an algorithm to help make personalized video recommendations to Netflix users. It started producing its own video content. Over time, the company planted itself firmly within many homes and routines. Conversely, Blockbuster adapted to new platforms too slowly and too late. After its peak in 2004, Blockbuster started losing market share and relevance. Today, there is only one Blockbuster store left, a curious tourist attraction in Bend, Oregon.
Markets and industries change all the time. Distinguishing these important changes from temporary fads is essential. History has many examples of companies and organizations that did not sense important changes, did not change their approach, and as a result, ended up obsolete and irrelevant. A similar shift is happening today in healthcare, but there is more at stake than a late fee. Like Netflix, the healthcare industry needs to shift and adapt to consumer preferences.
The COVID-19 pandemic has had an immediate impact on the health of our country and has also indelibly changed how patients interact with the healthcare system. Hospitals and providers around the country have had to quickly develop new strategies to connect with patients – to comply with social distancing guidelines, in an effort to slow down the spread of the virus. Consistent communication and accessibility is vital, especially given the disturbing trends in decreased preventive care visits and delayed emergency care. One solution is telehealth.
During this pandemic, we have seen that remote patient monitoring is valuable for patients with a wide variety of needs: certainly, those quarantined with coronavirus, but for healthy patients too – children in need of regularly scheduled well-child visits and adults who need routine care. Many patients have experienced telehealth for the first time and many have positive impressions, with nearly three quarters of patients who had a recent telehealth visit describing it as good or very good, according to a recent survey.
Even after the COVID-19 pandemic settles, these “temporary” approaches will permanently change patient attitudes towards technology and force healthcare providers to reexamine their approach to care. Telehealth will remain a convenient option and, in some cases, a necessary way to receive care. Embedding telehealth into standard practice of care enables providers to expand the access to people who otherwise might forgo care, and to people who may face barriers getting to a clinic, for example patients with inflexible job schedules or limited transportation.
Patients and providers are not the only people recognizing the benefits; government officials are too. While reimbursement rules were temporarily expanded to include telehealth, some states, such as Colorado and Idaho, are making COVID-19 telehealth expansions permanent.
There are many parallels to borrow from the Blockbuster example. As healthcare providers, we cannot be complacent and stick with old business models because they are what we are used to. We cannot wait for people to come to us. We cannot ignore these changing times and consumers’ changing preferences. In fact, if we adapt and provide care in ways that patients prefer, we could improve health outcomes.
The healthcare institutions that will grow and be successful during this time are those who are more like Netflix. Instead of waiting for patients to decide to seek healthcare when it may be too late (e.g., just like a Blockbuster “late fee”), we will actively reach out and remind our patients about the importance of timely healthcare services. Instead of ignoring changes in patient preferences and new technology, we will adapt quickly to new platforms for healthcare visits. Instead of waiting for patients to feel comfortable to return to a healthcare facility, we will show patients what our healthcare system is doing to ensure patient safety and protection from COVID-19. Most importantly, instead of being complacent, we will accept and develop new ways of providing care.
There was once a time that we thought that getting in a car, driving to a strip mall, and walking through aisles with thousands of video tapes was the only option to watch a movie at home. Now, many of us can get thousands of titles on our televisions, computers, and phones through several movie streaming platforms. The COVID-19 pandemic has forced healthcare systems to quickly adapt to new constraints; however, it may really be an opportunity to develop new models of care, to engage with our patients, and to make healthcare more accessible. As healthcare providers, we need to make the choice to be more like Netflix, and less like Blockbuster.

Nationwide, state and local government leaders are warning of major budget cuts as a result of the pandemic. One state – New York – even referred to the magnitude of its cuts as having “no precedent in modern times.”
Declining revenue combined with unexpected expenditures and requirements to balance budgets means state and local governments need to cut spending and possibly raise taxes or dip into reserve funds to cover the hundreds of billions of dollars lost by state and local government over the next two to three years because of the pandemic.
Without more federal aid or access to other sources of money (like reserve funds or borrowing), government officials have made it clear: Budget cuts will be happening in the coming years.
And while specifics are not yet available in all cases, those cuts have already included reducing the number of state and local jobs – from firefighters to garbage collectors to librarians – and slashing spending for education, social services and roads and bridges.
In some states, agencies have been directed to cut their budget as much as 15% or 20% – a tough challenge as most states prepared budgets for a new fiscal year that began July 1.
As a scholar of public administration who researches how governments spend money, here are the ways state and local governments have reduced spending to close the budget gap.
State and local governments laid off or furloughed 1.5 million workers in April and May.
They are also reducing spending on employees. According to surveys, government workers are feeling personal financial strain as many state and local governments have cut merit raises and regular salary increases, frozen hiring, reduced salaries and cut seasonal employees.
Washington state, for example, cut both merit raises and instituted furloughs.
A survey from the National League of Cities shows 32% of cities will have to furlough or lay off employees and 41% have hiring freezes in place or planned as a result of the pandemic.
Employment reductions have met some resistance. In Nevada, for example, a state worker union filed a complaint against the governor to the state’s labor relations board for violating a collective bargaining statute by not negotiating on furloughs and salary freezes.
Most of the employee cuts have been made in education. Teachers, classroom aids, administrators, staff, maintenance crews, bus drivers and other school employees have seen salary cuts and layoffs.
The job loss has hurt public employees beyond education, too: librarians, garbage collectors, counselors, social workers, police officers, firefighters, doctors, nurses, health aides, park rangers, maintenance crews, administrative assistants and others have been affected.
Residents also face the consequences of these cuts: They can’t get ahold of staff in the city’s water and sewer departments to talk about their bill; they can’t use the internet at the library to look for jobs; their children can’t get needed services in school.
Most of these cuts have been labeled temporary, but with the extensions to stay-at-home orders and a mostly closed economy, it will be some time before these employees are back to work.

As another way to reduce costs quickly, a National League of Cities survey shows 65% of the municipalities surveyed are stopping temporarily, or completely, capital expenditure and infrastructure projects like roads, bridges, buildings, water systems or parking garages.
In New York City, there is a US$2.3 billion proposed cut to the capital budget, a fund that supports large, multiyear investments from sidewalk and road maintenance, school buildings, senior centers, fire trucks, sewers, playgrounds, to park upkeep. There are potentially serious consequences for residents. For example, New York housing advocates are concerned that these cuts will hurt plans for 21,000 affordable homes.
Suspending these big money projects will save the government money in the short term. But it will potentially harm the struggling economy, since both public and private sectors benefit from better roads, bridges, schools and water systems and the jobs these projects create.
Delaying maintenance also has consequences for the deteriorating infrastructure in the U.S. The costs of unaddressed repairs could increase future costs. It can cost more to replace a crumbling building than it does to fix one in better repair.
In many states, the new budgets severely cut their aid to local governments, which will lead to large local cuts in education – both K-12 and higher education – as well as social programs, transportation, health care and other areas.
New York state’s budget proposes that part of its fiscal year 2021 budget shortfall will be balanced by $8.2 billion in reductions in aid to localities. This is the state where the cuts were referred to in the budget as “not seen in modern times.” This money is normally spent on many important services that residents need everyday –mass transit, adult and elderly care, mental health support, substance abuse programs, school programs like special education, children’s health insurance and more. Lacking any of these support services can be devastating to a person, especially in this difficult time.

As teachers and administrators figure out how to teach both online and in person, they and their schools will need more money – not less – to meet students’ needs.
Libraries, which provide services to many communities, from free computer use to after-school programs for children, will have to cut back. They may have fewer workers, be open for fewer hours and not offer as many programs to the public.
Parks may not be maintained, broken playground equipment may stay that way, and workers may not repave paths and mow lawns. Completely separate from activists’ calls to shift police funding to other priorities, police departments’ budgets may be slashed just for lack of cash to pay the officers. Similar cuts to firefighters and ambulance workers may mean poorly equipped responders take longer to arrive on a scene and have less training to deal with the emergency.
To keep with developing public safety standards, more maintenance staff and materials will be needed to clean and sanitize schools, courtrooms, auditoriums, correctional facilities, metro stations, buses and other public spaces. Strained budgets and employees will make it harder to complete these new essential tasks throughout the day.
To avoid deeper cuts, state and local government officials are trying a host of strategies including borrowing money, using rainy day funds, increasing revenue by raising tax rates or creating new taxes or fees, ending tax exemptions and using federal aid as legally allowed.
Colorado was able to hold its budget to only a 3% reduction, relying largely on one-time emergency reserve funds. Delaware managed to maintain its budget and avoided layoffs largely through using money set aside in a reserve account.
Nobody knows how long the pandemic, or its economic effects, will last.
In the worst-case scenario, budget officials are prepared to make steeper cuts in the coming months if more assistance does not come from the federal government or the economy does not recover quickly enough to restore the flow of money that governments need to operate.

Many public health professionals and politicians are urging or requiring citizens to wear face masks to help slow the spread of the COVID-19 virus.
Some Americans have refused, wrongly claiming mask decrees violate the Constitution. An internet search turns up dozens of examples.
“Costco Karen,” for instance, staged a sit-in in a Costco entrance in Hillsboro, Oregon after she refused to wear a mask, yelling “I am an American … I have rights.”
A group called Health Freedom Idaho organized a protest against a Boise, Idaho, mask mandate. One protester said, “I’m afraid where this country is headed if we just all roll over and abide by control that goes against our constitutional rights.”
As one protester said, “The coronavirus doesn’t override the Constitution.”
Speaking as a constitutional law scholar, these objections are nonsense.

It is not always clear why anti-maskers think government orders requiring face coverings in public spaces or those put in place by private businesses violate their constitutional rights, much less what they think those rights are. But most of the mistaken objections fall into two categories:
Mandatory masks violate the First Amendment right to speech, assembly, and especially association and mandatory masks violate a person’s constitutional right to liberty and to make decisions about how to their own health and bodily integrity.
They’re not mutually exclusive claims: A lawsuit filed by four Florida residents against Palm Beach County, for example, argues that mask mandates “interfere with … personal liberty and constitutional rights,” such as freedom of speech, right to privacy, due process, and the “constitutionally protected right to enjoy and defend life and liberty.” The lawsuit asks the court to issue a permanent injunction against the county’s mask mandate.
Responding to a reporter who asked why President Donald Trump appeared unconcerned about the absence of masks and social distancing at a campaign rally in Tulsa, Vice President Mike Pence said: “I want to remind you again freedom of speech and the right to peaceably assemble is in the Constitution of the U.S. Even in a health crisis, the American people don’t forfeit our constitutional rights.”
The First Amendment protects freedom of speech, press, petition, assembly and religion.
There are two reasons why mask mandates don’t violate the First Amendment.
First, a mask doesn’t keep you from expressing yourself. At most, it limits where and how you can speak. Constitutional law scholars and judges call these “time, place, and manner” restrictions. If they do not discriminate on the basis of the content of the speech, such restrictions do not violate the First Amendment. An example of a valid time, place and manner restriction would be a law that limits political campaigning within a certain distance of a voting booth.
Additionally, the First Amendment, like all liberties ensured by the Constitution, is not absolute.
All constitutional rights are subject to the goverment’s authority to protect the health, safety and welfare of the community. This authority is called the “police power.” The Supreme Court has long held that protecting public health is sufficient reason to institute measures that might otherwise violate the First Amendment or other provisions in the Bill of Rights. In 1944, in the case of Prince v. Massachusetts, for example, the Supreme Court upheld a law that prohibited parents from using their children to distribute religious pamphlets on public streets.
Some anti-maskers object that masks violate the right to liberty.
The right to liberty, including the right to make choices about one’s health and body, is essentially a constitutional principle of individual autonomy, neatly summarized as “My body, my choice.”
The 1905 case of Jacobsen v. Massachusetts shows why mask mandates don’t violate any constitutional right to privacy or health or bodily integrity. In that case, the Supreme Court upheld a smallpox vaccination requirement in Cambridge, Massachusetts.
The court said that the vaccination requirement did not violate Jacobsen’s right to liberty or “the inherent right of every freeman to care for his own body and health in such way as to him seems best.”
As the court wrote, “There are manifold restraints to which every person is necessarily subject for the common good. On any other basis, organized society could not exist with safety to its members.” In a 1995 New York case, a state court held that an individual with active tuberculosis could be forcibly detained in a hospital for appropriate medical treatment.
Even if you assume that mask mandates infringe upon what the Supreme Court calls “fundamental rights,” or rights that the court has called the “very essence of a scheme of ordered liberty,” it has consistently ruled states can act if the restrictions advance a compelling state interest and do so in the least restrictive manner.
As the Jacobsen ruling and the doctrine of time, place and manner make clear, the protection of all constitutional liberties rides upon certain necessary – but rarely examined – assumptions about communal and public life.
One is that is constitutional rights – whether to liberty, speech, assembly, freedom of movement or autonomy – are held on several conditions. The most basic and important of these conditions is that our exercise of rights must not endanger others (and in so doing violate their rights) or the public welfare. This is simply another version of the police power doctrine.
Unfortunately, a global pandemic in which a serious and deadly communicable disease can be transmitted by asymptomatic carriers upsets that background and justifies a wide range of reasonable restrictions on our liberties. Believing otherwise makes the Constitution a suicide pact – and not just metaphorically.

Turn on the TV news, or look at a news website, and you’ll see charts, graphics, and dashboards that supposedly indicate the latest with COVID-19 – statistics revealing the number of tests, cases, hospitalizations and deaths, along with where they happened and whether they are rising or falling.
Different stories are told depending on the dashboard. But one thing is certain: These indicators lag behind the actions we take, or don’t take, on COVID-19. As researchers who focus on public health, we can tell you that a fully accurate, real-time snapshot of the progress of the virus isn’t possible.
There are many reasons for this. Here’s one: diagnostic testing data are incomplete. Someone infected with COVID-19 must first come in contact with the virus either through the air or (less likely) environmental surfaces. Symptoms show between two and 14 days later. But at least 40% of those infected will never manifest symptoms, or show such mild ones they don’t even suspect they have COVID-19. So they may never get tested, which means they won’t show up in the total number of tests, or the total number of cases.
Another example: because of the lack of testing availability – a widespread problem in the U.S. since the start of the pandemic – not everyone who should be tested gets a test.
And another: the tests themselves are not perfect. Up to one-third who get a negative result may actually be infected. This happens because they are tested before they have a viral load sufficient enough for detection. Or maybe the sampling is not adequate. Or perhaps the test itself simply failed.

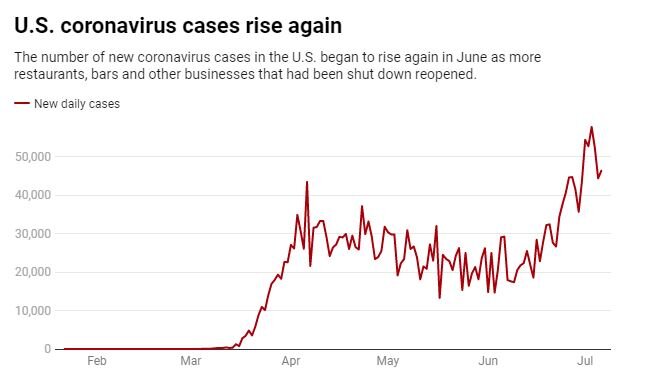
This is why problems arise when we use case numbers to determine disease levels in a community. Case counts actually reflect what was happening in a community weeks earlier. Four weeks, for instance, could elapse between the time a person is exposed to the virus and when they are reported as a case. Even the best testing results often take a week to report to public health authorities, and longer to appear on dashboards. Some testing results, seriously delayed, may take ten days or more.
Other factors impact the metrics. Laboratory results, often released in batches, may introduce artificial variation in case numbers. Someone who tested two days ago, then got a result back immediately, might be added on the same day as someone who was sick two weeks ago, but whose test results were delayed. To smooth out these variations, it helps to look at a rolling seven-day case average.
Hospitalization is a clearer metric for assessing the level of community disease. Those who are seriously ill, in most cases, will be hospitalized whether previously tested or not. Data suggests roughly one in five infected persons are hospitalized. Individuals seem to do okay for the first week, with more life-threatening symptoms showing in the second. That means hospitalizations represent exposures that happened three or four weeks earlier.
Again, a seven-day rolling average evens out artificial variations. There is one caveat for this: Though hospitalization is a useful metric, only about 20% of infected people need it. That means hospitalization numbers alone underestimate the number of people infected and what age groups they represent.
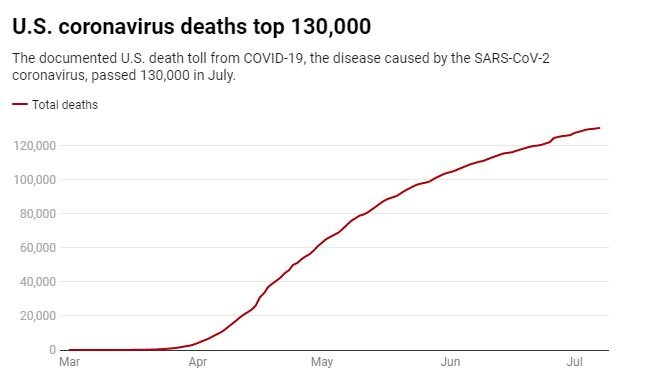
The death numbers are not a reliable indicator either. In some states, to count as a COVID-19 death, the deceased must have had a test reporting positive. In other states, probable cases are reported.
As clinicians learn how to better treat COVID-19, fatality rates are dropping. Deaths, the longest lagging indicator, reflect people who were infected six or eight weeks earlier. When comparing one region to another, deaths are best expressed as rates – a ratio of deaths to population.
Another issue: News reports do not always clearly distinguish between diagnostic testing, which shows if you currently have COVID-19, and antibody testing, which shows if you had it in the past, and now harbor antibodies that can fight it. So far, however, antibody testing has not provided a useful picture of who has been infected and who has not. Once that happens, it could provide researchers and clinicians with some indicators on how widely the virus has spread.
Though the dashboards are ubiquitous on television, none of these frequently used indicators they feature is perfect. Still, taken together, they provide a reasonable approximation of COVID-19 transmission in communities. But as authorities make decisions, they should take into account the numbers are weeks old.
What does this mean to you? Understanding these limitations may help you understand your risk. We are still in the midst of a pandemic that is not under control. Being educated will help all of us from becoming a part of tomorrow’s lagging indicators.

In many respects this recession is unique. Most recessions result from developments inside the economy, but an external shock—the public health crisis—caused this one. To avoid getting sick, people have curtailed working, shopping, and attending school. Whatever the cause, the coronavirus recession, like all recessions, is imposing heavy costs. Many workers have lost jobs and income, and many business owners’ financial survival is at risk. The economy’s extraordinarily rapid decline earlier this year—as well as the sharp but incomplete rebound following the first steps toward reopening—reflect this recession’s unusual source. In addition, the sectors suffering most differ from past recessions. The heaviest blows have fallen on service industries that involve close personal contact (including retail trade, leisure and hospitality, and transportation) rather than, as is more typical, on the housing, capital investment, and durable goods sectors. Lower-paid workers, as well as women and minorities, are over-represented in the most-affected sectors, and thus have borne a disproportionate share of the job and income losses. And, the virus has affected almost every country, with potentially devastating consequences for trade and international investment.
Because this recession is unprecedented in so many ways, forecasting the recovery is difficult. The course of the pandemic itself is by far the most important factor. As long as people fear catching a potentially deadly illness from other people, they will be cautious about resuming normal activities, even after state and local governments lift lockdowns. Thus, controlling the spread of the virus must be the first priority for restoring more-normal levels of economic activity—but, more importantly, for saving possibly tens of thousands of lives. Members of Congress, local leaders, and other policymakers need to do all they can to support testing and contact tracing, medical research, and sufficient hospital capacity, and they must work to ensure that businesses, schools, and public transportation have what they need to operate safely. Both authors of this testimony are serving on state re-opening commissions, which has provided us insight into the substantial challenges to safe re-opening.
If the pandemic comes under better control, economic recovery should follow. However, the pace of the recovery could be slow and uneven, for several reasons. First, in the face of ongoing uncertainty, households and businesses may remain cautious for a time. They may increase saving and reduce spending, hiring, and capital investment. The longer the recession lasts, the greater the damage it will inflict on household and business balance sheets and the longer it will take to repair the damage. Second, the depth of the recession may leave scars—business closures and the deterioration of unemployed workers’ skills—that will affect growth for several years. Third, depending on the course of the virus, some restructuring of the economy may be needed. For example, people and resources will need to be redeployed out of the sectors most damaged by the pandemic, and business operations will need to be reorganized to protect workers and customers. All of that will take time and money. Fiscal and monetary policies must aim to speed the recovery and minimize the recession’s lasting effects.
The Federal Reserve has moved swiftly and forcefully in this crisis. It eased monetary policy in March by lowering the federal funds rate, the overnight interest rate on loans between banks, nearly to zero and indicating that it plans to keep rates low for several years. Low interest rates probably had limited economic benefits in the spring. Lockdowns prevented people from spending or working more. However, we expect low rates will spur spending in sectors like housing as the economy reopens. And the Fed may well do more in coming months as re-opening proceeds and as the outlook for inflation, jobs, and growth becomes somewhat clearer. In particular, to maintain downward pressure on longer-term interest rates, the Federal Open Market Committee (FOMC) likely will provide forward guidance about the economic conditions it would need to see before it considers raising its overnight target rate. And it likely will clarify its plans for further securities purchases (quantitative easing). It is possible, though not certain, that the FOMC will also implement yield-curve control by targeting medium-term interest rates. It could, for example, target two-year rates by announcing its willingness to buy two-year Treasury notes at a fixed yield. The completion of the Fed’s internal review of its tools and framework in coming months will help guide these decisions.
The Fed also has been active beyond monetary policy.
First, the Fed has served as market maker of last resort by acting to stabilize critical financial markets when capital or other regulatory constraints have interfered with normal market-making or arbitrage. The Fed has served this role for repurchase agreements (repos) since September, when intermittent liquidity shortages led to spikes in repo rates. Banks did not provide liquidity to offset these spikes, as they normally would, citing balance sheet limits and other constraints. Because repo markets are critical to the functioning of broader financial and credit markets, as well as for the transmission of monetary policy, the Fed has restored more-normal function in repo markets by conducting large-scale repo operations and by steadily increasing the quantity of reserves in the banking system.
An even larger shock occurred in March, when uncertainty about the pandemic led hedge funds and others to scramble to raise cash by selling longer-term securities. The upsurge in the supply of longer-term securities, including Treasuries, was more than dealers and other market-makers could handle. Key financial markets, including for Treasury securities, experienced substantial volatility. To stabilize these markets, which like the repo market play a critical role in our financial system, the Fed purchased large quantities of Treasuries and mortgage-backed securities, again serving as market maker of last resort. It also set up a new repo facility to allow foreign official institutions to borrow dollars, using their Treasury reserves as collateral, thus avoiding the need to sell those Treasuries. Although risk and liquidity premiums in these key markets have returned closer to normal, at some point the Fed and the Treasury will need to review why the market-making facilities in place before the pandemic hit did not work more efficiently.
Second, the Fed has served as lender of last resort to the financial system, a classic function of central banks. Banks and other financial intermediaries typically borrow short and lend long—that is, they rely heavily on short-term funding to finance long-term loans and investments. If they lose their short-term funding—because their funders lose confidence or for other reasons—they can be forced to sell their assets in fire sales, restrict credit to customers, and, in extreme cases, become insolvent. Central banks can short-circuit that dangerous dynamic by lending to financial institutions against good collateral, replacing the lost liquidity. In the 2007-2009 crisis, which centered on the financial system and included a global financial panic, the Fed as lender of last resort took many actions to provide liquidity to financial institutions, with the goal of stabilizing the system and preserving the flow of credit to the economy.
Fortunately, the financial system is in much better shape today than in was during the financial crisis. Banks in particular are strong, with much higher levels of capital and liquidity. The Fed nevertheless has once again taken steps to ensure that the financial system has sufficient liquidity. Largely replicating our playbook from the crisis era, the Fed has eased terms on the discount window (which provides short-term loans to banks); re-established the Primary Dealer Credit Facility (which lends to broker-dealers); and established a facility that lends indirectly to money market mutual funds, ensuring that the funds can meet depositor withdrawals. In a novel step, the Fed also created a facility that lends to banks, without recourse, against Payroll Protection Program loans, ensuring that banks have sufficient funds to make those loans.
Under the heading of lender of last resort to the financial system, establishing currency swap lines with fourteen foreign central banks was one of the most important actions the Fed took in the 2007-2009 crisis. The Fed has revived this program. Currency swap lines allow foreign central banks (who assume all the credit risk) to lend dollars to banks in their jurisdictions. The broad availability of dollar liquidity is essential because most global banks do substantial borrowing and lending in dollars, including lending within the United States. The swap lines sustain the flow of dollar credit and reduce volatility in dollar-based markets, to the benefit of the U.S. economy.
Third, the Federal Reserve, with the support of the Congress and the Treasury, has also served during the current crisis as a lender of last resort to the non-financial sector, backstopping key credit markets facing the prospect of severe disruption from the pandemic. To take on this role, the Fed invoked its emergency lending powers under Section 13(3) of the Federal Reserve Act. Since those powers require that the Fed’s lending be well secured, it has had to rely on funds appropriated by the Congress and allocated by the Treasury to cover possible losses. Using these authorities, the Fed revived financial crisis-era facilities to stabilize commercial paper and asset-backed securities markets. Going beyond the financial crisis playbook, the Fed has also added new facilities to lend to corporations and state and local governments and to buy outstanding corporate bonds.
These programs have not extended much credit, so far, but that does not mean they have not succeeded. By establishing the programs, the Fed gave private investors the confidence to re-engage by reassuring them that the government would not allow these critical markets to become dysfunctional. Indeed, the corporate and municipal bond markets largely stabilized after the announcements, before any loans were made. Of course, if these markets seize up again, the Fed’s programs can extend credit.
The Fed also established the Main Street Lending Program to lend (through banks) to medium-sized companies. It is too soon, however, to judge its performance. This program is very different from anything the Fed has attempted before and poses difficult technical challenges. Although the Fed took many public comments while setting up the program, and made substantial changes, questions remain about how many banks and borrowers will participate. The Fed and Treasury may have to further ease terms for borrowers and increase incentives for banks for this program to have the desired effect. Or, the Fed and Treasury could add a new facility, along the lines of funding-for-lending programs run by the Bank of England and the European Central Bank, that simply subsidize banks for making additional loans to qualifying borrowers (for example, businesses below a certain size). That approach leaves the underwriting decision completely with the banks, while the size of the subsidy can be adjusted as needed to achieve the desired level of lending.
Finally, the Fed has also taken actions as a bank regulator—for example, encouraging banks to work with borrowers hobbled by the pandemic. It decided recently, based on stress test results, to bar stock buybacks by banks and to limit—but not eliminate—their dividends. Based on our experience in the global financial crisis, we think the Fed may find it needs to go further. Although banks are currently strong, it is possible the pandemic will so damage the economy that credit losses mount rapidly. For a successful recovery, the banking system must remain strong and able to lend.
Is there more the Fed could do? As we noted, the Fed likely will provide more clarity about its monetary policy plans, and it may need to adjust the terms or borrower eligibility requirements of its various lending facilities. Broadly speaking, though, the Fed’s response has been forceful, forward-looking, and comprehensive. But, as Chair Powell often notes, the Fed’s authorities allow it to lend, not spend. Some households and firms will need subsidies or grants, rather than loans, and spending is, of course, the province of the Congress.
The fiscal response to the pandemic has thus far been quite effective. Enhanced unemployment insurance and the Paycheck Protection Program have helped unemployed workers and their families, together with many businesses, survive the spring shutdowns. The fiscal support for the Fed’s lending programs likely will help preserve credit availability, possibly with only a portion of the allocated funds being spent.
However, some programs authorized by the Congress are ending, and new actions are necessary. Our recommendations for further fiscal action are:
First, Congress should develop a comprehensive plan to support medical research; increase testing, contact tracing and hospital capacity; make available critical supplies; and support state and local efforts to safely open businesses, schools, and public transportation.
Nothing is more important for restoring economic growth than improving public health. Investments in this area are likely to pay off many times over.

Many U.S. hospitals and health systems have furloughed staff to help offset revenue losses from the COVID-19 pandemic. Now, some are starting to bring furloughed workers back as they resume nonemergency procedures and medical appointments.
Here are 14 reported in July and June:
Editor’s Note: This webpage will be updated routinely.
July
1. Elmeria, N.Y.-based Arnot Health said it brought back about half of the about 400 people it furloughed in mid-April, according to WETM-TV .
2. Guthrie said most furloughed staff have returned to the Sayre, Pa.-based health system, according to WETM-TV .
3. Charlottesville-based University of Virginia Health System will end some of its pandemic-related furloughs and pay cuts by the end of July and others in August.
4. Holyoke (Mass.) Medical Center brought back nearly 170 of 250 furloughed employees at the start of July, and another 80 to 90 are expected to return at month’s end, President and CEO Spiros Hatiras told BusinessWest.
5. Sarasota (Fla.) Memorial Health Care System brought back 640 furloughed workers.
June
6. MUSC Health, an eight-hospital system based in Charleston, S.C., called back nearly half of the employees who had been furloughed.
7. Lewiston-based Central Maine Healthcare has recalled about three-quarters of its 300 employees furloughed in April, spokesperson Kate Carlisle told the Sun Journal. The remaining furloughed employees are expected to return by mid-July.
8. Lewiston, Maine-based St. Mary’s Health System has recalled 80 percent to 85 percent of its 77 employees furloughed in April, spokesperson Steve Costello told the Sun Journal. Others are expected to return in July.
9. About 3,000 furloughed workers at hospitals in the Dayton, Ohio, region have been called back to work, according to the Springfield News-Sun. As of June 24, 2,606 workers remained on furlough, Sarah Hackenbracht, CEO of the Greater Dayton Area Hospital Association, told the newspaper. Initially, 5,648 hospital employees were furloughed in the 11-county region during the pandemic.
10. As of June 1, Claxton-Hepburn Medical Center in Ogdensburg, N.Y., brought back 34 employees, including nurses and staff for surgery, according to WWNY-TV. This is out of about 175 employees who were furloughed in April.
11. St. Lawrence Health System, a three-hospital system in Potsdam, N.Y., had called 80 furloughed employees back to work as of June 1, according to WWNY-TV. The health system furloughed about 400 workers.
12. St. Joseph’s Health in Syracuse, N.Y., had brought back 135 workers as of June 1, according to Syracuse.com. The organization, a member of Livonia, Mich.-based Trinity Health, furloughed 500 employees in April.
13. Crouse Health in Syracuse, N.Y., an affiliate of New Hyde Park, N.Y.-based Northwell Health, had brought back 63 of its 278 furloughed workers as of June 1, according to Syracuse.com.
14. Lewis County Health System CEO Gerald Cayer said June 12 that the Lowville, N.Y.-based organization soon will end the eight-week furlough that put 14 percent of its workforce on unpaid leave, according to nny360.com. Ten furloughed employees had returned to work as of June 12, and Mr. Cayer said other employees would return to work beginning June 21.