
Cartoon – Revenue Enhancement

A lawsuit filed last week accuses RWJBarnabas Health of “a years-long systemic effort” to hamper competition and monopolize acute care hospital services in northern New Jersey.
The case brought by CarePoint Health to a U.S. District Court accuses the state’s largest integrated healthcare delivery system of “aiming to destroy the three hospitals operated by CarePoint as independent competitors” with the support of healthcare real estate investors and Horizon Blue Cross Blue Shield, the state’s largest health insurer.
CarePoint Health includes the 349-bed Christ Hospital, 224-bed Bayonne Medical and 348-bed Hoboken University Medical Center (HUMC).
The group said RWJBarnabas intended to force the first two hospitals to shut down but acquire the third due to its more profitable payer mix.
“RWJBarnabas Health’s] goal explicitly disregarded the needs of the poor, underinsured and charity care patients which CarePoint serves in its role as the safety net hospital system in Jersey City and surrounding areas,” CarePoint wrote in the lawsuit.
The slew of alleged tactics listed in the lawsuit largely surround RWJBarnabas Health’s “serial acquisitions” of hospitals, providers and real estate that “has gone unchecked by the state and [New Jersey Department of Health],” CarePoint wrote.
This included an alleged bad faith proposal to acquire Christ Hospital and HUMC, the true intent of which CarePoint said was to “gain market knowledge and gather competitive intelligence, and use this newly-acquired information to freeze programmatic growth and any significant hiring or construction at Christ Hospital.” The process had a negative impact on CarePoint’s employee retention and staffing, according to the suit.
The plaintiff also alleged that RWJBarnabas used its political connections to influence whether state departments granted CarePoint Certificates of Need for multiple revenue-generating projects as well as COVID-19 relief funding.
Further, CarePoint accused RWJBarnabas of strategically adjusting its service offerings in competitive markets to drive uninsured or underinsured patients to CarePoint facilities while using its relationships with Horizon and ambulance operators to drive emergency room traffic and well-insured patients, respectively, to competing locations.
These collective actions constitute violations of the Sherman Antitrust Act as well as the New Jersey Antitrust Act, CarePoint wrote.
“The idea that [RWJBarnabas Health] would use its influence to jeopardize the health of that community and the care providers of a competing hospital not only directly contradicts its own vision, but clearly demonstrates that [RWJBarnabas Health] is far more interested in anti-competitive and predatory business activities than serving the New Jersey community,” CarePoint wrote.
RWJBarnabas Health discounted the allegations in an email statement.
“This is yet another in a series of baseless complaints filed by CarePoint, an organization whose leadership apparently prefers to assign blame to others rather than accept responsibility for the unsatisfactory results of their own poor business decisions and actions over the years,” a spokesperson for the system told Fierce Healthcare. “RWJBarnabas Health has a longstanding commitment to serve the residents of Hudson County, and is proud of the significant investments we have made in technology, facilities and clinical teams as we advance our mission.”
RWJBarnabas Health treats over 3 million patients per year and employs 37,000 people. The academic healthcare system runs 12 acute care hospitals and four specialty hospitals alongside other locations and services. It disclosed more than $6.6 billion in total operating revenues across 2021.
The system’s merger and acquisition activity placed it in the federal spotlight this past year after the Federal Trade Commission moved to block its planned integration of New Brunswick-based Saint Peter’s Healthcare System. The deal was called off in June.
https://www.washingtonpost.com/business/2022/09/12/minnesota-nurses-strike/

About 15,000 nurses in Minnesota walked off the job Monday to protest understaffing and overwork — marking the largest strike of private-sector nurses in U.S. history.
Slated to last three days, the strike spotlights nationwide nursing shortages exacerbated by the coronavirus pandemic that often result in patients not receiving adequate care. Tensions remain high between nurses and health-care administrators across the country, and there are signs that work stoppages could spread to other states.
Minnesota nurses charge that some units go without a lead nurse on duty and that nurses fresh out of school are delegated assignments typically held by more experienced nurses, across some 16 hospitals where strikes are expected.
The nurses are demanding a role in staffing plans, changes to shift scheduling practices and higher wages.
“I can’t give my patients the care they deserve,” said Chris Rubesch, the vice president of the Minnesota Nurses Association and a nurse at Essentia Health in Duluth. “Call lights go unanswered. Patients should only be waiting for a few seconds or minutes if they’ve soiled themselves or their oxygen came unplugged or they need to go to the bathroom, but that can take 10 minutes or more. Those are things that can’t wait.”
Paul Omodt, a spokesman for the Twin Cities Hospital Group, which represents four hospital systems where nurses are striking in the Minneapolis-St. Paul area, said that the nurses union did not do everything it could to avoid a strike.
“Nurses have steadfastly refused to go to mediation,” Omodt said. “Their choice is to strike. This strike is on the nurses.”
Conny Bergerson, a spokeswoman for Allina Health, another hospital system in the Twin Cities where nurses are on strike, said “rushing to a strike before exhausting all options such as engaging a neutral federal mediator does not benefit our employees, patients or the communities we serve.”
The Minnesota Nurses Association, the nurses union, said hospital administrators have continued to “refuse solutions” on understaffing and safety in contract negotiations. It said nurses have increasingly been asked to take on more patients for bedside care to make up for labor shortages, exacerbating burnout and high turnover.
Some hospitals have offered increased safety protocols for reporting security incidents in negotiations, but have not budged on other safety- and staffing-related demands.
The union has proposed new mechanisms for nurses to have a stronger say in how wards are staffed, including a committee made up of nurses and management at each hospital that would determine appropriate staffing levels. It has also proposed protections against retaliation for nurses who report understaffing. Striking nurses at some hospitals said their shifts are often short five to 10 nurses, forcing nurses to take on more patients than they can handle.
Omodt said that while there was a rise in understaffing reports during the height of covid, conditions have improved, and nurses have made contradictory claims when it comes to staffing at their hospitals since then.
In the lead-up to the strike, Minnesota hospital groups filed unfair labor practices charges against the union for refusing to go to mediation, and asked the National Labor Relations Board to block the strike for a failure to provide enough notice. The NLRB has thrown out at least some of those charges.
Hospitals facing strikes have been recruiting traveling nurses from across the region and plan to maintain staffing levels during the strike, though they are preparing for reduced operations, according to some of the hospital groups facing strike activity.
For years, hospitals in the United States have faced understaffing problems. A surge in demand and increased safety risks for nurses during the pandemic accelerated those trends. The number of health-care workers in the United States has still not recovered to its pre-pandemic levels, down 37,000 workers compared with February 2020.
At the same time, demand for health-care services has steadily increased during the pandemic, with a backlog of people who delayed care now seeking medical attention. During the covid wave that swept across the United States this summer, states such as New York and Florida reported the worst nursing shortages in decades. Research shows that patients are more likely to die because of preventable reasons when health-care providers are overworked.
Nurses, who risked their lives during the pandemic, are quitting and retiring early in droves, because of increased workloads caused by short staffing and demanding schedules that make finding child care and having a life outside of work exceedingly difficult. The understaffing crisis is pronounced in Minnesota in part because of its aging population and its record low unemployment rate.
There are some signs that nurse- and other health-care-worker strikes could spill over to other states in the coming weeks. Four thousand nurses with the Michigan Nurses Association voted earlier this month to authorize a strike related to understaffing concerns, and 7,000 health-care workers in Oregon have also authorized a work stoppage. University of Wisconsin nurses narrowly averted a strike this week. Therapists and clinicians in Hawaii and California are currently in the fourth week of what has become the longest-running mental health care strike, over inadequate staffing levels.
In Minnesota, the Minnesota Nurses Association recorded a 300 percent increase in nurses’ reports of unsafe staffing levels on their shifts since 2014, up to 7,857 reports in 2021.
Kelley Anaas, 37, a nurse who works in the ICU at Abbott Northwestern in Minneapolis said nurses in her unit have been forced to double up on patient assignments and work with lead nurses who have less than a year of experience.
“It eats away at you. If that was my family member in that bed, I wouldn’t want to leave their side,” said Anaas, adding that her workload has increased steadily over her 14 years at Abbott Northwestern.
While the nurses say their main impetus for striking is staffing levels and not pay, they are also at odds with hospitals over wages. The Minnesota Nurses Association has proposed a 30 percent pay increase over the next three years, noting inflation is at a 40-year high, while health-care groups have proposed a pay increase of 10 to 12 percent.
“The union’s wage demands remain at 29 and 30 percent increases over three years, which we’ve told them is unrealistic and unaffordable,” Omodt said, noting that the average Minnesota nurse makes $80,960 a year.
Contracts expired in May and June, and the union has been in negotiations since March.
Nurses said they are frustrated the strike is happening, but the stakes are high for them and their patients.
“We’re really sad and disappointed that it has come to a strike,” said Brianna Hnath, a nurse at North Memorial in Robbinsdale. “But we feel like this is the only thing we can do to show administration how incredibly important a strong nursing core is to a hospital. Hospitals tell us it’s our fault, but we’ve been actively involved and getting nowhere.”
https://mailchi.mp/6a3812741768/the-weekly-gist-september-9-2022?e=d1e747d2d8
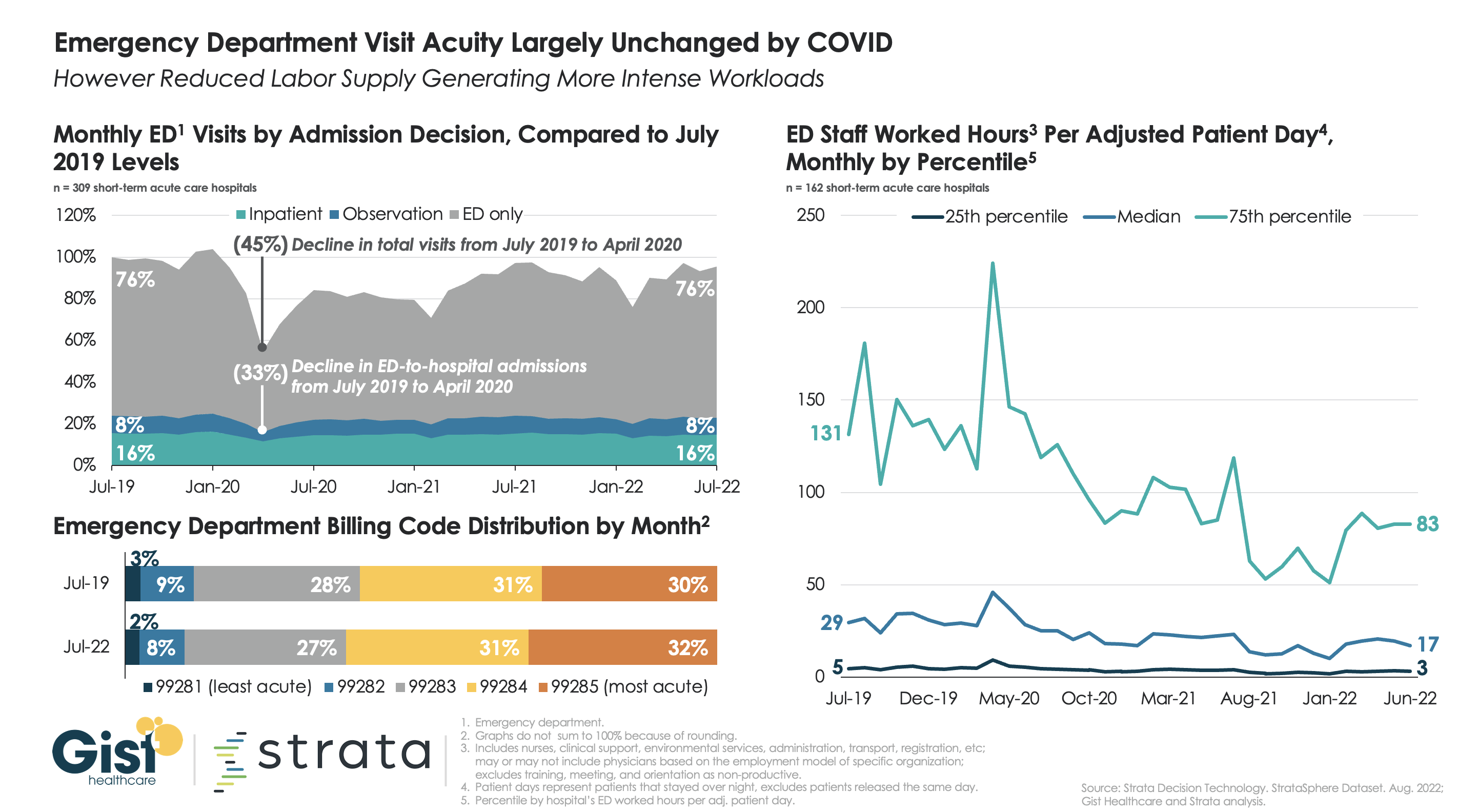
Many health systems are wondering if consumers are now leveraging new access points, including telemedicine, for low-acuity urgent care instead of going to the emergency department (ED), something which many experts are forecasting. For the graphic above, we partnered with healthcare software and analytics firm Strata Decision Technology to try to answer this question.
Using their national StrataSphere dataset for short-term acute care hospitals, we found that ED patient acuity levels in July 2022 were virtually identical to those in July 2019, though 2022 volumes were down by four percent. Admission and observation decisions across the two groups were also largely the same. We’ll be keeping our eye on the data to see if the story changes, as individuals who have delayed care over the last two and a half years now return, presenting to the ED with more advanced disease.
While current ED patients may not be more acute than before, the ongoing shortage of clinical labor may explain why some hospitals tell us that their EDs feel busier than ever. Measured by total worked hours of ED employees per adjusted patient day, the amount of labor dedicated to each patient requiring an overnight ED stay is down around forty percent from 2019 across hospital EDs of all staffing levels. With fewer labor hours to go around, each team member on the floor now has more to do.

Here are 14 health systems with strong operational metrics and solid financial positions, according to reports from Fitch Ratings and Moody’s Investors Service.
1. Advocate Aurora Health has an “AA” rating and stable outlook with Fitch. The health system, dually headquartered in Milwaukee and Downers Grove, Ill., has a strong financial profile and a leading market position over a broad service area in Illinois and Wisconsin, Fitch said. The health system’s fundamental operating platform is strong, the credit rating agency said.
2. AnMed Health has an “AA-” rating and stable outlook with Fitch. The Anderson, S.C.-based system has a leading market share in most service lines, strong operating performance and very solid EBITDA margins, Fitch said.
3. Banner Health has an “AA-” rating and stable outlook with Fitch. The Phoenix-based health system’s core hospital delivery system and growth of its insurance division combine to make it a successful highly integrated delivery system, Fitch said. The credit rating agency said it expects Banner to maintain operating EBITDA margins of about 8 percent on an annual basis, reflecting the growing revenues from the system’s insurance division and large employed physician base.
4. Bon Secours Mercy Health has an “AA-” rating and stable outlook with Fitch. The Cincinnati-based health system has a broad geographic footprint as one of the five largest Catholic health systems in the U.S., a good payer mix and a leading or near leading market share in eight of its eleven markets in the U.S., Fitch said.
5. Lincoln, Neb.-based Bryan Health has an “AA-” rating and stable outlook with Fitch. The health system has a leading and growing market position, very strong cash flow and a strong financial position, Fitch said. The credit rating agency said Bryan Health has been resilient through the COVID-19 pandemic and is well-positioned to accommodate additional strategic investments.
6. Franciscan Alliance has an “AA” rating and stable outlook with Fitch. The Mishawaka, Ind.-based health system has a very strong cash position and maintains leading market shares in seven of its nine defined primary service areas, Fitch said. The health system benefits from a good payer mix, the credit rating agency said.
7. Gundersen Health System has an “AA-” rating and stable outlook with Fitch. The La Crosse, Wis.-based health system has strong balance sheet metrics and a leading market position and expanding operating platform in its service area, Fitch said. The credit rating agency expects the health system to return to strong operating performance as it emerges from disruption related to the COVID-19 pandemic.
8. Hackensack Meridian Health has an “AA-” rating and stable outlook with Fitch. The Edison, N.J.-based health system has shown consistent year-over-year increases in market share and has a solid liquidity position, Fitch said.
9. Falls Church, Va.-based Inova Health System has an “Aa2” rating and stable outlook with Moody’s. The health system has a consistently strong operating cash flow margin and ample balance sheet resources, Moody’s said. Inova’s financial excellence will remain undergirded by its favorable regulatory and economic environment, the credit rating agency said.
10. Salt Lake City-based Intermountain Healthcare has an “Aa1” rating and stable outlook with Moody’s. The health system has exceptional credit quality, which will continue to benefit from its leading market position in Utah, Moody’s said. The credit rating agency said the health system’s merger with Broomfield, Colo.-based SCL Health will give Intermountain greater geographic reach.
11. Omaha-based Nebraska Medicine has an “AA-” rating and stable outlook with Fitch. The health system has a strong market position and is the only public academic provider in Nebraska with high acuity services, Fitch said. The health system continues to generate positive operating cash flow levels, and it has modest flexibility to absorb additional debt, according to the credit rating agency.
12. Fort Wayne, Ind.-based Parkview Health has an “Aa3” rating and stable outlook with Moody’s. The health system has a leading market position with expansive tertiary and quaternary clinical services in northeastern Indiana and northwestern Ohio, Moody’s said. The credit rating agency said the stable outlook reflects management’s ability to generate strong operating performance during the pandement and with less favorable reimbursement rates.
13. UnityPoint Health has an “AA-” rating and stable outlook with Fitch. The Des Moines, Iowa-based health system has strong leverage metrics and cash position, Fitch said. The credit rating agency expects the health system’s balance sheet and debt service coverage metrics to remain robust.
14. Yale New Haven (Conn.) Health has an “AA-” rating and stable outlook with Fitch. The health system’s turnaround efforts, brand recognition and market presence will help it return to strong operating results, Fitch said.
Working as a travel nurse in the early days of the Covid pandemic was emotionally exhausting for Reese Brown — she was forced to leave her young daughter with her family as she moved from one gig to the next, and she watched too many of her intensive care patients die.
“It was a lot of loneliness,” Brown, 30, said. “I’m a single mom, I just wanted to have my daughter, her hugs, and see her face and not just through FaceTime.”
But the money was too good to say no. In July 2020, she had started earning $5,000 or more a week, almost triple her pre-pandemic pay. That was the year the money was so enticing that thousands of hospital staffers quit their jobs and hit the road as travel nurses as the pandemic raged.
Two years later, the gold rush is over. Brown is home in Louisiana with her daughter and turning down work. The highest paid travel gigs she’s offered are $2,200 weekly, a rate that would have thrilled her pre-pandemic. But after two “traumatic” years of tending to Covid patients, she said, it doesn’t feel worth it.
“I think it’s disgusting because we went from being praised to literally, two years later, our rates dropped,” she said. “People are still sick, and people are still dying.”
The drop in pay doesn’t mean, however, that travel nurses are going to head back to staff jobs. The short-lived travel nurse boom was a temporary fix for a long-term decline in the profession that predates the pandemic. According to a report from McKinsey & Co., the United States may see a shortage of up to 450,000 registered nurses within three years barring aggressive action by health care providers and the government to recruit new people. Nurses are quitting, and hospitals are struggling to field enough staff to cover shifts.
Nine nurses around the country, including Brown, told NBC News they are considering alternate career paths, studying for advanced degrees or exiting the profession altogether.
“We’re burned out, tired nurses working for $2,200 a week,” Brown said. People are leaving the field, she said, “because there’s no point in staying in nursing if we’re expendable.”
Travel nursing seems to have started as a profession, industry experts say, in the late 1970s in New Orleans, where hospitals needed to add temporary staff to care for sick tourists during Mardi Gras. In the 1980s and the 1990s, travel nurses were often covering for staff nurses who were on maternity leave, meaning that 13-week contracts become common.
By 2000, over a hundred agencies provided travel contracts, a number that quadrupled by the end of the decade. It had become a lucrative business for the agencies, given the generous commissions that hospitals pay them. A fee of 40 percent on top of the nurse’s contracted salary is not unheard of, according to a spokesperson for the American Health Care Association, which represents long-term care providers.
Just before the pandemic, in January 2020, there were about 50,000 travel nurses in the U.S., or about 1.5 percent of the nation’s registered nurses, according to Timothy Landhuis, vice president of research at Staffing Industry Analysts, an industry research firm. That pool doubled in size to at least 100,000 as Covid spread, and he says the actual number at the peak of the pandemic may have far exceeded that estimate.
By 2021, travel nurses were earning an average of $124.96 an hour, according to the research firm — three times the hourly rate of staff nurses, according to federal statistics.
That year, according to the 2022 National Health Care Retention & RN Staffing Report from Nursing Solutions Inc., a nurse recruiting firm, the travel pay available to registered nurses contributed to 2.47% of them leaving hospital staff jobs.
But then, as the rate of deaths and hospitalizations from Covid waned, the demand for travel nurses fell hard, according to industry statistics, as did the pay.
Demand dropped 42 percent from January to July this year, according to Aya Healthcare, one of the largest staffing firms in the country.
That doesn’t mean the travel nurses are going back to staff jobs.
Brown said she’s now thinking about leaving the nursing field altogether and has started her own business. Natalie Smith of Michigan, who became a travel nurse during the pandemic, says she intends to pursue an advanced degree in nursing but possibly outside of bedside nursing.
Pamela Esmond of northern Illinois, who also became a travel nurse during the pandemic, said she’ll keep working as a travel nurse, but only because she needs the money to retire by 65. She’s now 59.
“The reality is they don’t pay staff nurses enough, and if they would pay staff nurses enough, we wouldn’t have this problem,” she said. “I would love to go back to staff nursing, but on my staff job, I would never be able to retire.”
The coronavirus exacerbated issues that were already driving health care workers out of their professions, Landhuis said. “A nursing shortage was on the horizon before the pandemic,” he said.
According to this year’s Nursing Solutions staffing report, nurses are exiting the bedside at “an alarming rate” because of rising patient ratios, and their own fatigue and burnout. The average hospital has turned over 100.5% of its workforce in the past five years, according to the report, and the annual turnover rate has now hit 25.9%, exceeding every previous survey.
There are now more than 203,000 open registered nurse positions nationwide, more than twice the number just before the pandemic in January 2020, according to Aya Healthcare.
An obvious short-term solution would be to keep using travel nurses. Even with salaries falling, however, the cost of hiring them is punishing.
LaNelle Weems, executive director of Mississippi Hospital Association’s Center for Quality and Workforce, said hospitals can’t keep spending like they did during the peak of the pandemic.
“Hospitals cannot sustain paying these exorbitant labor costs,” Weems said. “One nuance that I want to make sure you understand is that what a travel agency charges the hospitals is not what is paid to the nurse.”
Ultimately, it’s the patients who will suffer from the shortage of nurses, whether they are staff or gig workers.
“Each patient added to a hospital nurse’s workload is associated with a 7%-12% increase in hospital mortality,” said Linda Aiken, founding director of the University of Pennsylvania’s Center for Health Outcomes and Policy Research.
Nurses across the country told NBC News that they chose the profession because they cared about patient safety and wanted to be at the bedside in the first line of care.
“People say it’s burnout but it’s not,” Esmond said about why nurses are quitting. “It’s the moral injury of watching patients not being taken care of on a day-to-day basis. You just can’t take it anymore.”

A Kaiser Health News analysis of federal data published Sept. 9 highlights an increasing trend among hospitals — establishing independent, nonprofit health center “look-alikes” for primary care patients to improve their financial picture.
Federally qualified health center look-alikes, as designated by the federal government, deliver primary care services to underserved communities. They receive federally qualified health center prospective payment system reimbursement through CMS — a higher rate than if the sites were owned by the hospitals — as well as help with the recruitment and retention of primary care providers via HHS’ National Health Service Corps.
However, they don’t receive health center program funding from HHS to cover operational expenses.
Some hospitals increasingly view look-alikes as a strategy to help with their financial picture, since they can divert primary care patients without urgent needs to look-alike clinics from expensive emergency rooms, according to Kaiser Health News.
The Kaiser Health News analysis published Sept. 9 found that at least eight hospitals and health systems have converted or built new clinics designated as look-alikes from 2019 through 2022. This includes Mount Carmel, Ill.-based Wabash General Hospital, Beverly Hospital in Montebello, Calif., and Parrish Medical Center in Titusville, Fla., among others.
To read the full Kaiser Health News report, click here.

Fortune and Great Place to Work released their list of the “Best Workplaces in Health Care” on Sept. 7.
Survey responses from more than 161,000 employees were analyzed to determine the best workplaces in the healthcare industry. To be considered for the list, organizations were required to be Great Place to Work-Certified and be in the healthcare industry. Learn more about the methodology here.
Below are the nine best large health systems to work for, ordered by their corresponding number in the overall list of 30 organizations. Health systems with 1,000 or more employees were considered for the large category.
1. Texas Health Resources (Arlington)
3. Southern Ohio Medical Center (Portsmouth)
5. Northwell Health (New Hyde Park, N.Y.)
6. Baptist Health South Florida (Coral Gables)
7. OhioHealth (Columbus)
8. Scripps Health (San Diego)
9. WellStar Health System (Marietta, Ga.)
10. Atlantic Health System (Morristown, N.J.)
21. BayCare Health System (Clearwater, Fla.)
Fortune and Great Place to Work also released a list of the best small and medium healthcare organizations to work for. Organizations with up to 999 employees were considered for the small and medium category. No hospitals or health systems were listed in that category.

Moody’s Investors Service has downgraded MultiCare Health System’s revenue bonds to “A1” from “Aa3,” and revised the health system’s rating outlook to negative from stable.
Moody’s said the downgrade and the revision of the outlook to negative reflect several pressures that weaken the health system’s credit profile, including an unexpected 24 percent increase in debt, a decline in liquidity and significant operating losses through the first six months of fiscal 2022.
“Operations are expected to improve through the second half of fiscal 2022, but nevertheless full year results will remain weak, providing at best thin headroom to MultiCare’s debt service coverage covenant,” Moody’s said.
Moody’s noted that MultiCare, an 11-hospital system based in Tacoma, Wash., will continue to benefit from several strengths, including a large and growing revenue base and strong clinical offerings.
