Late last week, Salt Lake City, Utah-based Intermountain Healthcare and University of Colorado-affiliated UCHealth, based in Aurora, CO, shared that they are jointly developing a clinically integrated network (CIN). It will initially comprise 700 primary care physicians working at UCHealth’s 12 hospitals and hundreds of clinics, but may expand in the future. The CIN will leverage Intermountain’s value-based care expertise and its SelectHealth insurance plans. The two health systems will remain independent and operate the CIN as a separate company.
The Gist: This partnership continues Intermountain’s expansion into Colorado, after it finalized its merger with SCL Health in April of last year.
It’s a smart way for Intermountain to strengthen its foothold in the state, especially as further health system acquisitions in the Denver area may raise antitrust concerns.
Intermountain will be able to tap into a larger network ofphysician relationships that it can use tobolster its health plan, with significantly lower infrastructure costs compared to employment.
These types of partnership strategies may also be bed-warming for deeper relationships, with the opportunity to demonstrate value before a full-on merger.
Last Thursday, the Federal Trade Commission (FTC) released a proposed rule that would ban employers from imposing noncompete agreements on their employees. Noncompetes affect roughly 20 percent of the American workforce, and healthcare providers would be particularly impacted by this change, as far greater shares of physicians—at least 45 percent of primary care physicians, according to one oft-cited study—are bound by such agreements.
The rulemaking process is expected to be contentious, as the US Chamber of Commerce has declared the proposal “blatantly unlawful”. While it is unclear whether the rule would apply to not-for-profit entities, the American Hospital Association has released a statement siding with the Chamber of Commerce and urging that the issue continue to be left to states to determine.
The Gist: Should this sweeping rule go into effect, it would significantly shift bargaining power in the healthcare sector in favor of doctors, allowing them the opportunity to move away from their current employers while retaining local patient relationships.
The competitive landscape for physician talent would change dramatically, particularly for revenue-driving specialists, who would have far greater flexibility to move from one organization to another, and to push aggressively for higher compensation and other benefits.
Given that the FTC cited suppressed competition in healthcare as an outcome of current noncomplete agreements, the burden will be on organizations that employ physicians—including health systems and insurers, as well as private equity-backed corporate entities—to prove that physician noncompetes areessential to their operations and do not raise prices, as the FTC has suggested.
Radio Advisory’s Rachel Woods sat down with Optum EVP Dr. Jim Bonnette to discuss the sustainability of modern-day hospitals and why scaling down might be the best strategy for a stable future.
Rachel Woods:When I talk about hospitals of the future, I think it’s very easy for folks to think about something that feels very futuristic, the Jetsons, Star Trek, pick your example here. But you have a very different take when it comes to the hospital, the future, and it’s one that’s perhaps a lot more streamlined than even the hospitals that we have today. Why is that your take?
Jim Bonnette: My concern about hospital future is that when people think about the technology side of it, they forget that there’s no technology that I can name that has lowered health care costs that’s been implemented in a hospital. Everything I can think of has increased costs and I don’t think that’s sustainable for the future.
And so looking at how hospitals have to function, I think the things that hospitals do that should no longer be in the hospital need to move out and they need to move out now. I think that there are a large number of procedures that could safely and easily be done in a lower cost setting, in an ASC for example, that is still done in hospitals because we still pay for them that way. I’m not sure that’s going to continue.
Woods: And to be honest, we’ve talked about that shift, I think about the outpatient shift. We’ve been talking about that for several years but you just said the change needs to happen now. Why is the impetus for this change very different today than maybe it was two, three, four, five years ago? Why is this change going to be frankly forced upon hospitals in the very near future, if not already?
Bonnette: Part of the explanation is regarding the issues that have been pushed regarding price transparency. So if employers can see the difference between the charges for an ASC and an HOPD department, which are often quite dramatic, they’re going to be looking to say to their brokers, “Well, what’s the network that involves ASCs and not hospitals?” And that data hasn’t been so easily available in the past, and I think economic times are different now.
We’re not in a hyper growth phase, we’re not where the economy’s performing super at the moment and if interest rates keep going up, things are going to slow down more. So I think employers are going to become more sensitized to prices that they haven’t been in the past. Regardless of the requirements under the Consolidated Appropriations Act, which require employers to know the costs, which they didn’t have to know before. They’re just going to more sensitive to price.
Woods: I completely agree with you by the way, that employers are a key catalyst here and we’ve certainly seen a few very active employers and some that are very passive and I too am interested to see what role they play or do they all take much more of an active role.
And I think some people would be surprised that it’s not necessarily consumers themselves that are the big catalyst for change on where they’re going to get care, how they want to receive care. It’s the employers that are going to be making those decisions as purchasers themselves.
Bonnette: I agree and they’re the ultimate payers. For most commercial insurance employers are the ultimate payers, not the insurance companies. And it’s a cost of care share for patients, but the majority of the money comes from the employers. So it’s basically cutting into their profits.
Woods: We are on the same page, but I’m going to be honest, I’m not sure that all of our listeners are right. We’re talking about why these changes could happen soon, but when I have conversations with folks, they still think about a future of a more consolidated hospital, a more outpatient focused practice is something that is coming but is still far enough in the future that there’s some time to prepare for.
I guess my question is what do you say to that pushback? And are there any inflection points that you’re watching for that would really need to hit for this kind of change to hit all hospitals, to be something that we see across the industry?
Bonnette: So when I look at hospitals in general, I don’t see them as much different than they were 20 years ago. We have talked about this movement for a long time, but hospitals are dragging their feet and realistically it’s because they still get paid the same way until we start thinking about how we pay differently or refuse to pay for certain kinds of things in a hospital setting, the inertia is such that they’re going to keep doing it.
Again, I think the push from employers and most likely the brokers are going to force this change sooner rather than later, but that’s still probably between three and five years because there’s so much inertia in health care.
On the other hand, we are hitting sort of an unsustainable phase of cost. The other thing that people don’t talk about very much that I think is important is there’s only so many dollars that are going to health care.
And if you look at the last 10 years, the growth in pharmaceutical spend has to eat into the dollars available for everybody else. So a pharmaceutical spend is growing much faster than anything else, the dollars are going to come out of somebody’s hide and then next logical target is the hospital.
Woods: And we talked last week about how slim hospital margins are, how many of them are actually negative. And what we didn’t mention that is top of mind for me after we just come out of this election is that there’s actually not a lot of appetite for the government to step in and shore up hospitals.
There’s a lot of feeling that they’ve done their due diligence, they stepped in when they needed to at the beginning of the Covid crisis and they shouldn’t need to again. That kind of savior is probably not their outside of very specific circumstances.
Bonnette: I agree. I think it’s highly unlikely that the government is going to step in to rescue hospitals. And part of that comes from the perception about pricing, which I’m sure Congress gets lots of complaints about the prices from hospitals.
And in addition, you’ll notice that the for-profit hospitals don’t have negative margins. They may not be quite as good as they were before, but they’re not negative, which tells me there’s an operational inefficiency in the not for-profit hospitals that doesn’t exist in the for-profits.
Woods: This is where I wanted to go next. So let’s say that a hospital, a health system decides the new path forward is to become smaller, to become cheaper, to become more streamlined, and to decide what specifically needs to happen in the hospital versus elsewhere in our organization.
Maybe I know where you’re going next, but do you have an example of an organization who has had this success already that we can learn from?
Bonnette: Not in the not-for-profit section, no. In the for-profits, yes, because they have already started moving into ambulatory surgery centers. So Tenet has a huge practice of ambulatory surgery centers. It generates high margins.
So, I used to run ambulatory surgery centers in a for-profit system. And so think about ASCs get paid half as much as a hospital for a procedure, and my margin on that business in those ASCs was 40% to 50%. Whereas in the hospital the margin was about 7% and so even though the total dollars were less, my margin was higher because it’s so much more efficient. And the for-profits already recognize this.
Woods: And I’m guessing you’re going to tell me you want to see not-for-profit hospitals make these moves too? Or is there a different move that they should be making?
Bonnette: No, I think they have to. I think there are things beyond just ASCs though, for example, medical patients who can be treated at home should not be in the hospital. Most not-for-profits lose money on every medical admission.
Now, when I worked for a for-profit, I didn’t lose money on every Medicare patient that was a medical patient. We had a 7% margin so it’s doable. Again, it’s efficiency of care delivery and it’s attention to detail, which sometimes in a not-for-profit friends, that just doesn’t happen.
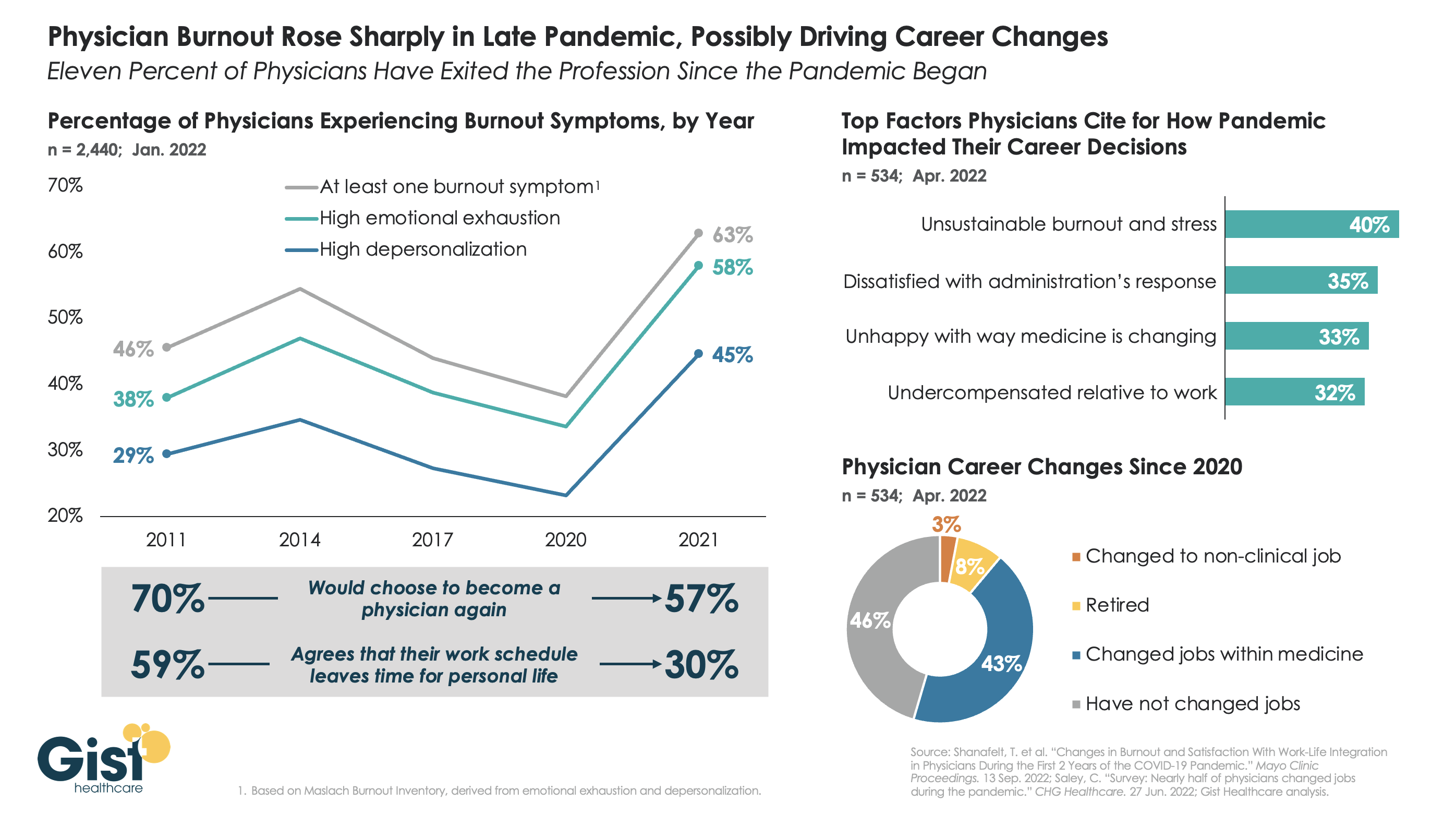
The long hours, stressful conditions, and labor shortages brought on by the pandemic have done serious harm to the physician workforce. The graphic above tracks physician burnout, a combination of emotional exhaustion, loss of agency, and depersonalization that has become the primary measure of the pandemic’s toll on workers, to reveal that physicians are demoralized like never before.
Physician burnout levels had been decreasing since 2014, in part due to practice consolidation and the expansion of team-based care models. Burnout reached its lowest levels in 2020—perhaps explained by a pandemic-induced sense of purpose—but 2021 then saw a dramatic spike in every measure of physician dissatisfaction, as the heroic glow of the early pandemic faded, and an overtaxed and understaffed delivery system became the new norm.
In explaining how the pandemic has impacted their career decisions, surveyed physicians list unsustainable burnout and stress as their top concern, and 11 percent say they have exited the profession, either for retirement or a non-clinical job, in the past two years.Four in ten surveyed physicians report changing jobs since 2020, mainly within similar or different practice settings, citing a desire for better work-life balance as their primary motivation. (It should be caveated that these data are from a smaller survey of 534 physicians, 40 percent of whom identified as “early career”.)
While the solutions here aren’t new, they are challenging: we must continue to implement team-based care models that provide physicians top-of-license practice and improved work-life balance, remove administrative tasks wherever possible, and ensure that we are communicating and engaging physicians—employed and independent alike—in organizational strategy and decision-making.
An enlightening piece published this week in Stat News lays out exactly how UnitedHealth Group (UHG) is using its vast network of physicians to generate new streams of profit, a playbook being followed by most other major payers. Already familiar to close observers of the post-Affordable Care Act healthcare landscape, the article highlights how UHG can use “intercompany eliminations”—payments from its UnitedHealthcare payer arm to its Optum provider and pharmacy arms—to achieve profits above the 15 to 20 percent cap placed on health insurance companies.
So far in 2022, 38 percent of UHG’s insurance revenue has flowed into its provider groups, up from 23 percent in 2017. And UHG expects next year’s intercompany eliminations to grow by 20 percent to a total of $130B, which would make up over half of its total projected revenue.
The Gist:
The profit motive behind payer-provider vertical integration is as clear as it is concerning for the state of competition in healthcare.
UHG now employs or affiliates with 70K physicians—10K more than last year—seven percent of the US physician workforce, and the largest of any entity.
Given the weak antitrust framework for regulating vertical integration, the federal government has proven unable to stop the acquisition of providers by payers. Eventually, profit growth for these vertically integrated payers will have to come from tightening provider networks, and not just acquiring more assets. That could prompt regulatory action or consumer backlash, if the government or enrollees determine that access to care is being unfairly restricted.
Until then, the march of consolidation is likely to continue.
When it comes to her feelings about investing in care delivery startups, it’s a real “mixed bag” for Ulili Onovakpuri, managing partner at Kapor Capital. This is because a lot of them operate on a cash-pay model. She summarized the issue quite succinctly: there’s an incredible amount of innovation happening, but the people who could benefit the most from this type of care will be the last ones to receive it.
Healthcare investors are facing a myriad of care delivery startups seeking their capital. And it’s an interesting time in the care delivery startup space — there’s more and more questions arising about how much scrutiny should be applied to the way these companies are growing, what should be included in their gross margins, and how they should be valued.
When it comes to her feelings about investing in care delivery startups, it’s a real “mixed bag” for Ulili Onovakpuri, managing partner at Kapor Capital. She said so Sunday at Engage at HLTH, a patient engagement summit hosted by MedCity News in Las Vegas.
Healthcare is a stratified experience in the U.S. Onovakpuri drew attention to the fact that this stratification is getting worse with the advent of provider startups that operate on a cash-pay model, such as Sesame and Tia.
These types of cash-pay providers usually offer a simpler healthcare experience compared to the endless bureaucracy and billing confusion patients face in the traditional healthcare system. This can be very attractive to patients — they don’t want to deal with months-long wait times to see a provider, nor do they wish to navigate the Kafkaesque ordeal of trying to understand and pay their healthcare bills.
In Onovakpuri’s view, these cash-pay providers “are good for some” — those who can afford it. But those who lack the means to pay for care outside the traditional healthcare delivery system don’t get to take part in these startups’ care model, regardless of how innovative or convenient it may be.
“If I’m honest, it’s hard for me because I see a lot of great tech every single day, and when I talk to them, I’m like, ‘Wait, this is awesome — how much is this?’ and then I say, ‘Well, we can’t do it because the people that we care the most about can’t afford it.’ And it’s hard, because they’re probably the folks who need it the most,” Onovakpuri said.
She summarized the issue quite succinctly: there’s an incredible amount of innovation happening, but the people who could benefit the most from this type of care will be the last ones to receive it.
“Innovation is great, but it’s another dividing factor we face,” Onovakpuri declared.
Onovakpuri noted another key concern: the fact that many of the country’s most talented physicians are opting to leave their hospitals and health systems to work for cash-pay care delivery startups. She said she can understand why they make this choice (they are understandably fed up with the inefficiency of standard systems), but it still is a problem because it exacerbates hospitals’ labor shortage crisis and makes their patients wait times even longer to receive care.
Last week, over 1,200 resident physicians and interns at Montefiore Medical Center, one of the largest employers in New York City, with four hospitals in the Bronx, held an organizing vote and requested voluntary recognition of their bargaining unit. The residents organized under the Committee of Interns and Residents, a unit of the Service Employees International Union that claims 22K members and has established unions at five hospitals this year. Roughly seven percent of practicing doctors were unionized as of 2019; that number has grown in the wake of pandemic-induced burnout and industry consolidation. Montefiore Medical Center declined to voluntarily recognize the union and has requested that the union re-form via a secret ballot election.
The Gist: Health system executives may see the possibility of resident unions as another headache amid the ongoing labor crisis, but the drivers of the crisis—burnout, workplace safety concerns, work-life balance, and real-wage erosion—are responsible for the growing appeal of unions for physicians. Fueled by economy-wide stressors, unionization has been growing in nontraditional labor sectors, including among baristas and tech workers, and medical residents may be the next to join that wave.
Health systems worried about resident unionization should address residents’ concerns about working conditions proactively, which may involve reevaluating wages in light of residents’ significant contributions to operational and financial success.
In a concerning New York Times article, reporter Gina Kolata relates the findings of a recent Health Affairs study that convened focus groups of physicians to anonymously discuss the ways they provide—or too often, don’t provide—care to disabled patients. Many admitted to avoiding seeing patients in wheelchairs and complained about having to provide accommodations to speech-impaired patients, citing the high costs of adapting their clinic operations while dealing with disruptions to workflow. People with disabilities interviewed for the article, including Harvard professor of medicine Dr. Lisa Iezzoni, who ran the study, found its results confirmed impressions of widespread bias against the disabled, which is pervasive across healthcare.
The Gist: Reducing disparities in access and quality of care for disabled people often receives less attention than reducing economic, racial, and gender disparities. What’s revealing about this piece is how these disparities among disabled patients manifest, ranging from personal biases (physicians not wanting or knowing how to care for certain groups of disabled people) to structural challenges (constraints of time, money, and facilities needed for proper care). However, for disabled patients, these factors result in an often substandard and unacceptable healthcare experience, which must be addressed head-on by physician and health system leaders.
Last week a health system chief medical officer asked if we were hearing other systems complain of difficulties in securing call coverage for key specialties, particularly orthopedics, GI and urology. We agreed: with proceduralists building larger outpatient businesses, often funded by investors, there is less incentive for groups to support hospital call. To fill the gaps, hospitals are having to negotiate lucrative deals for coverage, and the market feels like the “deal for every doc” years in the early 2000s, when specialists had leverage to negotiate bespoke partnership contracts. In this leader’s case, he ended up brokering a deal with gastroenterologists to serve in a hospital-based role, providing in-house coverage for consults. “These docs are able to make $600K a year, working about 30 hours per week. It’s insane,” he lamented.
But beyond the cost of talent, he was concerned about the larger ramifications of these kind of roles on physician supply. “I’ve been thinking about a metric along the lines of ‘lifetime physician hours worked’, and how that has changed over time,” he shared. He explained that physicians of his generation expected to work 60- to 80- hour weeks for most of their careers. Most younger doctors want to work much less, say 40 or 50 hours.
Over a forty-year career, he calculated, the healthcare system could get 36,800, or roughly a third fewer, “lifetime work-hours” from a doctor starting today. And most early-career doctors also plan to retire younger. “Now don’t get me wrong,” he continued, “We probably worked too hard, and these younger guys are onto something.” But he was concerned about the ramifications for physician supply, and posited we are poised for a deep shortage of clinical talent.
Creating the future physician workforce will require not only training more doctors, but also finding ways to make their work hours more efficient, with greater use of technology and other caregivers, who must also be trained in greater numbers. It takes at least four years to train a nurse, and nearly a decade before a student entering medical school today becomes a practicing physician—we can’t afford such a long lag time before more physician capacity comes online.