The first known U.S. case of the Omicron variant was detected in California, the Centers for Disease Control and Prevention confirmed Wednesday.
Driving the news: The confirmed case was detected in a traveler returning from South Africa who was fully vaccinated and has mild symptoms, according to the CDC.
Anthony Fauci, the director of the National Institute of Allergy and Infectious Diseases, had previously cautioned that the Omicron would “inevitably” be found in the U.S.
What they’re saying: “The recent emergence of the Omicron variant … further emphasizes the importance of vaccination, boosters and general prevention strategies,” the CDC said in a statement.
“We know what we need to do to protect people,” Fauci said following the announcement. “Get vaccinated if you’re not already vaccinated.”
Hospitals saw operating margins continue to erode in October, declining 12% from September under the weight of rising labor costs, according to a national median of more than 900 health systems calculated by Kaufman Hall. It was the second consecutive monthly drop and comes as facilities are preparing for the fast-spreading omicron variant of the coronavirus.
Although expenses remained highly elevated, patient days and average length of stay fell for the first time in months in October, likely reflecting lower hospitalization rates as the pressure of treating large numbers of COVID cases began to ease, Kaufman Hall said in its latest report.
At the same time, operating room minutes rose 6.8% from September, pointing to renewed patient interest in elective procedures.
Dive Insight:
Doctors and nurses have barely caught a breath from the most recent surge in inpatient volumes driven by the delta variant. Now, hospitals face the possibility of a fresh wave of cases led by omicron.
“Performance could continue to suffer in the coming months as hospitals face sustained labor increases and the uncertainties of the emerging omicron variant,” according to the Kaufman Hall report.
The new variant has not been detected in the U.S. as of Wednesday morning, but Canada is amongthe 20 countries that have confirmed cases.
Scientists are scrambling to understand the characteristics of the omicron variant. Anthony Fauci, director of the National Institute of Allergy and Infectious Diseases, told a White House press briefing Tuesday that omicron’s mutation profile points to “increased transmissibility and immune evasion.” But it is too soon to tell whether omicron will cause more severe disease than other COVID-19 variants, or how well current vaccines and treatments work against it, Fauci said.
Moderna CEO Stéphane Bancel told the Financial Times he thought existing vaccines would be less effective against omicron than earlier variants. Moderna, Pfizer, Johnson & Johnson and other manufacturers are already working to adapt their vaccines to combat the new threat, first reported by South African scientists on Nov. 24.
Regeneron also said its COVID-19 antibody drug, the top-selling treatment in the U.S., might be less effective against omicron. The company said it is now conducting tests to determine how the variant affects its drug.
The median hospital operating margin, not including federal Coronavirus Aid, Relief, and Economic Security Act funding, was down 31.5% in October, compared to pre-pandemic levels in the same month of 2019, according to Kaufman Hall’s snapshot. Hospitals in the West, South and Midwest that were hardest hit by the delta variant saw year-over-year margin declines.
Total labor expenses rose nearly 3% from September to October, 12.6% compared to October 2020 and 14.8% compared to October 2019, Kaufman Hall said. Full-time equivalents per adjusted occupied bed decreased 4.5% versus 2020 and 4% versus 2019, suggesting higher salaries due to nationwide labor shortages, rather than increased staffing levels, are driving up labor expenses.
Total non-labor expenses, however, decreased 1% in October from September for supplies, drugs and purchased services, following months of increases.
“Broader economic trends such as U.S. labor shortages are adding to the extreme pressures of the pandemic. Hospitals face greater uncertainties in the coming months as a result, as COVID-19 cases and hospitalizations appear to once again be on the upswing before many have even had a chance to recover from the last surge,” Erik Swanson, a senior vice president of data and analytics at Kaufman Hall said.
There’s a lot of talk about “natural immunity” to Covid-19, and some people are refusing vaccination onthe grounds that they’ve got this natural immunity thanks to a previous Covid-19 infection. In this episode we take a look at how infection and vaccination compare in terms of immunity, reinfection, and overall health risks and benefits.
In the era of great awakening, leaders have to step up and be conscious about building trust with people they work with.
The old rules and hierarchies, that were already becoming obsolete, have now been thrown out of the window. People look for integration of work and well-being knowing that work is what you do, not a place you go to.
Opportunities are abound and excellent people have ample choices (they always had). It is high time that organizations and leaders think this through carefully to first align their own mindset to this new reality and then take conscious actions to build teams, practices and processes that are not just high-performing but also have a strong fabric of trust woven in.
Employees, after all, are volunteers who exercise their choice of working with you. Effective leadership is about making it worth for them.
Building high-trust environment means putting the human back at the center of how a business functions and building everything – purpose, culture, processes, structures, rituals, systems, tools and mindsets – around it.
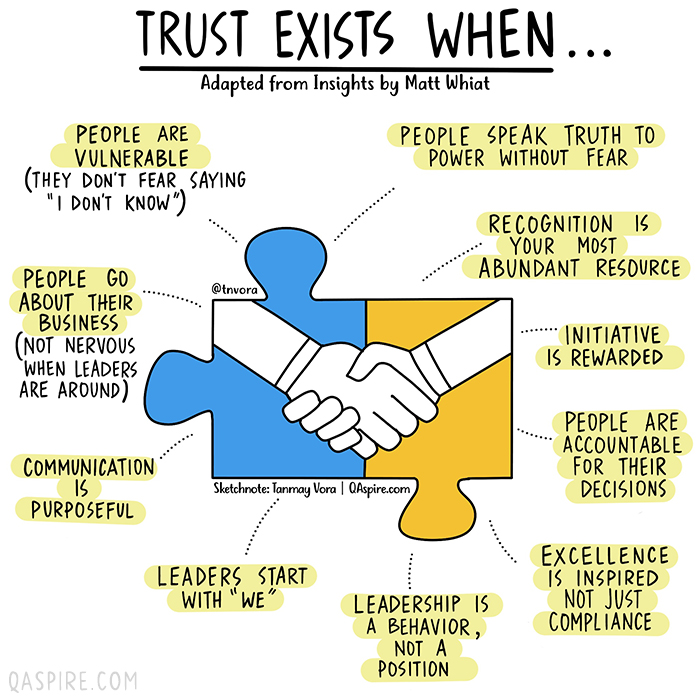
How would we know if we are working in an environment where we can trust others and that we are trusted? We can always answer this based on our intrinsic feeling but if you are a leader who is working hard to build trust, here are a few vital signs that you need to look for.
How much should we pay for drugs? That’s the question at the center of American Hospital Association v. Becerra, a sleeper of a case involving billions of dollars in federal spending and a chance to reshape two doctrines at the heart of administrative law.
Drugs, money, and the law: Sounds sexy, right? Still, you could be forgiven for never having heard of the case, which will be argued on Tuesday. It arises out of a technical dispute over how Medicare, the federal program that insures 63 million elderly and disabled people, pays for some of the drugs that hospitals dispense to patients in outpatient departments — in particular, chemotherapy drugs and other expensive anti-cancer medications.
The case centers on part of a 2003 law that gives Medicare two options for how to pay for those drugs. Under the first option, Medicare would survey hospitals about what it cost them to acquire the drugs. Medicare would then draw on the survey data and reimburse hospitals for their “average acquisition costs,” subject to variations for different types of hospitals. It’s a rough-cut way to make hospitals whole without requiring them to submit receipts for every drug purchase.
But Medicare immediately encountered a problem: It just wasn’t practical to survey hospitals about their acquisition costs. Fortunately, the law anticipated that possibility and gave Medicare a second option. In the absence of survey data, Medicare could pay the “average price” for the drug, “as calculated and adjusted by the Secretary [of Health and Human Services] as necessary for purposes of this [option].”
This approach turned out to be costly. A drug’s “average price” is fixed elsewhere in the Medicare statute, typically at 106% of the drug’s sale price. As a policy matter, this “average sales price plus 6%” approach is hard to defend. Because 6% of a large number is bigger than 6% of a small number, hospitals have an incentive to dispense more expensive drugs, even when there are cheaper and equally effective therapies.
Other developments soon made the payment policy look even more dubious. Back in 1992, Congress created something called the 340B program to support health-care providers that serve poor and disadvantaged communities. Eligible providers get steep discounts on the drugs that they purchase — anywhere between 20% and 50% of the normal price.
Initially, few hospitals qualified for the 340B program. Today, more than two-thirds of nonprofit hospitals participate. (For-profits are excluded from the program.) For years, Medicare kept paying those 340B hospitals 106% of the average sales price of their outpatient drugs. The upshot was that hospitals were buying highly discounted drugs and then charging the federal government full price. That heightened the incentive to prescribe very expensive medications — which is partly why Medicare spending on outpatient drugs has ballooned, growing an average of 8.1% per year from 2006 through 2017.
Federal regulators were troubled by the gap between hospital costs and Medicare payments. In their view, the point of the 2003 statute was to cover hospitals’ costs, not to subsidize 340B hospitals. That jibes with the Medicare statute more generally: Its “overriding purpose” is to provide “reasonable (not excessive or unwarranted) cost-based reimbursement.”
So Medicare adopted a rule that, starting in 2018, slashed the reimbursement rate for 340B hospitals’ outpatient drugs (or, more precisely, a subset of them) to 22.5% less than the average sales price. That was still generous, since on average the 340B discount is about one-third of a drug’s price. But it was much less generous than before, and Medicare estimated that the change would save taxpayers $1.6 billion every year.
The American Hospital Association, together with two hospital trade groups and three hospitals, filed suit. Had Medicare chosen option one, the plaintiffs argued, it could have focused on acquisition costs and even distinguished among hospital groups in setting payment rates. Instead, it chose option two, which says that Medicare must pay a drug’s “average price” — not its acquisition price — and doesn’t provide for discriminating between hospitals. While the plaintiffs acknowledged that Medicare could “adjust” the average price, they argued that a cut from 106% to 77.5% of the average sales price was not really an adjustment. It was a wholesale revision of the statutory scheme.
The plaintiffs encountered an obstacle right out of the gate. To prevent courts from second-guessing Medicare’s choices about how much to pay for outpatient care, the Medicare statute says that “[t]here shall be no administrative or judicial review” of those choices. In the government’s telling, Congress precluded review because Medicare has a fixed annual budget for outpatient care. Increasing payments for one type of care thus requires cutting payments for other types of care.
That linkage means that, if the plaintiffs win, it’s not just that they should have been paid more for certain drugs. It’s that all hospitals should have been paid less for other services. (That helps explains why coalitions representing rural and for-profit hospitals have filed amicus briefs in support of Medicare.) Unwinding that decision would be an administrative nightmare — which is why Congress precluded review in the first place.
As the plaintiffs see it, however, the government simply misreads the scope of the preclusion language. Though it generally precludes review of reimbursement decisions relating to outpatient care, it doesn’t cross-reference the subsection relating to outpatient drugs. Both the district court and the U.S. Court of Appeals for the District of Columbia Circuit agreed, invoking the strong presumption favoring judicial review of agency action.
On the merits, the plaintiffs fared less well. Though they won in the district court, the D.C. Circuit held that Medicare reasonably read the 2003 law to allow it to align hospital reimbursement with hospital acquisition costs. Medicare’s interpretation — and the scope of its authority to “adjust” payment rates — was thus owed deference under Chevron U.S.A. Inc. v. Natural Resources Defense Council, a 1984 decision holding that courts generally should defer to agencies’ reasonable interpretations of ambiguous statutes. Judge Cornelia Pillard dissented, arguing that the statute unambiguously foreclosed Medicare’s interpretation.
The plaintiffs asked the Supreme Court to review a single question: whether Medicare should receive Chevron deference for interpreting the 2003 law in the manner that it did. Tantalizingly, the plaintiffs noted that “[i]t is no secret that members of this Court have raised concerns about whether Chevron deference, particularly when applied as indiscriminately as it was in this case, violates the separation of powers.”
The Supreme Court bit. In its order granting certiorari, however, the court instructed the parties to brief an additional question: whether the Medicare statute precludes the lawsuit. What that means is that — in addition to resolving whether hospitals are entitled to billions of taxpayer dollars — the court will have the chance to address two foundational doctrines of administrative law: the presumption of reviewability and Chevron deference.
Arguably, AHA v. Becerraoffers an unusually vivid example of the costs of a strong presumption of reviewability. If the plaintiffs win, what’s the remedy? Is Medicare supposed to reopen every outpatient payment decision that it’s made since 2018, given that paying more for 340B drugs means it should have paid less for other services? The plaintiffs say no, arguing that Medicare wouldn’t be required to make any retroactive adjustments. But the government fears otherwise and the answer is not at all clear. Isn’t that the kind of mess that preclusion is meant to avoid?
I’ve called in my academic work for abandoning the presumption of reviewability precisely because it disrespects Congress’ reasonable desire to shield some administrative decisions from judicial review. In recent years, however, the Supreme Court has evinced no interest in doing so — the presumption of reviewability remains “strong.” We may soon find out just how strong it is.
But the big question about the case is whether the court will use it as a vehicle to reconsider Chevron deference. In the plaintiffs’ view, it is galling — “an affront to the separation of powers” — that the courts would defer when Medicare has exploited a purported ambiguity to sidestep Congress’ clear instructions about how much to pay hospitals. Several of the conservative justices, including in particular Justices Clarence Thomas and Neil Gorsuch, may be receptive to the argument. If so, the right wing of the court could use the case to narrow or even overturn Chevron, with potentially dramatic implications for the scope of executive-branch power.
Whether the court will do so is anyone’s guess. The justices could easily resolve the case on narrower grounds. Maybe the statute unambiguously forecloses Medicare’s interpretation of the law, as the plaintiffs argue. Or maybe, as the government claims, Medicare properly exercised its explicit authority to “adjust” prices for outpatient drugs.
Neither of those holdings would be the sexiest decision that the Supreme Court has ever issued. It would be technical, arcane — even boring. Given the financial stakes, however, it would be significant nonetheless.