

Cartoon – Our Employee Compensation Program


Surprise medical bills have become a major issue for Americans, but federal legislation to protect consumers continues to stall. Is Congress getting closer to halting this practice?
Listen to the full episode below, read the transcript or scroll down for more information.
Over the past two years, Congress has considered at least four bipartisan bills to protect patients from surprise charges, but all four have stalled. The proposals offer different approaches to determine how much insurers will pay out-of-network providers. These bills typically address the problem by adopting a payment standard, arbitration process or a hybrid of the two.
Insurers reimburse providers for out-of-network bills based on a set amount. Most bills propose using established in-network rates.
This process requires an insurer and provider to submit payment offers to a neutral party who makes the final call.
This approach combines the payment standard with arbitration to resolve disputes. An insurer pays a set amount, and if the provider disagrees, it can initiate arbitration.
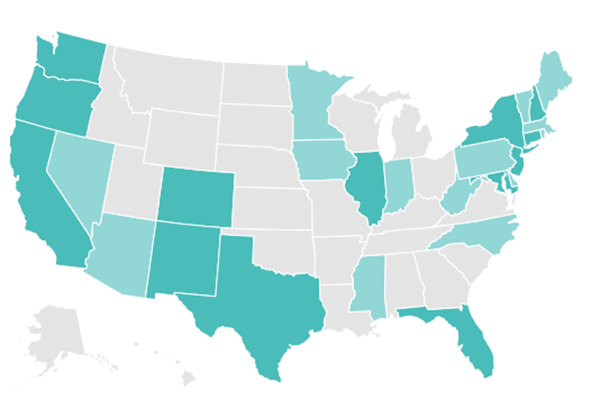
With federal solutions at a standstill, 30 states have passed varying levels of protections from surprise billing. As of July, 2020, 16 states have more comprehensive protections, which ensure that insured patients are only responsible for paying in-network costs, even when receiving care from out-of-network providers or emergency services at an out-of-network facility. Georgia was the latest state to pass such a law in July 2020. The other 14 states offer far more limited protections.
But even states with comprehensive protections cannot protect all patients from surprise medical bills. States are not able to regulate job-based coverage that falls under a federal law known as the Employee Retirement Income Security Act, which applies to most employer sponsored insurance. These patients remain vulnerable to surprise medical bills until Congress takes action to ban the practice.
Click on the map below for an interactive map from the Commonwealth Fund that details each state’s protections.
Despite strong bipartisan support for protecting patients from surprise bills, disagreement comes over how much physician groups should charge and how much insurers should pay. Essentially, resolving this issue may mean Congress has to pick sides.
As a result, stakeholders such as hospitals and private equity-backed physician groups, in particular, have pushed back on federal legislation, arguing that banning surprise billing will cripple their bottom line. These equity-backed physician groups have powerful lobbying groups, and in 2019, spent at least $5 million to persuade lawmakers to halt the legislation.
The pandemic has increased the risk that patients will unknowingly receive care from an out-of-network provider or at an out-of-network facility. The Trump administration tried to limit surprise bills for those in need of COVID-19 treatment by banning hospitals and providers that receive money from its Provider Relief Fund from sending balance bills to patients. But this approach leaves significant gaps and has had mixed success.
https://us3.campaign-archive.com/?u=6ab1fc39a0b1b15521551487c&id=6f9ac3fd86&e=ad91541e82
https://www.nejm.org/doi/full/10.1056/NEJMp2023312

This week’s contributor is Larry Levitt, the Executive Vice President for Health Policy at the Kaiser Family Foundation.
The study – by Sumit Agarwal and Benjamin Sommers, published in the New England Journal of Medicine – compares people who lost their jobs before and after the ACA went into effect in 2014 to see if there is a difference in how many people retained health insurance. During the pre-ACA period (2011-2013), there was about a 5% increase in the uninsured rate for people following a job loss. After the ACA went into effect (2014-2016), no such increase occurred. Instead, Medicaid and the marketplaces saw large increases in utilization.
If the economic crisis persists, the number of people losing job-based health insurance will climb, making the ACA’s role as a safety net more relevant than ever.

The healthcare industry added 75,000 jobs last month, a decline compared with the 126,000 that were added in July, the latest federal jobs report shows.
But there are some bright spots for the industry that is still recovering from major unemployment earlier this year sparked by job losses due to the COVID-19 pandemic.
The Bureau of Labor Statistics’ jobs report released Friday showed that hospitals continue to add more jobs after several major subsystems furloughed and laid off workers at the onset of the pandemic in March.
Hospitals added 14,000 jobs in August, which was below the 27,000 jobs the industry added in July.
The industry shed 26,000 jobs in May as hospitals took massive revenue hits from the cancellation of elective procedures and lower patient volume due to COVID-19.
Job numbers continue to recover robustly for other sectors of the healthcare industry.
Physician offices added 27,000 jobs and dentists another 22,000 in August. Home healthcare agencies added 12,000 positions in August.
But things continue to get worse for nursing homes.
Nursing homes and residential care facilities lost 14,000 jobs. But it was the lowest number of job losses the industry has faced in months.
In July the sector lost 28,000 jobs. In June, 20,000 positions were shed.
While several parts of the healthcare industry are adding jobs, the overall picture has been bleak. The federal government reported last month that healthcare employment has been down by nearly 800,000 jobs since February.
Things could continue to get worse for both hospitals and physician offices. Experts predict that hospital volumes, which have rebounded since major drops in March and April, are still below pre-pandemic levels for some facilities.

For-profit health systems have been better able to weather a financial crisis caused by COVID-19 than their nonprofit counterparts because they could reduce more expenses, a new analysis from the Medicare Payment Advisory Commission finds.
The analysis released Thursday during MedPAC’s monthly meeting comes as providers struggle to recover from low patient volumes stemming from the COVID-19 pandemic. The report also explored how physician offices have fared.
Hospitals faced a massive dip in patient volume in March and April at the onset of the pandemic, which forced facilities to cancel or delay elective procedures. Patient volumes have since recovered to near pre-pandemic levels, MedPAC found.
But the recovery has been mixed depending on the hospital system.
MedPAC looked at earnings for three large nonprofit systems in the U.S. and four large for-profit systems in the second quarter and found a variation in how they handled the decline in revenue.
Aggregate patient revenue for the nonprofit systems declined by $1.5 billion and this led to a $621 million loss for the systems in the second quarter compared to the same period in 2019. Overall the systems had operating profit margins ranging from negative 13% to positive 5%.
The four for-profit systems saw a $3.5 billion decline in patient revenue. However, the systems posted an increase of $634 million in operating income.
This led to a range of operating margin increases of 1 to 14% in the second quarter compared to 2019.
The for-profit systems got more relief funding ($1.9 billion compared with $782 million) from a $175 billion federal provider relief fund created by the CARES Act.
But the biggest difference between for-profit and nonprofit systems was how they handled expenses.
“For-profit systems substantially reduced expenses in the second quarter, in aggregate reduced by $2.3 billion and that made up for lost revenue,” said Jeff Stensland, a MedPAC staff member, during the meeting.
Nonprofit systems only saw a $13 million decline in expenses.
The analysis comes as some larger for-profit systems like HCA Healthcare generate profits in the second quarter, while nonprofit systems such as Providence posted losses.
MedPAC did not name the systems that it analyzed nor did it delve into what expenses were reduced and how.
Some systems have taken to furloughing employees but all systems have faced increased expenses for personal protective equipment and some staff.
The analysis also looked at the financial impact of the pandemic on physician offices. MedPAC found that federal grants, loans and payment increases offset a majority of the revenue lost in March and May due to patient volume declines.
MedPAC estimated physician offices lost between $45 to $55 billion. However, offices got $26 billion in loans from the Paycheck Protection Program, which don’t have to be repaid if the majority of the funds go to payroll.
Physician offices also received $5 billion out of the $175 billion provider relief fund passed as part of the CARES Act.
Physicians also got $1 billion in savings from the temporary suspension of a 2% decline in Medicare payments created under sequestration.

The merger of Einstein Healthcare Network and Jefferson Health is a matter of survival for Einstein’s flagship hospital, the two Philadelphia systems argued in a federal court filing this week, according to The Philadelphia Inquirer.
The health systems are attempting to overcome opposition to their merger from the Pennsylvania attorney general and the Federal Trade Commission.
A Sept. 14 hearing is slated on the FTC’s preliminary injunction request.
A court filing from the two health systems argued that Einstein, which has only had annual operating profits twice since 2012, is on a path to financial failure and needs $500 million to invest in key capital projects and deferred maintenance.
Without the infusion, Jefferson and Einstein said Einstein will continue to weaken “as it is forced to cut services or close facilities,” the Inquirer reported.
“Einstein was unable to identify any alternative buyer to Jefferson that possessed the financial strength and scale necessary to address Einstein’s financial problems,” the filing read, according to the Inquirer. “No other potential strategic partners were willing and able to commit to keep EMCP [Einstein Medical Center Philadelphia] open with its current set of services.”
The FTC announced in February its intent to sue to block the merger, arguing that combining the two systems would reduce competition in Philadelphia and Montgomery County.
“Jefferson and Einstein have a history of competing against each other to improve quality and service,” the FTC said in the February announcement. “The proposed merger would eliminate the robust competition between Jefferson and Einstein for inclusion in health insurance companies’ hospital networks to the detriment of patients.”
The FTC said that with a combination, the two parties would own at least 60 percent of the inpatient general acute care service market around Philadelphia and at least 45 percent of that same market in Montgomery County.


