
Cartoon – Getting Back to First Principles
https://mailchi.mp/9e0c56723d09/the-weekly-gist-july-8-2022?e=d1e747d2d8

Senate Democrats have reached a deal to give Medicare the power to negotiate drug prices, starting next year. The legislation includes provisions similar to those in the Build Back Better (BBB) Act, such as capping seniors’ out-of-pocket drug costs to $2,000 per year and limiting how fast drugmakers can raise prices.
This smaller package has support from moderate Senator Joe Manchin (D-WV), who blocked passage of the BBB last year. Manchin is reportedly open to using some of the estimated $1T in revenue from prescription drug negotiations to fund an extension of Affordable Care Act (ACA) insurer tax credits, which are set to expire this year.
The Gist: With a closely divided Senate and competing priorities, Democrats have been unable to pass significant healthcare reform since taking control in 2021.
If all 50 Senate Democrats can coalesce around this deal, it could pass under reconciliation rules without Republican support, allowing the party to deliver on its longstanding promise to lower prescription drug prices.
It would also help Democrats avoid a problematic “October surprise”: consumers receiving notices that their health insurance and drug plan premiums will be increasing just weeks ahead of the midterm elections.
https://mailchi.mp/9e0c56723d09/the-weekly-gist-july-8-2022?e=d1e747d2d8

Concierge primary care company One Medical is reportedly considering a sale after receiving interest from CVS Health, according to Bloomberg. While talks with CVS are no longer active, sources familiar with the situation say the company is weighing offers from other suitors. Also this week, there were rumors that Humana is interested in acquiring Florida-based Cano Health, which provides comprehensive care to over 200K seniors enrolled in Medicare Advantage plans across six states.
The Gist: We’ve long thought that the ultimate buyer for these primary care startups would be large, vertically integrated insurers, as many have struggled to achieve profitability while maintaining strong enrollment growth.
Competition among insurers to acquire care delivery assets has intensified, as payers look to Medicare Advantage as their primary growth vehicle, and aim to amass primary care networks capable of managing their growing senior care businesses.
https://mailchi.mp/9e0c56723d09/the-weekly-gist-july-8-2022?e=d1e747d2d8
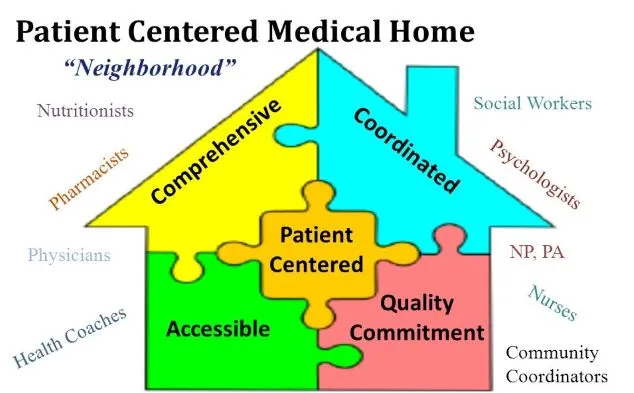
Although the patient-centered medical home (PCMH) practice model was first conceived over 50 years ago, its rapid adoption coincided with the launch of ACOs and value-based care. Primary care practices which adopted the medical home model expanded access and support available to patients, enhanced focus on chronic disease management, and embraced team-based care, with a focus on practice and provider sustainability.
But despite the model’s success, a recent conversation with a physician leader suggests that some of most progressive primary care practices are looking to move beyond the medical home. A primary care physician himself, he leads a network of hundreds of doctors, with nearly all the primary care practices PCMH-certified. He shared that “the medical home model in its traditional form doesn’t quite encapsulate what we’re trying to do now”. In his mind, it now feels paternalistic, focusing on what physicians think patients need without paying as much attention to what patients want from their healthcare.
We started brainstorming how a “consumer-centered medical home” might look. Built on the foundation of the PCMH, it would deliver access on the patient’s terms, bringing care online and into the home. Team-based care, supported by technology and even artificial intelligence tools, would enable easy, ongoing communication with patients.
As the list grew, it became increasingly clear that while a small practice could adopt the PCMH, scale is critical for these enhanced capabilities—being able to deliver more services to patients without increasing provider burnout. A tall order for sure, but an exciting vision for primary care that builds consumer loyalty in a competitive marketplace, while keeping the focus on improved care management and outcomes.
https://mailchi.mp/9e0c56723d09/the-weekly-gist-july-8-2022?e=d1e747d2d8

As the economic situation has worsened over the past few months, we’ve been working with several health systems to recalibrate strategy. For many, the anticipated “post-COVID recovery” period has turned into a struggle to reverse declining (often negative) margins, while still scrambling to address mounting workforce shortages. All this amid continued pressure from disruptive competitors and ever-rising consumer expectations.
In the graphic above, we’ve pulled together some of the most important changes we believe health systems need to make. These range from improvements to the operating model (shifting to a team-based approach to staffing, greater use of automation where appropriate, and moving to asset-light capital strategies) to transformations of the clinical model (moving care into lower-cost outpatient and community settings, integrating virtual care into clinical delivery, and creating tighter alignment with key physicians).
In general, the goal is to deliver lower-cost care in less expensive settings, using less expensive staff.
But those cost-saving strategies will need to be coupled with a new go-to-market approach, including new payment models that reward systems for shifting away from high-cost (and highly reimbursed) care models.
Employers and consumers will expect more solution-based offerings, which integrate care across the continuum into coherent bundles of service. This will require a more deliberate focus on service line strategies, moving away from a fragmented, inpatient-centric model.
Contracting approaches must align payment with this shift, changing incentives to reward coordinated, cost-effective, outcomes-driven care.
A key insight from our discussions with health system leaders: short-term cost-cutting initiatives to “stop the bleed” won’t suffice—instead, more permanent solutions will be required that address not only the core operating model, but also the approach to revenue generation.
The post-COVID environment is turning out to be a lot tougher than many had expected, to say the least.
https://mailchi.mp/9e0c56723d09/the-weekly-gist-july-8-2022?e=d1e747d2d8
In states with laws that criminalize performing abortions, physicians are facing the dilemma of having to wait until a pregnant patient’s death is imminent to perform a potentially lifesaving procedure. Reporting from STAT News reveals how these laws are disrupting care. A physician in Missouri, which outlaws all abortions unless the life of the mother is in danger, described having to spend hours getting clearance from a hospital ethics team to perform the procedure on a patient with an ectopic pregnancy.
Even non-pregnancy care is being impacted. An arthritis patient taking methotrexate, which can also be used for abortion, was told by her doctor that all prescriptions for the drug are on pause due to legal uncertainty.
The Gist: Doctors and hospital legal counsel are dealing with a new legal landscape, marked by restrictive, ill-defined anti-abortion laws that fail to clarify what constitutes a medical emergency.
Physicians are forced to interpret unclear laws, often written without help from medical professionals, and many feel compelled to wait until patients are in dangerous, life-threatening situations to provide care—the opposite of what was instilled in them during years of training.
https://mailchi.mp/9e0c56723d09/the-weekly-gist-july-8-2022?e=d1e747d2d8

As part of the 2023 Physician Fee Schedule proposed rule, the Centers for Medicare & Medicaid Services (CMS) outlined major changes to the Medicare Shared Savings Program (MSSP), with the goals of increasing participation in the program and improving health equity.
The agency hopes their revisions to the benchmarking methodology, which will advantage smaller accountable care organizations (ACOs) and those enrolling large numbers of underserved beneficiaries, will change the trajectory of the program.
With participation among providers stagnating in recent years, the new rules represent a recognition from CMS that MSSP, in its current form, is likely to increase spending rather than generate significant savings. The rule also includes a 3.9 percent decrease in the “conversion factor” for physician payment, which has already drawn outrage from the American Medical Association and other physician groups.
The Gist: There is little reason to expect that these modifications—as significant as they are—will be meaningful to beneficiaries or to the Medicare program’s overall sustainability. Although it is heartening to see CMS admit that ACOs are on course to violate the statutory requirement that the program not increase spending, the proposed changes would net only $14.8B in savings over a twelve-year period—a rounding error for a program that spent $830B in 2020 alone. Meanwhile the 11M beneficiaries attributed to MSSP ACOs are dwarfed by the 28M enrolled in MA.
For many health systems and physician groups—particularly those who are most progressive in managing risk—MSSP is now a sideshow to their Medicare Advantage (MA) strategies. The federal government has made two “bets” on how to lower health spending for seniors, and the dollars spent on enticing insurers to grow their MA businesses (in the form of subsidies) far outweigh the effort to encourage provider participation in ACOs—a clear sign of Medicare’s priorities.
But with MA currently not generating savings compared to fee-for-service Medicare, cuts in per-beneficiary spending in MA will be necessary to achieve savings in the long term.
As this summer heats up, so has the spread of the hot new version of COVID-19.
Why it matters: This subvariant of Omicron called BA.5 — the most transmissible subvariant yet — quickly overtook previous strains to become the dominant version circulating the U.S. and much of the world.
BA.5 is so transmissible — and different enough from previous versions — that even those with immunity from prior Omicron infections may not have to wait long before falling ill again.
What they’re saying: “I had plenty of friends and family who said: ‘I didn’t want to get it but I’m sort of glad I got it because it’s out of the way and I won’t get it again’,” Bob Wachter, chairman of the University of California, San Francisco Department of Medicine told Axios. “Unfortunately that doesn’t hold the way it once did.”
State of play: This week, the CDC reported BA.5 became the dominant variant in the U.S., accounting for nearly 54% of total COVID cases. Studies show extra mutations in the spike protein make the strain three or four times more resistant to antibodies, though it doesn’t appear to cause more serious illness.
Yes, but: “I’m certainly hearing about more reinfections and more fairly quick reinfections than at any other time in the last two and a half years,” Wachter said.
Zoom in: That is also largely the experience of the surge seen firsthand in New York City by Henry Chen, president of SOMOS Community Care, who serves as a primary care physician across three boroughs of the city.
The big picture: Another summertime wave of cases could prolong the pandemic, coming after many public health precautions were lifted and with available vaccines losing their efficacy against the ever-evolving virus.
The bottom line: The messaging isn’t to panic, but to understand the virus is likely spreading in local communities much more than individuals realize due to shrinking testing programs — and without the level of protection they might assume they have.

The U.S. economy added 372,000 jobs last month, while the unemployment rate held at 3.6%, close to the lowest level in a half-century, the government said on Friday.
Why it matters: Jobs growth remains healthy, even as the Federal Reserve tries to slam the brakes on the economy to contain decades-high inflation.
By the numbers: Job gains in April and May were 74,000 lower than initially estimated.
The backdrop: There has been a spate of companies announcing layoffs, rescinding job offers and pausing hiring, though these developments have largely been concentrated in sectors like housing and technology.
