
Cartoon – Health Insurance Industry Profits

Oakland, Calif.-based Kaiser Foundation Health Plan, Kaiser Foundation Hospitals and their subsidiaries reported a net loss of $1.5 billion for the quarter ending Sept. 30, according to a Nov. 4 financial report.
The company posted total operating revenues of $24.3 billion and total operating expenses of $24.3 billion for the quarter. Total operating revenues of $23.2 billion and total operating expenses of $23.1 billion for the same period in 2021.
Additionally, there was an operating loss of $75 million in the third quarter compared to an operating income of $38 million in the third quarter of 2021, according to a Nov. 4 news release.
“I am proud of our ability to navigate the challenges of the past few years, including a global economic crisis, the high cost of goods and services, supply chain issues, labor shortages, and the pandemic while serving our 12.6 million members,” said Greg Adams, chair and CEO of Kaiser Permanente.
The net loss of $1.5 billion in the third quarter of 2022 compares to a $1.6 billion net income in the third quarter of 2021. Capital spending totaled $2.5 billion year-to-date.
“We are grateful to our extraordinary people whose commitment and compassion allow us to continue to fulfill our mission of providing high-quality and affordable care and improving the health of our communities,” said Tom Meier, corporate treasurer of Kaiser Permanente.
https://mailchi.mp/46ca38d3d25e/the-weekly-gist-november-4-2022?e=d1e747d2d8

According to reporting from Bloomberg, primary care company VillageMD, which is majority-owned by Walgreens, is engaged in talks to merge with New Jersey-based Summit Health, a large medical group network and urgent care chain backed by private equity firm Warburg Pincus.
In 2019, Summit merged with CityMD, a New York City-based urgent care chain, and operates over 370 clinic locations based in and around New York City, as well as in central Oregon. The combined entity would be valued between $5B and $10B.
The Gist: Should this deal go through, it would epitomize recent trends in healthcare M&A: a well-established independent medical group using private equity funding to rapidly expand its operations before selling off to an industry giant.
If that industry giant ends up being VillageMD, Walgreens would finally have a physician practice with deep experience in managing risk, on which they can anchor their larger ambitions in care provision. And if the deal with Walgreens falls through, Summit, with its combination of mostly suburban value-based care practices and largely urban urgent care chains, is sure to attract plenty of other suitors, including any of the major national insurers.
https://mailchi.mp/46ca38d3d25e/the-weekly-gist-november-4-2022?e=d1e747d2d8
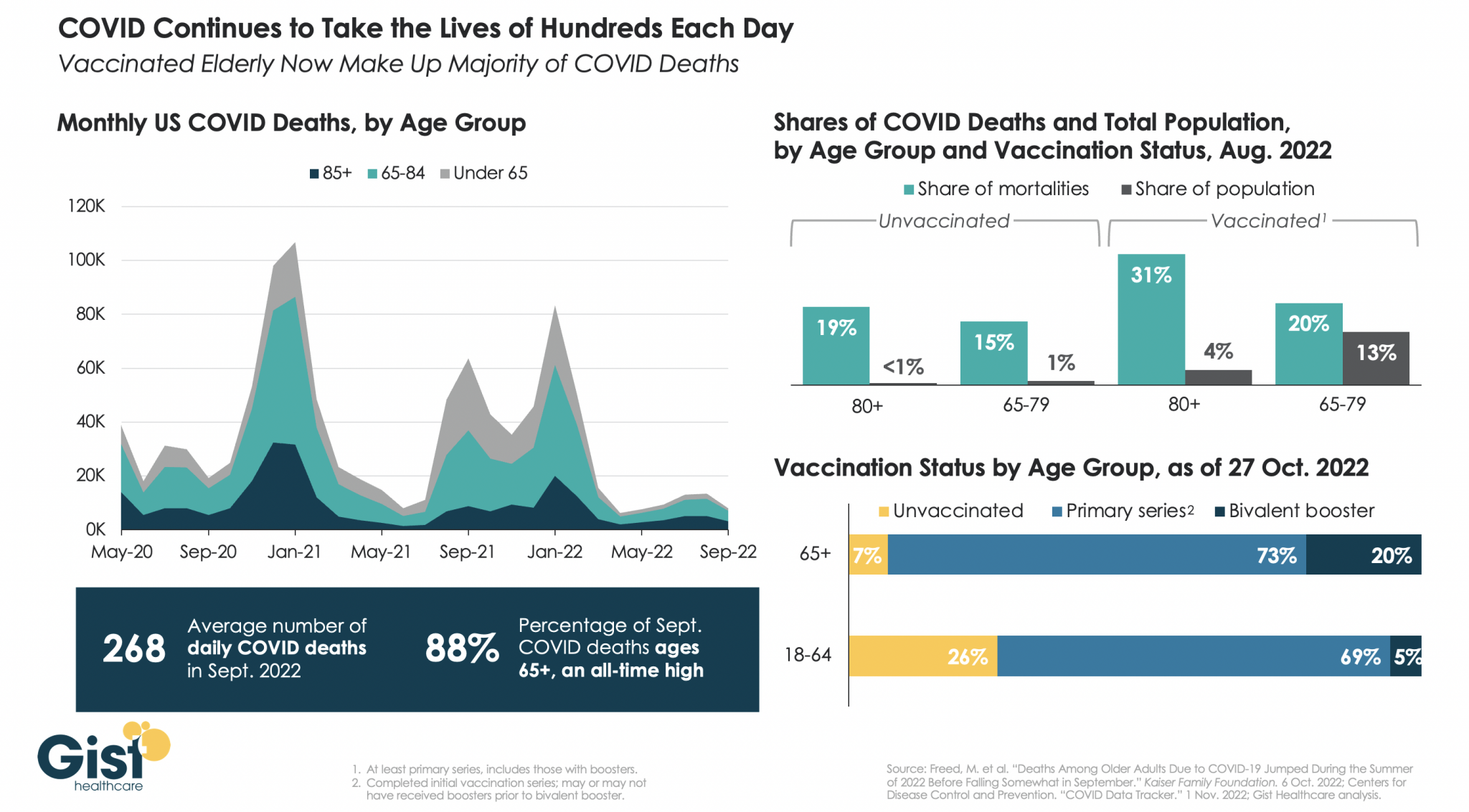
While we have mercifully moved beyond the crisis phase of the pandemic, COVID remains a leading cause of US deaths, taking the lives of hundreds of Americans each day.
In the graphic above, we analyzed COVID mortality data, finding the defining characteristic of Americans still dying of COVID is age. As death rates have dropped, the percentage of COVID deaths accounted for by individuals 65 years or older has risen to an all-time high of 88 percent.
Notably, a majority of people dying of COVID today are vaccinated, due to the high rate of vaccination in the 65+ population. While the near-universal vaccination of seniors, including the fact that one in five have received the most recent bivalent booster, is not sufficient to save all of their lives, unvaccinated seniors are still dying at higher rates than vaccinated ones.
In August 2022, vaccinated individuals over age 80, who represent about four percent of the total US population, made up 31 percent of COVID deaths, while unvaccinated individuals in the same age group, who represent less than one percent of the total population, made up 19 percent of COVID deaths.
We entered 2020 with about 55M Americans ages 65 and older, and have since lost 790K, or nearly 1.5 percent of the senior population, to COVID. Meanwhile, reports of the new, immune-evasive BQ variant sweeping New York and California remind us that COVID’s not done with us yet, even if we think we’re done with it.
https://mailchi.mp/46ca38d3d25e/the-weekly-gist-november-4-2022?e=d1e747d2d8

In a recent STAT News article, reporters Tara Bannow and Bob Herman took an in-depth look at private-equity firm Welsh, Carson, Anderson & Stowe, examining the performance of four of its healthcare portfolio companies. They show how the firm’s A-list partners, clients, and board members have promoted controversial business practices—often at the expense of publicly funded healthcare programs—that conflict with its well-curated public image.
The Gist: This article emphasizes how the complex and opaque regulatory structure of American healthcare allows motivated parties like PE firms to find technically legal, though ethically suspect, business models, which can easily tip over into outright illegality.
It highlights the “revolving door” flow of executives between industry and government, which allows investment firms to play a long game by actively shaping the regulatory landscape and lobbying to create business opportunities where none previously existed. Justified backlash at “gotcha” business models and profit-seeking at the expense of vulnerable patients may swamp any positive contribution that PE investment and rollups may make to the business of healthcare.
https://mailchi.mp/46ca38d3d25e/the-weekly-gist-november-4-2022?e=d1e747d2d8

Tuesday marked the start of the tenth season of open enrollment in the ACA’s health insurance exchanges. Last year, a record 14.5M Americans obtained coverage through the exchanges, and this year’s total is expected to surpass that. That’s thanks to the extended subsidies included in the Inflation Reduction Act, a fix to the “family glitch” that prevented up to 1M low-income families from accessing premium assistance, and expanded offerings by most major insurers, who have been enticed by the exchanges’ recent stability. The average unsubsidized premium for benchmark silver plans in 2023 is expected to rise by about four percent, but the enhanced financial assistance will lower net premiums for most enrollees.
The Gist: ACA marketplace enrollment has grown nearly 80 percent since opening in 2014, and exchange plans now cover 4.5 percent of Americans. After enrollment lagged during the Trump administration, the combination of policy fixes and improved risk pools are attracting insurers back into the exchanges, where enrollees are finding more affordable plans than ever before.
We consider this a commendable first decade, but the success of the exchanges over the next ten years remains subject to political winds. Congress must revisit the extended subsidies by 2025, and a different administration might deprioritize marketplace advertising and navigation support, policies have which proven crucial to the exchanges’ recent growth.
https://mailchi.mp/46ca38d3d25e/the-weekly-gist-november-4-2022?e=d1e747d2d8

Physicians are set to see a 4.5 percent decrease in Medicare payment next year, in part due to the expiration of a temporary payment boost that was passed by Congress in December 2021 to avert scheduled sequester cuts. Physician groups are expected to lobby lawmakers heavily in the final months of the year, hoping to secure a reprieve, especially as inflation and labor costs continue to rise.
Other changes in the 2023 rules include advance payments to new participants in the Medicare Shared Savings Program, intended to boost participation of providers in rural and underserved areas. Some pandemic-era telehealth flexibilities that are set to expire with the end of the federal COVID public health emergency were also extended.
The Gist: We do not expect the full Medicare physician reimbursement cut to physicians to go into effect, as a bipartisan group of Senators has already asked leadership to address it in the upcoming lame-duck session. However, the cut serves the important purpose of rebasing negotiations between physician lobbies and Congress, such that keeping rates flat or obtaining a small boost would feel like a win for both groups—even if it falls far short of the rate increases needed to meet the rising cost of running a practice.
If Congress continues to intervene to push off or mitigate Medicare’s sequestration payment reductions, we could find ourselves back in a Sustainable Growth Rate (SGR)-type situation where a payment cut constantly looms, physicians continually lobby for yet another reprieve, and the delayed cuts balloon in size.

I began to wonder if this trip to a pediatric urgent care with my son was even necessary.
Sure, he had been diagnosed with pneumonia a week ago and didn’t seem to be getting better. His cough sounded uglier. But here Ethan was in classic two-and-a-half-year-old mode: running in big circles around the waiting room chairs and causing the kind of ruckus only a toddler can.
He’d stuff some Pirate’s Booty I had hastily thrown into my purse in his mouth, before returning to his wild banshee ways and dashing around in circles again.
Our pediatrician said their office was too swamped with sick kids to see us, and referred us to this place. We had been told the wait to see a doctor would be a minimum of an hour. We struggled to find a seat in the packed waiting room as far as possible from other coughing kids.
We finally graduated from the waiting room to the doctor’s office, only for Ethan to continue his marathon by scooting a rolling chair back and forth, roaring with laughter every time it hit the examining table. When the physician walked in, I felt like I needed to defend wasting her time with this visit with my seemingly A-OK, albeit destructive, son.
But Ethan wasn’t OK.
The doctor listened to his chest with her stethoscope and didn’t like what she heard: wheezing, some crackling.
She showed me how Ethan’s Pirate’s Booty-stuffed stomach moved heavily each time he inhaled and exhaled.
They had Ethan complete a nebulizer treatment in the office, which meant slipping a device on his face that resembled an oxygen mask, while medicated air meant to open up his lungs flowed through a frightfully loud machine. I held him in my lap while the nebulizer was on, scrambling to find 100 different versions of “Wheels on the Bus” videos on YouTube to try to distract him from the vacuum-like whirring of the machine.
The doctor listened to his lungs again. His breathing still didn’t sound great, but she said the hospitals were too inundated right now.
I knew all too well what she meant. A few days before our urgent care visit, I had flagged a report for editors at The Hill that said children’s hospitals in the Washington area were at capacity, flooded with young kids suffering from RSV, a potentially life-threatening respiratory illness that has no vaccine.
After a three-hour visit, she gave Ethan a steroid and told us to follow up with his pediatrician the next day.
By the time we got to the pediatrician’s office the following morning, my happy-go-lucky, playful little guy was anything but. He curled up in my lap, as we went through a similar routine that the urgent care doctor had done just the night before. His oxygen levels were too low, and our pediatrician had him do another nebulizer treatment.
“Our goal is to keep you from going to the hospital,” our pediatrician told us.
It seemed like an unusual “goal” from a doctor, but I understood her reasoning. But after Ethan’s oxygen levels dipped lower still after the nebulizer, she said we should rush him straight to the hospital after all.
My “Blue’s Clues” and vehicle-obsessed son, usually the epitome of toddler “I can do it myself!” independence, wouldn’t let me put him down for even a moment as we waited in the emergency room lobby. Surprisingly, a separate waiting area in the ER just for children wasn’t completely full, and I wondered if maybe news reports of endless waits were overblown.
Not so.
“He’s so cute,” a young mother in the waiting room told me, as she motioned to Ethan’s head of curls. She cradled her two-month-old in her arms, patiently rocking the baby after telling me she had waited three hours so far.
I held Ethan as my husband rushed from work to the hospital, meeting us there and with us as we were brought to an ER triage area. They ran more oxygen tests on Ethan, got some of his history, and then sent us back to the waiting room.
Finally, they called Ethan’s name and we were in the ER. My vibrant, otherwise-healthy kid was lethargic, laying on me with a glazed look in his eyes. We struggled to fit the two of us on an exam table meant for a single adult. They draped a lead apron over me and Ethan as they took X-rays of his tiny lungs. The nurse placed a cannula in Ethan’s nose for supplemental oxygen and put an IV in his arm to give him fluids, before wrapping it with a diaper so he wouldn’t try to take out the tube.

My husband and I, loopy from what was happening, laughed at the sight of a diaper being used MacGyver-style. “Hey, it works!” the nurse said, explaining that he’d done the maneuver with kid after kid in recent weeks.
The ER doctor finally came in our room and delivered a crash course in what might be to come. “Everywhere is full. The entire Eastern seaboard,” he said of hospitals.
“We’ve been airlifting kids to Pittsburgh, sometimes to Richmond,” he added. This hospital had a pediatric unit, but not an intensive care geared towards kids. So if Ethan’s condition became even more dire, they wouldn’t be able to treat him there. Our only hope was that the pediatric unit, which had just a few remaining beds, accepted him.
It was a gut punch. As the doctor left, my husband looked at Ethan, who had fallen asleep with a mask on as the nebulizer loudly buzzed away for another treatment.
“He’s just a baby. He’s not supposed to be here,” my husband said, defeated.
The pediatric unit doctor finally came into our room. She examined Ethan, and briefed us on how they’ve been dealing with case after case of the same thing: RSV.
But she offered us hope: he could head to the pediatric unit at the hospital. We wouldn’t need to travel for his care, as long as he didn’t worsen. Ten hours after we first entered the hospital, we had a bed for Ethan.
We’re among the lucky ones. We were told beyond airlifting, plenty of families had been spending multiple nights in the ER because there were no beds.
In Maryland, Gov. Larry Hogan (R) announced last week that that hospitals would receive $25 million in additional funding from the state to prioritize pediatric intensive care unit staffing. Children from birth to age two comprised 57 percent of hospitalizations last week, according to Hogan’s office.
Next to the ghost decorations for Halloween adorning the doors of the pediatric unit, room after room had the same notice taped up: isolation guidelines. The rooms were all filled with kids facing the exact same thing as Ethan. RSV was everywhere.
There’s no cure for RSV. Every two hours on the dot, the nurses would give Ethan the nebulizer treatment.

A monitor affixed to his foot would alert nurses if his oxygen dipped dangerously low, which it did several times throughout the first night. I thought at one point to ask what happens if Ethan stopped responding to the treatments, but then didn’t ask because I didn’t want to know the answer.
The goal was to get him going without the need for additional oxygen, and breathing well for at least four hours between treatments, two times in a row.
That seemingly simple goal proved elusive for two full days. I originally thought it would be a nightmare trying to get a two-year-old to stay in a hospital bed for more than five minutes, but Ethan was in such bad shape that he barely made a fuss. Then, after midnight on our second night in the hospital, Ethan suddenly perked up.
He sat up and rolled over in the hospital bed. Then, he rolled onto my head, spreading his arms and legs out as far as he could stretch, and giggled.
“Should I sleep here?” he said, cracking himself up.
It was like someone hit the power button on my kid, and suddenly he snapped back to himself. I didn’t care that it was midnight and we needed to get some extremely interrupted sleep before the next nebulizer treatment. My son was back.
A nurse later told me that she enjoyed working with kids because for as quickly as their health can deteriorate, they can just as speedily bounce back.
After that, the doctor advised us to try stretching out his time between treatments. Finally, we were told he was stable enough to go home. I somehow hadn’t shed a tear the entire time we were at the hospital, but when the doctor signed off on us leaving, I bawled.
As nightmarish an experience as it was, I realize how incredibly fortunate my family is.
My husband and I have jobs that allowed us to drop everything when our son needed help, we have health insurance policies, and resources to get through spending days at the hospital.
Perhaps most importantly, we had access to an incredible team of doctors and nurses and the sheer fortune of being able to get a bed for our son during an unprecedented and unthinkable time for hospitals.
At the risk of repeating one of those parenting cliches that I would’ve rolled my eyes at a week ago, I’m thankful that I trusted my gut. Even when Ethan was being a wild child at urgent care, I knew something just wasn’t right. What I didn’t know was how much he had been struggling to breathe.
At the hospital after being discharged, Ethan and I waited in the lobby as my husband went to get our car from the parking lot to pick us up. Ethan spotted some empty wheelchairs in the corner of the lobby, and immediately ran over to them. He giggled as he tried to roll one of the chairs into the automatic opening and closing doors. As I looked on as he laughed and laughed at the pint-sized commotion he created, I breathed a sigh of relief.
https://www.axios.com/2022/11/04/october-job-report-2022-release

The labor market remained solid in October: the U.S. economy added 261,000 jobs, while the unemployment rate rose to 3.7% from 3.5%, the government said on Friday.
Why it matters: The last major economic report before the midterm elections shows that while jobs growth has slowed, employers continue to add workers at a robust pace as the labor market defies fears of a recession.
Driving the news: October’s jobs gains were above the 205,000 payrolls economists expected. It’s a slightly slower pace than the 315,000 jobs added in September, which was revised higher by 52,000.
The backdrop: The Federal Reserve this year has raised interest rates at historically rapid pace in an effort to slow the economy and, in turn, beat back soaring inflation. Many economists warn that the U.S. will soon enter a recession. Still, the labor market has chugged along.
That is worrisome for the Fed, which fears the too-hot labor market will stoke inflation. But, on the flip side, it’s been great for American workers — though the booming job market has been coupled with decades-high inflation that’s eaten away at wage gains.

