
Author Archives: henrykotula
3 Ascension Texas hospitals to pay $20.9M for alleged kickbacks
:max_bytes(150000):strip_icc()/GettyImages-477514725-c4271ad485734ba6b84cae22be7833cf.jpg)
Three Ascension hospitals in Texas agreed to pay $20.9 million for allegedly paying multiple physician groups above fair market value for services, according to a recent news release from the HHS’ Office of Inspector General.
The three Texas hospitals are Ascension’s Dell Seton Medical Center in Austin, Ascension Seton Medical Center Austin and Ascension Seton Williamson in Roundrock. Ascension self-disclosed the conduct to the inspector general.
The hospitals allegedly violated the Civil Monetary Penalties Law, including provisions related to physician self-referrals and kickbacks in seven instances, according to the April 30 news release.
Some of the allegations the report outlined include Dell Seton paying an Austin physician practice above fair market value for on-call coverage; Ascension Seton Austin paying an Austin practice above fair market value for transplant on-call coverage and administrative services; and Ascension Seton Williamson paying a practice above fair market value to lease the practice’s employed registered nurses and surgical technologists who assisted in surgeries at the hospital.
The release did not disclose the physician groups allegedly involved.
Access the full release here.
CommonSpirit posts $1.7B net income in Q3

After posting a $1.4 billion net loss in the third quarter of fiscal year 2020, CommonSpirit, a 140-hospital system based in Chicago, saw improved finances in the third quarter of fiscal year 2021, according to financial documents released May 14.
CommonSpirit, formed in 2019 through the merger of San Francisco-based Dignity Health and Englewood, Colo.-based Catholic Health Initiatives, reported revenues of $8.8 billion in the third quarter of fiscal 2021, up from $7.8 billion recorded in the same quarter one year prior. The health system said the third quarter of fiscal 2021 was the first period to fully include results from Virginia Mason Fransican Health, an 11-hospital system that was formed in January and joined the CommonSpirit network.
The health system’s operating expenses also increased year over year. It reported total expenses of $8.3 billion in the third quarter of fiscal 2021, compared to about $8 billion recorded in the same period last year.
CommonSpirit ended the third quarter of fiscal 2021 with an operating income of $539 million, a figure that included federal relief aid and a pre-tax gain on the sale of joint venture shares. CommonSpirit said without the aid and pre-tax gain, the health system would have posted an operating loss of $117 million in the quarter ended March 31, “highlighting the continuing concerns around overall patient volumes and the ongoing impact of the pandemic.”
After factoring in $1.2 billion in non-operating income, including $636 million in investment income, CommonSpirit posted a net income of $1.7 billion in the quarter ending March 31. In the same quarter one year prior, CommonSpirit recorded a net loss of $1.5 billion.
“In many ways this quarter was similar to what we experienced over the last year, with a very challenging period followed by a robust recovery,” said CommonSpirit CFO Dan Morissette in a May 14 news release. “With vaccination rates rising and many people returning to their pre-pandemic routines, we expect to continue a strong path to recovery, while also recognizing that we will likely see operational impacts from the pandemic for quite some time.”
CommonSpirit said it also is working to strengthen its financial foundation by realizing operational synergies this year. The goal is to realize $350 million to $400 million in savings during fiscal 2021, and it is on track to meet or surpass that goal.
Walmart, Amazon continue to build healthcare presence

Late last week, retail giant Walmart announced its plan to acquire national telemedicine provider MeMD, for an undisclosed sum. According to Dr. Cheryl Pegus, Walmart’s executive vice president for health, the acquisition “complements our brick-and-mortar Walmart Health locations”, allowing the company to “expand access and reach consumers where they are”.
MeMD, founded in 2010, provides primary care and mental health services to five million patients nationally. The acquisition extends Walmart’s health delivery capabilities beyond the handful of in-store and store-adjacent clinics it runs, and follows the launch of its own Medicare Advantage-focused broker business, and partnership with Medicare Advantage start-up Clover Health to offer a co-branded insurance product.
Walmart has been climbing the healthcare learning curve for several years, building on its sizeable retail pharmacy business, and seems to have hit on a successful formula in its latest in-person clinic model, which includes primary care, behavioral health, vision, and dental services. The retailer plans to add 22 new clinic locations by the end of this year, and its new telemedicine offering will allow it to expand its virtual reach even further.
The MeMD acquisition also represents a new front in Walmart’s head-to-head competition with Amazon, which launched its own national telemedicine service earlier this year. That service, Amazon Care, is targeted at the employer market, and right on cue, Amazon announced its first customer sale last week—to Precor, a fitness equipment company.
Both retail giants are slowly circling the $3.6T healthcare industry, targeting inefficiencies by deploying their expertise in convenience and consumer engagement. Incumbents beware.
Should hospitals mandate the COVID vaccine for employees?

As we’ve talked to health system executives about the challenges of rolling out COVID vaccines in their communities, one topic keeps coming up: how difficult it’s been to get hospitals’ own workers fully vaccinated. One system told us recently that only 55 percent of their frontline caregivers have opted to get vaccinated, despite early and easy availability, and ongoing encouragement from the hospital’s leaders.
Healthcare workers, it turns out, are just like the general population, bringing the same diversity of perspectives and concerns about vaccination to work with them from their own communities. Vaccine hesitancy is not a new issue for hospital staffers; getting the workforce to take the flu vaccine is an annual struggle for many hospitals.
But given the risks of COVID-19, why not just mandate that hospital employees get the vaccine, as other employers have started to do? We commonly hear two concerns.
One is a labor relations worry: will mandating vaccination cause workers to quit, or make it harder to hire staff in an already difficult market for talent? And given growing concerns about unionization of healthcare workers, will mandatory vaccination become a flashpoint issue?
The second concern is medical liability: can we force workers to get a vaccine that hasn’t been fully approved by the FDA? Would that expose the hospital to legal challenges down the road, if there turn out to be long-term complications from the vaccine?
Our own view is that the first concern is overblown—we suspect vaccine mandates are going to become more and more common as the economy reopens. As to the second, we’re more sympathetic. But once the FDA does grant full approval for the vaccines, we’d hope hospitals will get tougher about vaccine mandates (with the necessary exemptions for health, religious, and other concerns).
At the end of the day, hospitals are in the patient care business, and they should view vaccine mandates—whether for COVID or for influenza—as a patient safety issue, not a workforce engagement issue.
Hospital volume continues an uneven recovery

Though consumers say they’re increasingly confident in returning to healthcare settings, hospital volume is not returning with the same momentum across the board. Using the most recent data from analytics firm Strata Decision Technology, covering the first quarter of this year, the graphic above shows that observation, inpatient, and emergency department volumes all remain below pre-COVID levels.
Consumers are still most wary about returning to the emergency department, with volume down nearly 20 percent across the past year. Meanwhile, hospital outpatient visits rebounded quickly, and have been growing steadily month over month, finishing March 2021 at 36 percent above the 2019 level.
Meanwhile, a recent report from the Commonwealth Fund shows that no ambulatory specialty fully made up for the COVID volume hit by the end of last year. But some areas, including rheumatology, urology, and adult primary care, have bounced back faster than others.
With continued success in rolling out vaccines and reducing COVID cases, we’d expect a continued recovery of most hospital visit volume. It may be, however, that some areas, such as the emergency department, will never fully recover to pre-COVID levels. To the extent those visits are now being replaced by more appropriate telemedicine and urgent care utilization, that’s welcome news.
But the continued lag of inpatient admissions indicates that some of the loss of emergency volume is more worrisome—warranting continued efforts on the part of providers to reassure patients it’s safe to use healthcare services. Stay tuned as our team continues to dig into this data.
Hospital giants bet big on hospital at home

This week Mayo Clinic and Kaiser Permanente announced a $100M joint investment in Boston-based Medically Home, a provider of virtual hospital solutions. Founded in 2016, Medically Home is one of a handful of companies that coordinate with hospitals and doctors to provide in-home clinician visits, round-the-clock communications and monitoring, and access to support services to enable hospital-level care in the home. While interest has surged during the pandemic, the first hospital at home programs launched in the 1990s, and the model has a proven track record of delivering care that is lower cost and clinically equivalent (or better), when compared to a traditional hospital admission.
A confluence of market forces has driven rapid expansion in the model across the past year. Health systems are increasingly looking to hospital at home to address emerging consumer demand for care outside the hospital, and achieve the longer-term goals of providing flexible, lower-cost acute care capacity. And payers are looking to add hospital at home capabilities to their growing virtual and home-based care platforms to manage acutely ill Medicare Advantage beneficiaries in a lower-cost care setting.
Early adopters estimate that as many as 30 percent of patients admitted to hospitals today could be candidates for treatment at home. The large infusion of funding from Kaiser and Mayo will enable Medically Home to scale across the US, and also provides an endorsement of, and commitment to, the care model from these respected systems, which may help convince physicians who remain skeptical.
Coupled with the Centers for Medicare & Medicaid Services’ waiver program, allowing payment for home-hospital care, this investment should drive a new wave of growth in the model—and will likely make hospital at home a routine part of the care options available to patients.
Missouri backtracks on Medicaid expansion
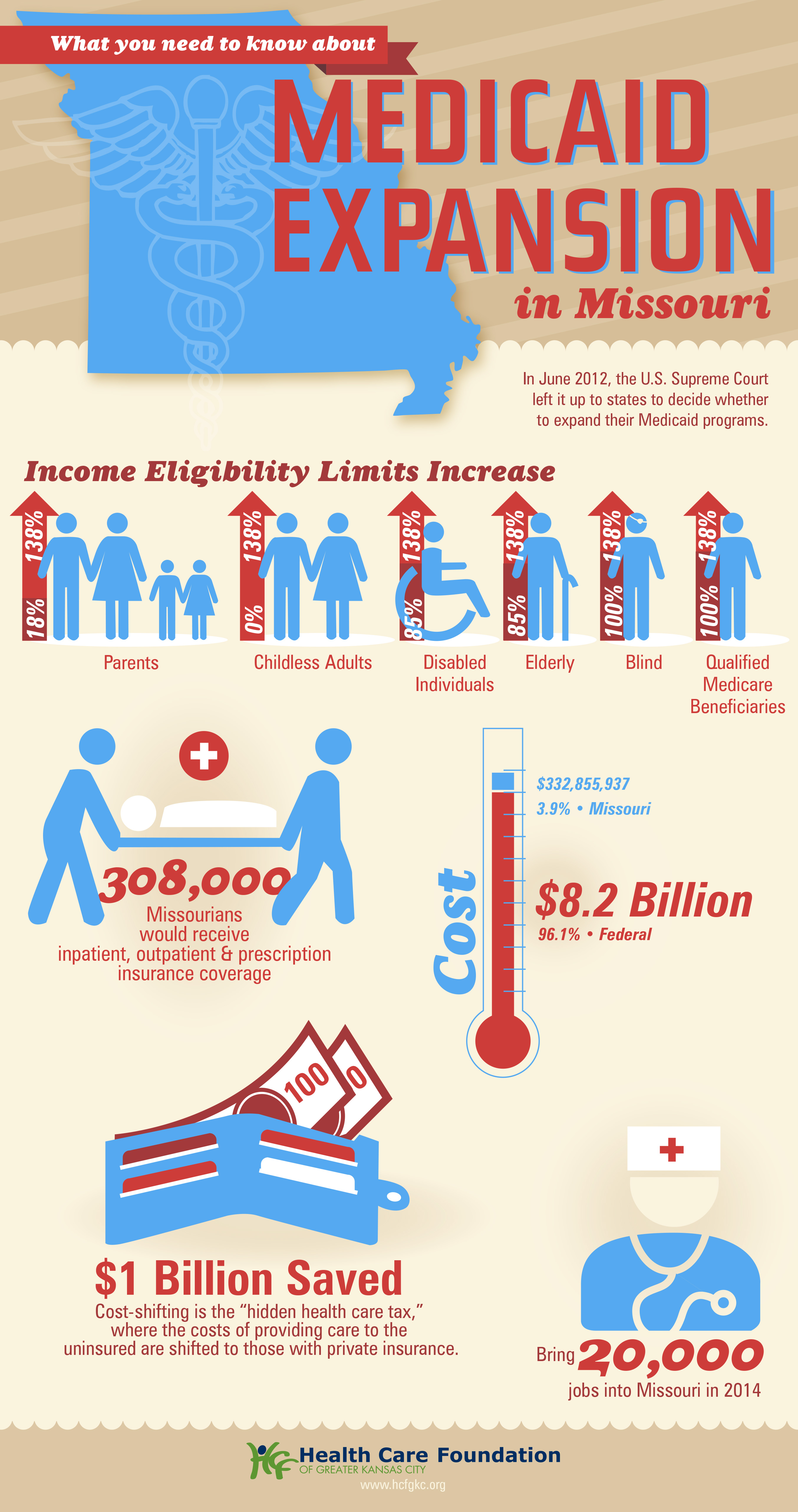
Missouri Gov. Mike Parson announced Thursday that his state would not expand Medicaid coverage to 275,000 residents who will become eligible on July 1st, despite a 2020 ballot initiative in which a majority of the state’s voters approved the expansion. Because the Missouri legislature has blocked funding for the expansion, Parson declared that the state’s Medicaid program, MO HealthNet, would run out of money if it moved forward.
The legislature’s decision to block funding was bolstered by an appeals court opinion last year, which challenged the expansion because the ballot initiative did not include a funding mechanism for widening coverage.
Under the Affordable Care Act (ACA), the federal government would have picked up 90 percent of the cost of expanding Medicaid in the state, in addition to boosting funding for existing Medicaid enrollees by 5 percent, thanks to a measure in the recent American Rescue Plan Act.
The governor’s decision leaves in place one of the strictest Medicaid eligibility standards in the nation: a family of three in Missouri must earn less than 21 percent of the federal poverty level—$5,400 per year—in order to qualify for coverage. The expansion measure would have opened the program to childless adults, and raised the eligibility limit to 138 percent of the federal poverty level.
The Missouri Hospital Association called the decision an “affront” to voters, pointing out that the state is currently running a budget surplus, and could easily allocate funds for the expansion. The status of Medicaid expansion in Missouri, which would become the 38th state to undertake expansion since the ACA’s passage, will ultimately be decided by court ruling, according to observers.
Meanwhile, like other states (mostly in the Southeast) that have resisted Medicaid expansion, Missouri will continue to see tax dollars flow out of the state to fund benefits in states that have expanded eligibility—despite the express will of voters. Given ample evidence that Medicaid expansion boosts access to care, health status, and health system sustainability, it’s nearly unfathomable that the politics of “Obamacare” continue to complicate the extension of this critical safety-net program.
The US Funded Universal Childcare During World War II—Then Stopped

Federally-subsidized childcare centers took care of an estimated 550,000 to 600,000 children while their mothers worked wartime jobs.
When the United States started recruiting women for World War II factory jobs, there was a reluctance to call stay-at-home mothers with young children into the workforce. That changed when the government realized it needed more wartime laborers in its factories. To allow more women to work, the government began subsidizing childcare for the first (and only) time in the nation’s history.
An estimated 550,000 to 600,000 children received care through these facilities, which cost parents around 50 to 75 cents per child, per day (in 2021, that’s less than $12). But like women’s employment in factories, the day care centers were always meant to be a temporary wartime measure. When the war ended, the government encouraged women to leave the factories and care for their children at home. Despite receiving letters and petitions urging the continuation of the childcare programs, the U.S. government stopped funding them in 1946.
Before World War II, organized “day care” didn’t really exist in the United States. The children of middle- and upper-class families might go to private nursery schools for a few hours a day, says Sonya Michel, a professor emerita of history, women’s studies and American studies at the University of Maryland-College Park and author of Children’s Interests/Mothers’ Rights: The Shaping of America’s Child Care Policy. (In German communities, five- and six-year-olds went to half-day Kindergartens.)
For children from poor families whose father had died or couldn’t work, there were day nurseries funded by charitable donations, Michel says. But there were no affordable all-day childcare centers for families in which both parents worked—a situation that was common for low-income families, particularly Black families, and less common for middle- and upper-class families.
The war temporarily changed that. In 1940, the United States passed the Defense Housing and Community Facilities and Services Act, known as the Lanham Act, which gave the Federal Works Agency the authority to fund the construction of houses, schools and other infrastructure for laborers in the growing defense industry. It was not specifically meant to fund childcare, but in late 1942, the government used it to fund temporary day care centers for the children of mothers working wartime jobs.
Communities had to apply for funding to set up day care centers; once they did, there was very little federal involvement. Local organizers structured childcare centers around a community’s needs. Many offered care at odd hours to accommodate the schedules of women who had to work early in the morning or late at night. They also provided up to three meals a day for children, with some offering prepared meals for mothers to take with them when they picked up their kids.
“The ones that we often hear about were the ‘model’ day nurseries that were set up at airplane factories [on the West coast],” says Michel. “Those were ones where the federal funding came very quickly, and some of the leading voices in the early childhood education movement…became quickly involved in setting [them] up,” she says.
For these centers, organizers enlisted architects to build attractive buildings that would cater to the needs of childcare, specifically. “There was a lot of publicity about those, but those were unusual. Most of the childcare centers were kind of makeshift. They were set up in church basements or garages.”
Though the quality of care varied by center, there hasn’t been much study of how this quality related to children’s race (in the Jim Crow South, where schools and recreational facilities were segregated, childcare centers were likely segregated too). At the same time, the United States was debuting subsidized childcare, it was also incarcerating Japanese American families in internment camps. So although these childcare facilities were groundbreaking, they didn’t serve all children.
Subsidized Childcare Ends When War Ends

When the World War II childcare centers first opened, many women were reluctant to hand their children over to them. According to Chris M. Herbst, a professor of public affairs at Arizona State University who has written about these programs in the Journal of Labor Economics, a lot of these women ended up having positive experiences.
“A couple of childcare programs in California surveyed the mothers of the kids in childcare as they were leaving childcare programs,” he says. “Although they were initially skeptical of this government-run childcare program and were worried about the developmental effects on their kids, the exit interviews revealed very, very high levels of parental satisfaction with the childcare programs.”
As the war ended in August 1945, the Federal Works Agency announced it would stop funding childcare as soon as possible. Parents responded by sending the agency 1,155 letters, 318 wires, 794 postcards and petitions with 3,647 signatures urging the government to keep them open. In response, the U.S. government provided additional funding for childcare through February 1946. After that, it was over.
Lobbying for national childcare gained momentum in the 1960s and ‘70s, a period when many of its advocates may have themselves gone to World War II day care as kids. In 1971, Congress passed the Comprehensive Child Development Act, which would have established nationally-funded, locally-administered childcare centers.
This was during the Cold War, a time when anti-childcare activists pointed to the fact that the Soviet Union funded childcare as an argument for why the United States shouldn’t. President Richard Nixon vetoed the bill, arguing that it would “commit the vast moral authority of the National Government to the side of communal approaches to child rearing over against the family-centered approach.”
In this case, “family-centered” meant the mother should care for the children at home while the father worked outside of it—regardless of whether this was something the parents could afford or desired to do. World War II remains the only time in U.S. history that the country came close to instituting universal childcare.
Cartoon – Gout Education

Gout can take a toll on not only health, but also on your wallet. Gout-related costs, on average, can be $12,000 per year. To minimize costs—and painful flares—make sure to get checked early and get uric acid levels checked once every six months. https://bit.ly/GoutCost
