
The U.S. economy added back the smallest number of jobs in seven months in November, as the labor market endured mounting pressure from the coronavirus pandemic while businesses wait for a vaccine to be distributed next year.
The U.S. Department of Labor released its monthly jobs report Friday morning at 8:30 a.m. ET. Here were the main results from the report, compared to Bloomberg consensus data as of Friday morning:
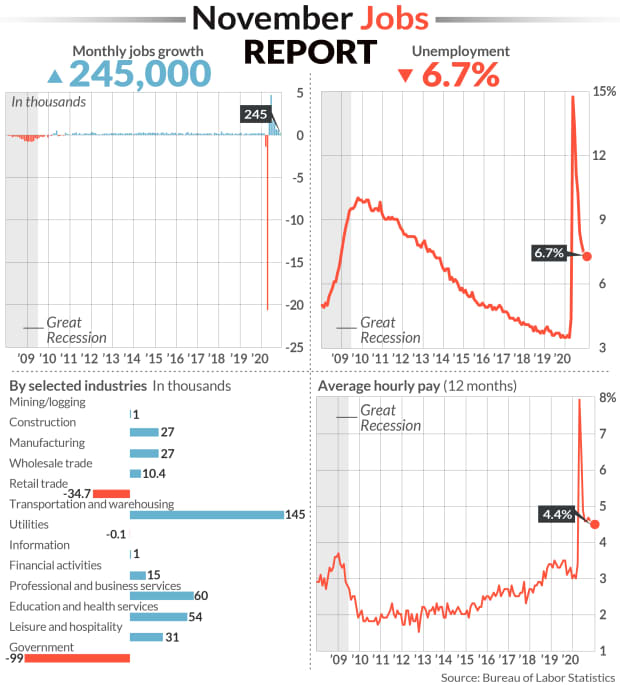
- Change in non-farm payrolls: +245,000 vs. +460,000 expected and a revised +610,000 in October
- Unemployment rate: 6.7% vs. 6.7% expected and 6.9% in October
- Average Hourly Earnings month-over-month: 0.3% vs. +0.1% expected and +0.1% in October
- Average Hourly Earnings year-over-year: 4.4% vs. +4.2% expected and a revised +4.4% in October
During November, a plethora of new stay-in-place measures and curfews swept the nation as COVID-19 cases, hospitalizations and deaths swelled to record levels. These renewed restrictions weighed on the rate of the recovery in the labor market, which had already been slowing after a record surge in rehiring followed the initial wave of lockdowns in the spring.
To that end, job gains in November sharply missed expectations. Non-farm payrolls grew by just 245,000 during the month for the smallest number since April’s record, virus-induced decline. October’s payroll gain was downwardly revised to 610,000 from the 638,000 reported earlier, while September’s gain was raised to 711,000 from 672,000.
A third straight month of declining government employment served as a drag on the headline payrolls figure, as another 93,000 temporary workers hired for the 2020 Census were let go.
In the private sector, retail trade industries shed nearly 35,000 jobs following a gain of 95,000 in October. Leisure and hospitality employers added just 31,000 jobs during November, declining by nearly 90% from October. And in goods-producing industries, manufacturing jobs rose by only 27,000 for the month, falling short of the 40,000 expected.
But a handful of other industries added more jobs in November from October: Transportation and warehousing jobs grew by 145,000 to more than double October’s advance, and growth in wholesale trade positions also doubled to 10,400.
November’s unemployment rate also improved just marginally to 6.7% from the 6.9% reported in October. While down from a pandemic-era high of 14.7% in April, the jobless rate remains nearly double that from before the pandemic.
Other employment reports this week underscored the decelerating trend. Private-sector hiring fell to the lowest level in four months in November, according to data tracked by ADP. New weekly jobless claims began rising again around the 12th of the month, when the Labor Department conducts its surveys for its monthly jobs report. And in the Federal Reserve’s November Beige Book, the central bank noted that nearly all districts reported rising employment, “but for most, the pace was slow, at best, and the recovery remained incomplete.”
The U.S. economy still has a ways to go before fully making up for the drop in payrolls induced by the pandemic. Even with a seventh straight month of net job gains, the economy remains about 9.8 million jobs short of its pre-pandemic level in February. The U.S. economy lost more than 22 million jobs between March and April.
And worryingly, the number of the long-term unemployed has kept climbing. Those classified as “permanent job losers” totaled 3.7 million in November, eclipsing the number of individuals on temporary layoff for the second time since the start of the pandemic. Permanent job losers have increased by 2.5 million since February, before the pandemic meaningfully hit the U.S. economy.
In Washington, congressional lawmakers have for months been at a stalemate over the size and scope of another stimulus package, which could help provide funds for businesses to help keep workers employed, and offer extended unemployment benefits for those the pandemic has kept out of work. Federal unemployment programs authorized under the CARES Act in the spring are poised to expire at the end of the month. These include the Pandemic Emergency Unemployment Compensation and Pandemic Unemployment Assistance programs, which together provide benefits for more than 13 million Americans.
“The only thing that matters about today’s NFP [non-farm payrolls] report is whether it increases the likelihood of a stimulus deal getting done during the lame duck session,” Peter Tchir, head of macro strategy for Academy Securities, said in an email Friday morning. “While the unemployment rate shrunk and wages ticked up nicely, the headline number dropped significantly, was well below average expectations, and included some downward revisions to last month (and upward revisions to 2 months ago) – all of which point to a less robust job market.”









{kind=link}