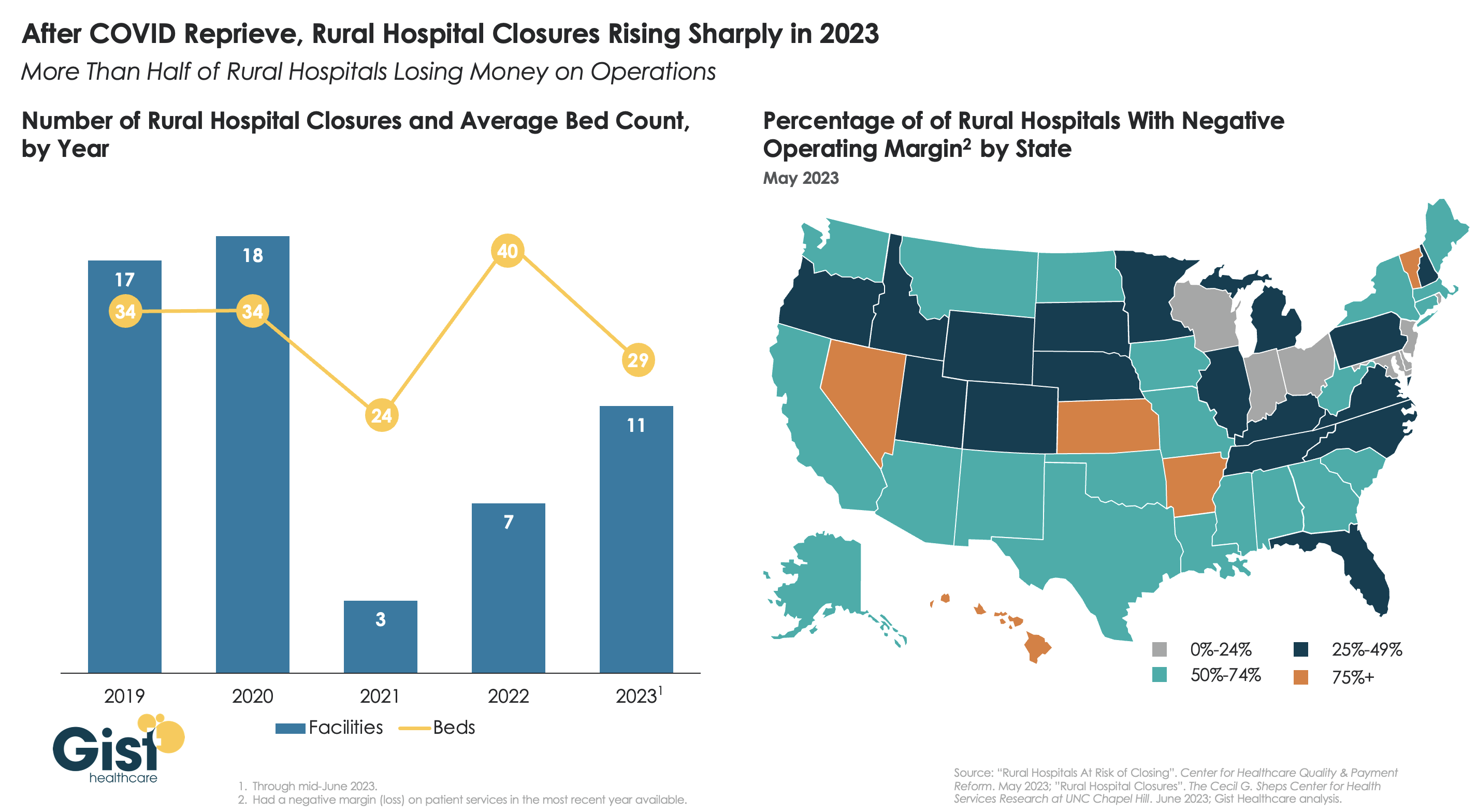
After a brief reprieve thanks to COVID relief funds, rural hospital closures are once again on the rise, with 11 facilities already closing in the first half of this year.
More rural facilities have already closed in 2023 than the previous two years combined, and this year is on pace to be the second-highest number of rural hospital beds lost since 2005.
And the majority of rural hospitals that haven’t closed are experiencing negative operating margins, with almost one in three at immediate or high risk of closure due to declining volumes, shifting payer mix, and increased labor and supply costs.
Leaders at rural hospitals now face difficult decisions including drastically cutting services, merging with a larger system, or closing their doors altogether. The Centers for Medicare and Medicaid Services (CMS) launched the Rural Emergency Hospital Program recently, designed to financially support small rural hospitals that convert to providing emergency services only, but so far program uptake has been limited.
While efforts to prop up hospitals will help to sustain access to care in the near term, rural communities ultimately need a new model for care, with reimagined facilities, supported by enhanced virtual connections to specialists and higher-acuity services.
Physician income has not kept pace with inflation and administrative costs prompting 70% to leave private practice. Half are now employed by hospitals and another 20% by private equity-backed practice managers. Both trends began before the pandemic in response to tougher financial conditions for physicians across all specialties. While hospitals held their own at the sector level, physicians lost ground. Per CMS’ NHE analysis, from 2000 to 2021:
Spending in hospitals increased from 30.4% of total spending to 31.4%
Spending for prescription drugs was essentially unchanged from 8.95% to8.88%
Public health spending. increased slightly from 3.2% of total spending to 4.4%.
But spending for physician services shrank from 21.1% to 15.6%.
In tandem with the erosion of finances for medical practices, investments in medical practices by private equity grew. Per Pitchbook, there have been 874 practice acquisitions by PE/Venture backed sponsors in the last 12 years with 20 in the first half of this year alone. Most of these are small ($7.53 million/transaction) and most involve a tuck-in to an existing PE backed platform (i.e., Privia, Sheridan, et al). Rightfully, physicians point out that while hospitals and drug companies have protected their piece of the health care pie successfully for 20 years while physicians have lost ground.
Physicians are not happy and burnout is pervasive. The employment of physicians in hospital and private equity settings has not made life happier for physicians. Per Medscape’s most recent assessment, burnout increased to 53% in 2022–up from 47% in 2021 and 26% since 2018. More than one in five physicians (22%) reported experiencing depression—up from 15% since 2018. They’re anxious about the future and increasingly sensitive to compensation comparisons with professions that require less training and earn more. They’re suspicious of consultants, lawyers and bankers whose experience is limited but fees inexplicably high They’re incensed by executive compensation in hospitals, drug companies, and health insurer settings they deem overpaid and overhyped. And they resent execs in for-profit and private equity companies who achieve astronomical wealth via their stock-option packages earned on the backs of the physicians they control.
The realities are these:
Physicians lack a strong voice. The American Medical Association’s membership includes less than a third of active-practice physicians. It is increasingly under-fire for under-representing primary and preventive health providers in its government-authorized monopoly on coding, its lobbying efforts against scope of practice expansion for APNs and pharmacists, its opposition to medical training innovations that could significantly improve the readiness and effectiveness of the physician workforce and more. The AMA’s influence is strong on a shrinking number of issues and increasingly resonate out of touch on issues that resonate with voters and lawmakers (expanded scope of practice for nurses and pharmacists, price and outcome transparency, et al).
Physicians operate in a buyers’ market but behave like it’s a sellers’ market. Physicians are trained to think of themselves as the hub of a system in which what they say determines what everyone else does…including patients. They are conditioned in medical school, residency and practice to be self-centered and resist efforts via data, clinical practice redesign or even “value-based incentives” to change their behaviors. They despise the notions of price transparency, cost effectiveness and outcome-based comparisons to their peers while calling for more accountability from hospitals, insurers and drug companies. They discount notions of consumerism and self-care and believe report cards over-rate patient experiences since medical practice is uniquely complicated.
Most live in a buyers’ market mentality unwilling/unable to see the sellers’ market healthcare has become. Otherwise, price transparency would be prevalent, operating hours and support services more conducive to the needs of patients and digital investments to maintain connectivity significant…but most don’t.
My take:
The U.S. economy will be testy for the 12 months: bringing down inflation will require interest rate hikes. Unemployment will increase slightly, wage inflation will slow, and the 2024 election cycle will draw unwelcome attention to healthcare spending and its affordability as root causes of growing financial insecurity in American households.
Given this backdrop, the profession of medicine faces a tipping point: become an integral part of the system’s solution or a vestige of its past. That solution should address medicine’s role in…
Addressing affordability for households and patients and the direct role it plays.
Integrating generative AI into more accurate diagnostics and more accessible, efficient treatment methods.
Embracing transparency about medical services pricing, costs, outcomes, business relationships and conflicts of interest.
Creating care plans around individualized social determinants of health and distinctions in populations.
Streamlining medical training toward competency-based lifelong learning, data-driven technology support, a team-based delivery and ‘whole person’ orientation to individuals.
Accepting full accountability for their effectiveness in reducing unnecessary costs and spending, increasing equitable access and engaging consumers in self-care.
How value-based and alternative payment models figure into this is anyone’s guess. Some physician organizations (AAPG, NAACO, et al) are all-in for expansion of these while others note their lackluster results to date. And physician calls for a replacement to RVU-based conversion-factor will grow louder as Congress revisits MACRA and how Medicare pays physicians.
These are important and require urgent attention, but they do not elevate the profession to its rightful place at the center of system transformation.
I hold the profession of medicine in high regard. I respect and trust my physicians—Ben, Ben and Blake are trusted friends in my personal journey to health. But their profession as a whole appears stuck in the past and unable to play a central role in the health system transformation. Until and unless new physician leaders with fresh thinking about the entire system step up, the profession’s role will continue to erode.
Playing the victim card and blame game against Medicare, hospitals, insurers, drug companies and everyone else they deem unworthy will not solve the health system’s problems.
I believe conditions are right for physicians to seize the moral high ground and lead the needed reset of the health system but most aren’t ready.
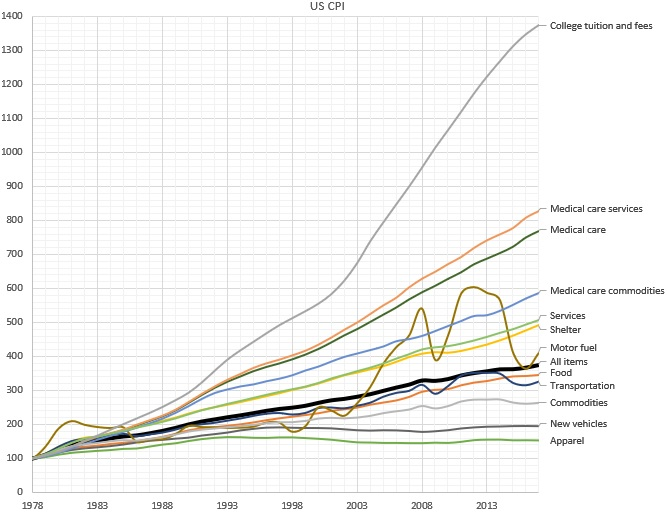
Why does the cost of education and healthcare services continue to rise rapidly, while the cost of goods rise much more slowly? According to economics theory, wages rise when there’s greater productivity; but a rise without an increase in productivity is referred to as “Baumol’s Cost Disease” . In an original study first published in 1966, economist William J. Baumol used the example of a string quartet to illustrate this idea: While the productivity of a given quartet has not increased over time over the last two hundred years, the salary (in nominal and real terms) has increased dramatically.
One way out of this trap is to turn services into goods. Employing a cobbler to make a pair of custom shoes, for instance, is expensive, so we buy factory made shoes: shoes as a good instead of as a service. In doing so, we accept some limitations: a finite set of styles and sizes to choose from; perhaps a less-than-perfect fit for each individual foot; limited styles and customizations — but with the positive trade off in favor of greatly decreased cost. In much the same way, we consume the “good” of the string quartet in the form of a digital recording of a musical piece, instead of the “service” of a live performance. In short, turning services into goods industrializes the process, increasing efficiency and reducing cost.
But is this seemingly alchemical transformation possible in healthcare?
Until today, it’s essentially been accepted as a given that this cost “disease” is incurable where there’s the need for professional, highly trained people performing services — industries like healthcare, education — and therefore drives some of the biggest cost crises of our day, that affect many people in countless ways.
To cure Baumol’s cost disease, we would have to transform the industry’s professional human labor into something that can be manufactured, commoditized, industrialized, and automated. While this has long been an issue in healthcare, for many good and bad reasons, the cure involves bringing more artificial intelligence (AI) to the industry. AI creates a new opportunity: to transform services into goods.
It’s no magic bullet for sure; even our own a16z partners Martin Casado and Matt Bornstein have argued that in enterprise companies, this won’t work, and that AI in this case effectively just replaces human services with different human services with few gains, given all the data cleanup and edge cases involved. But in healthcare, unlike in other industries — like social media content analysis, or self-driving cars — the kind of data labelling needed is actually already an intrinsic part of the healthcare system. In much the same way it is an intrinsic part of Google search — where people choose the most relevant link in the search results, and Google’s AI learns from this, improving with each search — whenever a doctor diagnoses a condition, prescribes a mediation, or interprets an x-ray, that information is then encoded into the electronic health record (EHR). Or, it’s in revenue cycle management — how all bills are paid in healthcare — where people currently perform the manual tasks of identifying what is billable, and to whom. Using AI to learn from these coders (the way, for example, Alpha Health does) means the human work — human labeling — is “free”, since it’s part of what we’re doing anyway.
What’s more, the data is high quality, because when all the doctors in the system are labellers, AI ensures every doctor has the very best teachers in the world — no single doctor alone could ever have that roster of mentors. Training is done on all patients, AI learns from everything, and everybody… and then outputs the results back out to everyone.
Of course, it’s not a total walk in the park; work needs to be done to integrate this data into the system. One you solve data labelling, you have to train with those labels. Data labelling is just one of the reasons AI based businesses are perceived to have low margins (often requiring an enormous amount of GPU or CPU time, and at great expense. But human training is also expensive: training must often be customized to individuals, and often needs to be redone as employees churn. Because computers are identical, training AI has no such challenges. If you compare the cost of AI training to the cost of executing a simple algorithm,AI training is expensive. If you compare the cost of AI training to the cost of human training, AI is cheap. And, AI training gets exponentially cheaper over time, because of Moore’s Law’s profoundly powerful compounding effects. So even if using AI is at cost parity with a service solution now, the eventual win is obvious. And to some degree, we can commoditize the AI itself as well, for more efficiency, by keeping customization low and training rare with AI.
Another complaint about AI’s ability to transform services into goods is what’s referred to as the “long tail of tasks.” This is the idea that AI won’t be useful if it can only perform a small fraction of what humans can. But in healthcare, even a small fraction of that long tail can have enormous impact. With the right, highly efficient training and labeling, AI can transform perhaps 5% of the human labor of analyzing bills and claims to automate from services to goods. By using AI to learn from medical billing — even just by triaging the “easy” and mundane cases (and escalating the “long tail” of more complex tasks to people as needed) — can bring a dramatic cost savings. Not to mention allowing people to focus on the more higher order aspects of the job, allowing them to deliver better results and service.
We’ve been waiting decades — maybe even centuries — for the ability to reverse Baumol’s Cost Disease in our most service-heavy, yet most critical, industries, such as healthcare.
The transformation of services into goods won’t occur overnight. But Baumol himself couldn’t have foreseen the revolution that AI is creating, any more than someone in the Renaissance anticipating a shoe factory and Moore’s Law since. If applied in the right places, with the right conditions, taking into account the hard realities of the healthcare system, AI can be a vastly powerful lever to pull. We may not cure Baumol’s Cost Disease overnight, but even a small gain in cost and time savings would have huge impacts in healthcare.
At the end of a meeting last week with a health system executive team, the system’s COO asked us a question: “Your concept of a consumer-focused health system centered around treating patients as members describes exactly how we want to relate to our patients, but we’re not sure about the timing. Could you give us a list of the ‘no regrets’ investments you’d recommend for health systems looking to do this?”
We frequently get asked about “no regrets” strategies:
decisions or investments that will be accretive in both the current fee-for-service system as well as a future payment and operational model oriented around consumer value. The idea is understandably appealing for systems concerned about changing their delivery model too quickly in advance of payment change. And there is a long list of strategies that would make a system stronger in both fee-for-service and value: cost reduction, value-driven referral management, and online scheduling, just to name a few.
But as we pointed out, the decision to pursue only the no-regrets moves is a clear signal that the organization’s strategy is still tied to the current payment model.
If the system is truly ready to change, strategy development should start with identifying the most important investments for delivering consumer value. It’s fine to acknowledge that a health system is not yet ready, but we cautioned the team that they should not rely on the external market to provide signals for when they should undertake real change in strategy.
External signals—from payers, competitors, or disruptors—will come too slowly, or perhaps never. At some point, the health system should be prepared to lead innovation, introduce a new model of value to the market, and define and promote the incentives to support it.
Real change will require disruption of parts of the current business and cannot be accomplished with “no-regrets investments” alone.
American Hospitals is the fourth in a series of documentaries produced by the Unfinished Business Foundation, founded by Richard Master, CEO of MCS Industries Inc., who took a deep dive into the economics of the U.S. health-care system after his company was hit year after year with double-digit health insurance rate increases.
Master teamed up with filmmaker Vincent Mondillo to produce Fix It: Healthcare at the Tipping Point; Big Pharma: Market Failure; Big Money Agenda: Democracy on the Brink, and now, American Hospitals.
A provocative look at the cost and inequities of American Hospitals, often more motivated by money and power than in providing for the health needs of individuals and the communities they were founded to serve. From the filmmakers behind the hit documentaries Fix It: Healthcare at the Tipping Point, Big Money Agenda, and Big Pharma.
Learn more and find out where to see the latest film at fixithealthcare.com/events
After 18 years as CEO in Kaiser Permanente, I set my sights on improving the heatlh of the nation, hoping to find a way to achieve the same quality, technology and affordability our medical group delivered to 5 million patients on both coasts.
That quest launched the Fixing Healthcare podcast in 2018, and it inspired interviews with dozens of leaders, thinkers and doers, both in and around medicine. These experts shared innovative ideas and proven solutions for achieving (a) superior quality, (b) improved patient access, (c) lower overall costs, and (d) greater patient and clinician satisfaction.
Which of the hundreds of ideas presented remain most promising?
Why, after five years and so many excellent solutions, has our nation experienced such limited improvements in healthcare?
And finally, how will these great ideas become reality?
To answer the first question, I offer 15 of the best Fixing Healthcare recommendations so far. Some quotes have been modified for clarity with links to all original episodes (and transcripts) included.
Fixing the business of medicine
1. Malcolm Gladwell, journalist and five-time bestselling author: “In other professions, when people break rules and bring greater economic efficiency or value, we reward them. In medicine, we need to demonstrate a consistent pattern of rewarding the person who does things better.”
2. Richard Pollack, CEO of the American Hospital Association (AHA): “I hope in 10 years we have more integrated delivery systems providing care, not bouncing people around from one unconnected facility to the next. I would hope that we’re in a position where there’s a real focus on ensuring that people get care in a very convenient way.”
Eliminating burnout
3. Zubin Damania, aka ZDoggMD, hospitalist and healthcare satirist: “In the culture of medicine, specialists view primary care as the weak medical students, the people who couldn’t get the board scores or rotation honors to become a specialist. Because why would you do primary care? It’s miserable. You don’t get paid enough. It’s drudgery. We must change these perceptions.”
4. Devi Shetty, India’s leading heart surgeon and founder of Narayana Health: “When you strive to work for a purpose, which is not about profiting yourself, the purpose of our action is to help society, mankind on a large scale. When that happens, cosmic forces ensure that all the required components come in place and your dream becomes a reality.”
5. Jonathan Fisher, cardiologist and clinician advocate: “The problem we’re facing in healthcare is that clinicians are all siloed. We may be siloed in our own institution thinking that we’re doing it best. We may be siloed in our own specialty thinking that we’re better than others. All of these divides need to be bridged. We need to begin the bridging.”
Making medicine equitable
6. Jen Gunter, women’s health advocate and “the internet’s OB-GYN”: “Women are not listened to by doctors in the way that men are. They have a harder time navigating the system because of that. Many times, they’re told their pain isn’t that serious or their bleeding isn’t that heavy. We must do better at teaching women’s health in medicine.”
7. Amanda Calhoun, activist, researcher and anti-racism educator: “A 2015 survey showed that white residents and medical students still thought Black people feel less pain, which is wild to me because Black is a race. It’s not biological. This is actually an historical belief that persists. One of the biggest things we can do as the medical system is work on rebuilding trust with the Black community.”
Addressing social determinants of health
8. Don Berwick, former CMS administrator and head of 100,000 Lives campaign: “We know where the money should go if we really want to be a healthy nation: early childhood development, workplaces that thrive, support to the lonely, to elders, to community infrastructures like food security and transportation security and housing security, to anti-racism and criminal-justice reform. But we starve the infrastructures that could produce health to support the massive architecture of intervention.”
9. David T. Feinberg, chairman of Oracle Health: “Twenty percent of whether we live or die, whether we have life in our years and years in our life, is based on going to good doctors and good hospitals. We should put the majority of effort on the stuff that really impacts your health: your genetic code, your zip code, your social environment, your access to clean food, your access to transportation, how much loneliness you have or don’t have.”
Empowering patients
10. Elisabeth Rosenthal, physician, author and editor-in-chief of KHN: “To patients, I say write about your surprise medical bills. Write to a journalist, write to your local newspaper. Hospitals today are very sensitive about their reputations and they do not want to be shamed by some of these charges.”
11. Gordon Chen, ChenMed CMO: “If you think about what leadership really is, it’s influence. Nothing more, nothing less. And the only way to achieve better health in patients is to get them to change their behaviors in a positive way. That behavior change takes influence. It requires primary care physicians to build relationship and earn trust with patients. That is how both doctors and patients can drive better health outcomes.”
Utilizing technology
12. Vinod Khosla, entrepreneur, investor, technologist: “The most expensive part of the U.S. healthcare system is expertise, and expertise can relatively be tamed with technology and AI. We can capture some of that expertise, so each oncologist can do 10 times more patient care than they would on their own without that help.”
13. Rod Rohrich, influential plastic surgeon and social media proponent: “Doctors, use social media to empower your audience, to educate them, and not to overwhelm them. If you approach social media by educating patients about their own health, how they can be better, how can they do things better, how they can find doctors better, that’s a good thing.”
Rethinking medical education
14. Marty Makary, surgeon and public policy researcher: “I would get rid of all the useless sh*t we teach our medical students and residents and fellows. In the 16 years of education that I went through, I learned stuff that has nothing to do with patient care, stuff that nobody needs to memorize.”
15. Eric Topol, cardiologist, scientist and AI expert: “It’s pretty embarrassing. If you go across 150 medical schools, not one has AI as a core curriculum. Patients will get well versed in AI. It’s important that physicians stay ahead, as well.”
Great ideas, but little progress
Since 2018, our nation has spent $20 trillion on medical care, navigated the largest global pandemic in a century and developed an effective mRNA vaccine, nearly from scratch. And yet, despite all this spending and scientific innovation, American medicine has lost ground.
American life expectancy has dropped while maternal mortality rates have worsened. Clinician burnout has accelerated amid a growing shortage of primary care and emergency medicine physicians. And compared to 12 of its wealthiest global peers, the United States spends nearly twice as much per person on medical care, but ranks last in clinical outcomes.
Guests on Fixing Healthcare generally agree on the causes of stagnating national progress.
Healthcare system giants, including those in the drug, insurance and hospital industries, find it easier to drive up prices than to prevent disease or make care-delivery more efficient. Over the past decade, they’ve formed a conglomerate of monopolies that prosper from the existing rules, leaving them little incentive to innovate on behalf of patients. And in this era of deep partisan divide, meaningful healthcare reforms have not (and won’t) come from Congress.
Then who will lead the way?
Industry change never happens because it should. It happens when demand and opportunity collide, creating space for new entrants and outsiders to push past the established incumbents. In healthcare, I see two possibilities:
1. Providers will rally and reform healthcare
Doctors and hospitals are struggling. They’re struggling with declining morale and decreasing revenue. Clinicians are exiting the profession and hospitals are shuttering their doors. As the pain intensifies, medical group leaders may be the ones who decide to begin the process of change.
The first step would be to demand payment reform.
Today’s reimbursement model, fee-for-service, pays doctors and hospitals based on the quantity of care they provide—not the quality of care. This methodology pushes physicians to see more patients, spend less time with them, and perform ever-more administrative (billing) tasks. Physicians liken it to being in a hamster wheel: running faster and faster just to stay in place.
Instead, providers of care could be paid by insurers, the government and self-funded businesses directly, through a model called “capitation.” With capitation, groups of providers receive a fixed amount of money per year. That sum depends on the number of enrollees they care for and the amount of care those individuals are expected to need based on their age and underlying diseases.
This model puts most of the financial risk on providers, encouraging them to deliver high-quality, effective medical care. With capitation, doctors and hospitals have strong financial incentives to prevent illnesses through timely and recommended preventive screenings and a focus on lifestyle-medicine (which includes diet, exercise and stress reduction). They’re rewarded for managing patients’ health and helping them avoid costly complications from chronic diseases, such as heart attacks, strokes and cancer.
Capitation encourages doctors from all specialties to collaborate and work together on behalf of patients, thus reducing the isolation physicians experience while ensuring fewer patients fall through the cracks of our dysfunctional healthcare system. The payment methodology aligns the needs of patients with the interests of providers, which has the power to restore the sense of mission and purpose medicine has lost.
Capitation at the delivery-system level eliminates the need for prior authorization from insurers (a key cause of clinician burnout) and elevates the esteem accorded to primary care doctors (who focus on disease prevention and care coordination). And because the financial benefits are tied to better health outcomes, the capitated model rewards clinicians who eliminate racial and gender disparities in medical care and organizations that take steps to address the social determinants of health.
2. Major retailers will take over
If clinicians don’t lead the way, corporate behemoths like Amazon, CVS and Walmart will disrupt the healthcare system as we know it. These retailers are acquiring the insurance, pharmacy and direct-patient-care pieces needed to squeeze out the incumbents and take over American healthcare.
Each is investing in new ways to empower patients, provide in-home care and radically improve access to both in-person and virtual medicine. Once generative AI solutions like ChatGPT gain enough computing power and users, tech-savvy retailers will apply this tool to monitor patients, enable healthier lifestyles and improve the quality of medical care compared to today.
When Fixing Healthcare debuted five years ago, none of the show’s guests could have foreseen a pandemic that left more than a million dead. But, had our nation embraced their ideas from the outset, many of those lives would have been saved. The pandemic rocked an already unstable and underperforming healthcare system. Our nation’s failure to prevent and control chronic disease resulted in hundreds of thousands of unnecessary deaths from Covid-19. Outdated information technology systems, medical errors and disparities in care caused hundreds of thousands more. As a nation, we could have done much better.
With the cracks in the system widening and the foundation eroding, disruption in healthcare is inevitable. What remains to be seen is whether it will come from inside or outside the U.S. healthcare system.
Welcome to the “Lessons from the C-suite” series, featuring Advisory Board President Eric Larsen’s conversations with the most influential leaders in healthcare.
In this edition, Bill Gassen, President and CEO of Sanford Health and James Hereford, President and CEO of Fairview Health Services talk with Eric about the planned merger that will create the 11th largest health system in the United States that would span North Dakota, South Dakota, Iowa, and Minnesota.
The two CEOs describe the urgency and intent behind the merger, why not all disruptors are equally disruptive, and why it takes more than size to harness scale in healthcare.
Question: Bill and James, let’s jump right in. The two of you are architecting one of the most significant health system mergers of 2023 — a combination of Sanford Health and Fairview, which on its completion, will result in the 11th largest health system in the US. The discussions have attracted, understandably, a lot of interest and scrutiny not just in each of your communities, but nationally. Some may not be aware, but this is not the first time that Sanford and Fairview have considered coming together. Bill, let’s start with you – why is this time different?
Gassen: Eric, you’re right. This is not the only time our two organizations have considered the idea of merging. James and I, and our respective boards and organizations, have examined every element of the union and are confident that this is the right time to proceed. We have executed a Letter of Intent (LOI) and submitted an HSR filing that has been reviewed by the Federal Trade Commission (FTC). The parties provided substantial amounts of information to the FTC and the HSR process and it is now complete. There is an unwavering commitment from our respective leaders and our organizations to see this through.
It is a false choice for anyone to believe that James or I or anybody else has the benefit of sitting back and saying, well, maybe I’ll just maintain the world that I live in today. The healthcare status quo is gone. What is in front of us is taking the steps needed to ensure that we can continue to provide the best possible service for our patients, employees, and communities. Taking control over our destiny. We want to come together in a merger between our two organizations to put us in a position to fundamentally change and to be an agent for the modernization of the way care is delivered into the future. Our organizations exist only to serve patients, employees, and our communities. That is not up for debate. What we have in front of us is a decision to make that better for generations to come.
Hereford: I think Bill articulated that very well. Our purpose is to combine to improve and sustain our ability to offer world class healthcare. It is not simply a function of scale, you have to combine that with an intent to drive change, to improve value, and to innovate. And that’s a rare thing to have that intent. We have that intent today.
Avoiding the ‘Noah’s Ark’ problem
Q: Let’s go a bit deeper into the horizontal consolidation among health systems. This isn’t a new phenomenon — in fact, our $1.4 trillion hospital sector is already massively consolidated, with the top 100 systems controlling almost $900 billion in revenue. But with this degree of concentration, a lot of disillusionment: we just haven’t seen compelling or provable quality improvements, let alone the scale of cost reductions projected. Some of this might be what I call the “Noah’s Ark” problem—two of everything (two CEOs, two headquarters, two EHRs, etc.) … in other words, very little rationalization of back-office infrastructure or staffing.
I think about the proposed Sanford-Fairview merger differently. I might even characterize it as more a “vertical” merger, instead of “horizontal” — a combination of different and complementary capabilities instead of overlapping or competing ones — including Sanford’s proprietary health plan and virtual hospital investments, bringing Fairview’s specialty pharmacy and post-acute companies into the combination — for example. Am I thinking about this the right way?
Gassen: I think your characterization is right, Eric. We are different but very complementary organizations. We are contiguous as it relates to geography, but there is no overlap. We serve distinctly different populations in a similar part of the country. Roughly two-thirds of the patients who have been served today at Sanford Health come to us from a rural community. While most of those who Fairview serves come from much more densely populated urban communities. Both of those subsets of our population are experiencing similar challenges. There’s a need for financial sustainability, both on the provider side as well as on the patient side of the house.
When you think about our service mix, there are a number of complementary areas that make our union additive. Specialty and subspecialty expertise at Fairview coupled with a robust primary care backbone from Sanford plus our Virtual Care initiative and significant philanthropic investment will come together to create powerful healthcare solutions.
The fact that at Sanford alone we have $350 million solely dedicated to, and available for, scaling virtual care is amazing. And when you think about applying that investment to Sanford and Fairview, the opportunities are limitless. We’re going to be able to serve both our rural and urban communities, allowing us to truly transform the way in which healthcare is delivered and experienced in this part of the country.
And for those outside our orbit, they’ll say, “I want to partner with a combined Sanford Fairview” because that is much more attractive. And at the end of the day, partnering with us means that we’re all in a better position to transform the way in which we deliver care, how care is accessed, and how quality is improved. And do it in a financially sustainable way that allows us to deliver equitable care to more people in the upper Midwest.
Hereford: Here’s why scale matters: If you’re one hospital and you drive an innovation that requires a capital of investment of $1 million, that’s an expensive solution. But if you’ve got 100 hospitals, the size of that investment you made on a scale basis is much smaller. Therefore, your ability to drive the needed level of innovation is expanded significantly. To truly improve healthcare delivery, we must challenge ourselves to do things differently, but you have to have a certain level of scale to be able to do that.
Health system transformation must happen now
Q:I want to expand on the earlier point you made that the old health system status quo is forever gone. 2022, for health systems, was something of an Armageddon year — the worst on record with 11 out of 12 months with negative margins; supply chain costs up 17% versus pre-pandemic; health systems collectively spending an extra $125 billion on Labor last year compared to 2021. So not a great “state of the union” for acute-care centric health systems. How does this macroeconomic backdrop factor into your planning?
Hereford: Conceptually, cognitively, I would offer that hospital CEOs probably all know that the good old days are gone. But you don’t see organizations responding as if they’re gone. And we’re on the precipice of a significant cliff. The fundamental things that have defined healthcare and not-for-profit healthcare for decades have fundamentally shifted. We need to change in response.
We’re going to have 80,000 people when we combine. The challenge for us as leaders is going to be how do we shift the mindset and change the way we think about care delivery while maintaining essential services that persist with challenging economics. We are a high capital, low margin business that is critical to society.
Gassen: James, it’s as you and I talk about a lot. We don’t get the benefit of hitting pause, taking a year to revamp the industry because it’s 24 by 7 by 365. There are no breaks.
And while we’re doing that and while we are delivering essential services, the 45,000 incredible caregivers at Sanford and the 35,000 incredible caregivers at Fairview, collectively, are going to figure out how we evolve together as a unified organization to continue to elevate that critical work of patient care. And we don’t get reimbursed for a lot of those services. But those are essential services that people need.
If we want to be able to meet the needs of vulnerable patients and communities, we must face the increased pressure to lower costs and increase scale to drive positive margins. Those areas are few and far between in not-for-profit healthcare delivery. So, it necessitates that we continue to evolve and think differently about the work that we do driving down costs.
Larsen:And that’s increasingly becoming difficult — even for big players. I’ve been writing ruefully about the “billion-dollar club” — preeminent health systems like Ascension, MGB and Cleveland Clinic each posting more than a billion dollars in total losses (and even more in some cases, e.g., $4.5 billion for Kaiser). But Sanford, in contrast, is one of just a small handful of health systems that somehow managed to end 2022 in the black, with a $188 million operating income last year. Bill, any reflections on how you and the team did that?
Gassen: We count ourselves very, very blessed to be among the few who had the opportunity to experience positive margins in 2022. I would give first and foremost credit to an exceptionally talented team inside and outside the organization. They do a wonderful job of focusing their attention on that which matters most, which is patient care.
It’s also a very well-constructed organization from the ground up. We benefit coming into both the pandemic and then through the financial headwinds in 2022 with a well-diversified set of assets and geographies. On the acute side it’s largely contained across Iowa, South Dakota, and North Dakota.
In Minnesota, and across those above geographies, we have a great complement of assets across our provider sponsored health plan, hospitals, clinics, post-acute care, as well as our research enterprise, all of which, collectively, allowed us to do a better job than some of our peers at weathering that “economic storm” you mentioned earlier.
But, most importantly, it’s just the time that we’ve had to mature as an organization. And with that time, we’ve integrated more deeply as one singular operating company. Sanford Health is not a holding company. The decisions that we make, we make as one singular integrated system and that is a part of that special sauce that’s allowed us to be successful.
Everything that I’ve described has just given us a little bit of a head start and now it’s incumbent upon us to maximize that time.
The imagined and real disruption in healthcare
Q:Bill, you mentioned time is of the essence. And so far, we’ve mostly localized our discussion today talking about health system-specific competitive issues, which makes sense. But it also makes sense to lift up and survey the healthcare ecosystem outside of health systems and note the fact that even when Sanford and Fairview combine and represent $14 billion in revenue, it will still be comparatively tiny to some of the non-traditional players seeking to disrupt healthcare. We have trillion-dollar market cap companies like Amazon investing aggressively into the primary care, pharmacy, and home enablement spaces. We have Fortune 10 companies like UnitedHealth Group and CVS-Aetna vertically integrating and building out sophisticated ambulatory delivery systems. And we have retailers like Walmart and Best Buy transitioning into parts of the healthcare delivery chain as well. So, while Sanford-Fairview will be sizable by most conventional healthcare metrics, it has some pretty formidable competition. How do you assess the new competitive landscape emerging?
Hereford: So, I thought a lot about this because I do think it’s one of the most significant aspects of our industry right now. The opportunity for a CVS-Aetna is that they are proximate to a lot of people in the US. And there’s a lot of things that they could do for patients with a simple presentation of acute symptoms or for fairly simple chronic disease and stabilization. But that is not what drives the cost of health care in the US. It’s when people get very sick.
People receiving specialist care in hospitals are having complex procedures. They’re being treated for complex cancers. And we’re doing an amazing job of advancing the science and the technologies that we can apply to that. But that doesn’t happen in a drug store. That does not happen in a store front primary care office. That happens in organizations like ours. Our challenge is to create the same level of convenience, the same level of access, or partner in a smart way to achieve that.
Our job is to think about total cost of care within the context of delivering very complex care. That isn’t simply a function of primary care and that, I think, is our fundamental challenge. We can translate that into real total cost of care savings.
Gassen: For James and me, in our respective roles and responsibilities, this is our incredibly rewarding and incredibly difficult work. Because those other organizations aren’t required to provide care to everyone. They’re not required to provide free care. They’re not required to be able to provide services for which there is no margin. We don’t get to cherry pick.
It’s our responsibility to really be all things from a healthcare delivery perspective to all people, which means that we are always going to be challenged with how we do that in a financially sustainable way. I think it’s the beauty of where we find ourselves as an industry because out of that necessity comes that innovation that we’ve been talking about here because we can’t continue at current course and speed.
Larsen:When we start to talk about giants in healthcare we tend to index on their size and market cap and, as a result, we lump vertically integrating players and technology companies under the same umbrella. I think that’s a mistake. You have focused healthcare payers like CVS Aetna and UHG that are combining their underwriting business (and ownership of the premium dollar) with an ambulatory delivery network, with an emphasis on home and virtual care. To me that’s a very real and consequential development – and very different from what Big Tech is aspiring to do in our space.
Hereford: Eric, I agree.The world is so clearly changing and that is where the market and a number of very large healthcare organizations are betting. I do think that people who see the overall size of the healthcare marketplace and say “we want to be a part of that” but without any clear way of making sustainable margins.
Gassen: In contrast with the large public companies, as a not-profit health care system, it’s a fact of life that we operate on thin margins. But there are a lot of dollars floating around for other players in the healthcare ecosystem. Which to your point, is why people get enticed to enter into the healthcare space. Our goal with the transaction is to remain financially solid, with the resources needed to invest in our communities, while staying true to our non-profit mission.
Larsen:Your comments, Bill, underscore the power of being a ‘payvider’ in healthcare, which of course Sanford is. You’re in rarefied company — only a dozen or so health systems can claim this, and they have one thing in common — a very mature health plan function (average age of 44 years). So Intermountain, Geisinger, Kaiser, Sentara, Sanford and a small handful of others fit this bill. I presume a major part of the envisioned benefit of the merger is extending Sanford Health plan into Fairview. Can I get you both to comment on that?
Gassen: I certainly agree with you Eric about the importance of being a “payvider.” And of course, I’d also say there is a scale component to that, too. Today our health plan only has 220,000 covered lives. But it is a very valuable and strategic component of the larger Sanford Health system.
As we come together with Fairview into a combined system, we now have the opportunity to bring the Sanford Health plan and its additional options and opportunities for members to a much larger community. And one that’s backed by a combined system. It offers greater choices for the two million people across North Dakota, South Dakota, and Western Minnesota.
When we do that, it puts us in the best possible position to coordinate care that allows for the best outcomes, and as a consequence, also results in a better financial position for us. And so, when we think ahead to the opportunity to now apply the infrastructure that we’ve built to the greater Twin Cities market and beyond to bring that together with the care delivery assets and expertise of Fairview Health Services, we get really excited about the opportunities we unlock not just for the combined organization, but for importantly, for all the members within that community.
Healthcare’s technology paradox
Q:The above commentary on scaling out to wider geographies and connecting and transforming care brings me to the paradox of digital health. One of the only bright lights to come out of the pandemic was what I would characterize as a “Renaissance moment” in digital health — unprecedented funding ($72 billion globally in 2021 alone) fueling the creation of almost 13,000 digital startups, spanning new diagnostics, therapeutics, clinical/non-clinical workflow, care augmentation, you name it. And while we’re now seeing a rough contraction, with lots of companies starved for capital and struggling to sell into healthcare incumbents, we are going to see some winners and some transformational platforms emerge.
The question is, will healthcare incumbents like health systems be able to take advantage of this? The data are sobering — it takes an estimated 23 months for a health system to deploy a digital health technology (once it signs a contract). And while technology tends to be deflationary — lowers costs as it augments productivity — that just hasn’t happened in healthcare, as costs inexorably keep going up. How will the combined Sanford-Fairview tackle this? Who wants to go first?
Hereford: Let me start because I want to respond to something you said, Eric. You’re right, technology has been deflationary in other sectors but only since about 1995. In the 1990s many books in that period were asking “why are we investing all this money in technology across all sectors and we’re not seeing productivity improvements?”
But out of that question came reengineering — where companies started to reconfigure processes and workflows as opposed to just applying technologies. Only then did they see the deflationary benefits of greater efficiencies from technologies. So, I think that has a lot to do with how we’ve applied technology. We’ve had federal stimulus to apply technology, but it’s to apply technology for its own sake. Not to challenge how we use technology to make it easier to be a doctor or nurse. How do we use technology to make people more effective and therefore more efficient?
Gassen: I think that change, especially fundamental shifts, and changes to a business won’t happen until you absolutely have to. And that’s human nature.
The challenge ahead of us is to interrogate how we as an industry interact with our patients and ask, “How can we fundamentally tear that down to the studs and rebuild it better and fit for today?”
But I also want to be clear about why we’re here as a health system. Our reality is that there is a patient at the end of every single decision that we make. So, we must be extremely careful about how we look at processes and implement change. We know they’re rarely perfect, but oftentimes we do deliver the best outcome for the patient. Our job is to be able to make the right change without causing harm.
Larsen:Bill, we’ve made the argument together in past conversations that this same creation moment for digital health solutions beautifully aligns to address the conventional disadvantages of American rural medicine: insufficient infrastructure (hospitals, surgery centers, etc.) and a scarcity of clinicians and non-clinicians for the workforce. Digital health holds the promise to turn those deficits into advantages. And, you know, Sanford’s been a pioneer in launching a $350 million virtual hospital. Perhaps you can unpack this.
Gassen: I’d say our work here really has its origins in the unwavering belief that one zip code should not determine the level of care that a person receives. Every patient has the right to access world class care. So, it’s incumbent upon us, those of us who find ourselves in the privileged position to be in leadership in healthcare delivery organizations like Sanford and Fairview, to take the necessary steps to deploy the appropriate resources and to find the right partners to ensure that whether you’re living in the most rural parts of the heartland or an urban center, you get the best quality care possible.
We take great pride in the fact that our organization was built on the belief that we know many of our patients choose to live in rural America. Two-thirds of the patients today at Sanford Health, whom we have the privilege of serving, come to us from rural America.
It’s with that front and center, the Virtual Care initiative at Sanford Health is allowing us the opportunity to deliver world class care. It’s about making certain that through basically all facets of digital transformation, we leverage our resources to extend excellence in primary care, in specialty and subspecialty care, and offer those individuals access to that care close to home.
The vision for us is to ensure that those who choose to live in rural America are not forced to sacrifice access to high quality, dependable care. That’s at the core of both our beliefs and actions.
Larsen:And James, I think you’ve been one of the most progressive CEOs in the industry on thinking about capitalizing on digital health, innovation and partnering with capital allocators. And we talked about a few of them — leading VCs like Thrive or SignalFire who are partnering broadly with health systems — and finding ways to shorten the innovation cycle.
Hereford: It comes back to intent and purpose. Our job is to make sure that everybody can access high quality care and so the opportunity is to really think about the commonalities and leverage that across both rural America, urban communities, suburbs, exurbs, etc. The other thing that I think is often overlooked in your Cambrian explosion is the volume of scientific advancements over the last two decades.
I love the hypothetical of a medical student who learned everything about medicine in 1950 and how fast the volume of clinical knowledge would have doubled then. They would have had about 50 years before the knowledge base doubled. Today, an amazing medical student with the ambition to learn the entire body of clinical knowledge would have about seven months to see it doubled. That’s how fast medicine is advancing.
We built this industry based on highly specialized, incredibly smart, incredibly committed people who can master these topics. This volume of information on clinical care theory, the body of knowledge on clinical application, all layered on to how the business of care works is cognitive overload. We have got to give them better tools. We have got to help support them. I think we’re in a unique place to be able to really do something about it and create real solutions for people.
Gassen: Where we’re at right now necessitates that. And again, thinking a level deeper as it relates to rural America, the opportunity is so incredibly ripe because it’s necessary. The only way that we’re going to be able to scale to the level we need is to leverage and maximize technology. And so therein creates that opportunity and that necessity makes us a very fertile ground for organizations to come in and partner with us, to be able to extend those services.
The current deal’s state of play
Q:So, we started our conversation about the merger and went broad to talk about industry trends and the wider landscape. But I do want to circle back to a couple of the outstanding specifics of the merger. Sanford and Fairview are merging. What will the University of Minnesota’s relationship be with the merged organization?
Gassen: Both James and I firmly believe, and have articulated in our conversation with you today, the virtues of bringing Sanford Health and Fairview Health services together are absolutely essential to ensuring the delivery of world class healthcare in the upper Midwest. And we are committed to creating the right relationship with the University of Minnesota for it to pursue its mission.
Hereford: We’ve always said that we wanted the University to be part of what we’re building. And, the University of Minnesota has indicated their desire to purchase the academic assets of the system and we stand ready to engage with them to support that. If that is the path that they pursue and can get state funding to support, then we can work with them to determine the nature of the relationship between the new system and the University of Minnesota.
Larsen:And how about the other partners and players in the landscape? I’m thinking of the Minnesota Attorney General, the FTC, etc.
Gassen: We’ve engaged the elected officials across the states of North Dakota, South Dakota, and Minnesota, and we’ve continued to keep them apprised. We’ve also worked very closely with regulators and are happy to report that following its review, the Federal Trade Commission cleared the transaction and the HSR process is complete.
At this point in time, we are working closely with Attorney General Keith Ellison’s office in the state of Minnesota to ensure that he has sufficient information to complete his analysis under antitrust and charities laws to ensure that he’s continuing to protect the interests of all Minnesotans. We remain very engaged and look forward to the conclusion of that work.
The future focus of leadership
Q:Ok, I’d like to round out this conversation with a look to the future. Can you foreshadow your division of labor…where you will be converging and where will you be dividing and conquering as CEOs?
Hereford: One of the great positives of this deal and one of the great signals of the quality of the rationale here is that Bill and I went into this with the question: How do we set this up to be successful over the long term?
You may have noticed Bill and I are different ages. Bill has a lot more runway than I have, so it was not a difficult decision on my part to say “look, it’s important for me to help with the transition because it’s a big deal, right? And it’s not going to be over in a year.” But I can be that bridging function to help support the transition. This is a long-term play and Bill’s the person who’s going to be able to be in the seat to really see that through.
And given my interests I can take on the innovation that we’re talking about and how we make the membrane of this organization a little more permeable and a little bit more friendly to partners, while also being very demanding of partners in terms of the value they create, and we create within the system.
I’m really excited about the opportunity to do that. I do think the way that we have approached this is a very enlightened approach.
Gassen: Standing on the shoulders of James’ comments, one of the many aspects that makes this merger unique is the collegiality and foresight from our respective boards that see how incredibly valuable it is to be able to have co-CEOs working together, focusing first and foremost on ensuring that we’re bringing together the two organizations as one integrated, transformative healthcare delivery organization. I think James and I get up every morning with the goal of making sure that that happens every single day.
And it’s not just that James will work on the innovation piece because it brings him joy and energy but also, it’s where he has a deep level of experience and expertise. I get to focus more of my time and energy on the day-to-day of the two organizations coming together.
Together, James and I will be able to jointly balance the combination of the two organizations with day-to-day delivery and the transformative opportunities for us because of the unique nature of our backgrounds and expertise.
Hereford: And I think that’s a real advantage for the organization. I’m sure there are going be times when I’ll say “Bill, we’ve got to change. You’ve got to do this”. And he’s going to say “yeah, but I can’t do that. I can’t make that kind of change.”
But that’s the kind of dialogue that this structure sets up for us to hold that tension productively as opposed to responding to the tyranny of the urgent, which is ever present in a large health care delivery system. Transformation of care delivery systems will require the ability to manage those competing dynamics. I really appreciate both the structure but also how Bill is approaching this.
Gassen: I do think that what we just described here will prove to be one of the finer distinguishing factors that allows us to really be successful. Because you do oftentimes find yourself with a choice between A or B. And for us we get to choose C — “all of the above” — and go forward and do that.
At a recent meeting of physician leaders, we sat next to the head of the health system’s bariatric surgery program. Given the recent and rapid uptake of GLP-1 inhibitors like Ozempic and Wegovy, we asked how he thought these drugs, which can generate dramatic weight loss, would affect his practice.
He chuckled, “they’re really good drugs…they could put me out of business!
It’s too early to say if they’ll be effective over a lifetime, but there’s no doubt they’re going to have a huge impact on our work.” It got us thinking about the other reverberations this class of drugs could have on care needs, if a majority of obese Americans had access to them.
Some effects are obvious.
We could see significant declines in treatment needs for chronic diseases like obesity and heart failure, for which obesity is a strong risk factor. Given that obese patients are much more likely to need joint replacement surgery, we could see a big hit to that demand—although some patients who are poor candidates for surgery because of weight-related complications could become eligible.
Even longer-term, if American’s aren’t dying of chronic disease, we’ll still die of something, so expect diseases of advanced age, like Alzheimer’s and many cancers, to increase. Other pharmaceutical innovations, like the growth of immunotherapy and more targeted cancer treatments, also have the potential to radically alter how disease is managed.
We may be at the beginning of another wave of disruptive medical innovation on the order of the introduction of statins in the 1990s, which combined with minimally invasive catheterization, slashed the need for bypass surgery.
Given their sky-high prices, it’s too soon to tell how quickly the use of these new obesity drugs will grow, but innovations like these will serve to pull more care out of hospitals and into less invasive outpatient medical management.
The film “American Hospitals: Healing a Broken System” premiered in Washington, D.C., on March 29. This documentary exposes the inconvenient truths embedded within the U.S. healthcare system. Here is a dirty dozen of them:
Hospitals are largely unaccountable for poor clinical outcomes.
The cost of commercially insured care is multiples higher than the cost of government-insured care for identical procedures.
Customer service at hospitals is dreadful.
Frontline clinicians are overburdened and leaving the profession in droves.
Healthcare still operates the same way it has for the last one hundred years — delivering hierarchical, fragmented, hospital-centric, disease-centric, physician-centric “sick” care. Accordingly, healthcare business models optimize revenue generation and profitability rather than health outcomes. These factors explain, in part, why U.S. life expectancy has declined four of the five years and maternal deaths are higher today than a generation ago.
It’s hard to imagine that the devil itself could create a more inhumane, ineffective, costly and change-resistant system. Hospitals consume more and more societal resources to maintain an inadequate status quo. They’re a major part of America’s healthcare problem, certainly not its solution. Even so, hospitals have largely avoided scrutiny and the public’s wrath. Until now.
“American Hospitals” is now playing in theaters throughout the nation. It chronicles the pervasive and chronic dysfunction plaguing America’s hospitals. It portrays the devastating emotional, financial and physical toll that hospitals impose on both consumers and caregivers.
Despite its critical lens, “American Hospitals” is not a diatribe against hospitals. Its contributors include some of healthcare’s most prominent and respected industry leaders, including Donald Berwick, Elizabeth Rosenthal, Shannon Brownlee and Stephen Klasko. The film explores payment and regulatory reforms that would deliver higher-value care. It profiles Maryland’s all-payer system as an example of how constructive reforms can constrain healthcare spending and direct resources into more effective, community-based care.
The United States already spends more than enough on healthcare. It doesn’t need to spend more. It needs to spend more wisely. The system must downsize its acute and specialty care footprint and invest more in primary care, behavioral health, chronic disease management and health promotion. It’s really that simple.
My only critique of “American Hospitals” is many of its contributors expect too much from hospitals. They want them to simultaneously improve their care delivery and advance the health of their communities. This is wishful thinking. Health and healthcare are fundamentally different businesses. Rather than pivoting to population health, hospitals must focus all their efforts on delivering the right care at the right time, place and price.
If hospitals can deliver appropriate care more affordably, this will free up enormous resources for society to invest in health promotion and aligned social-care services. In this brave new world, right-sized hospitals deliver only necessary care within healthier, happier and more productive communities.
All Americans deserve access to affordable health insurance that covers necessary healthcare services without bankrupting them and/or the country. Let me restate the obvious. This requires less healthcare spending and more investments in health-creating activities. Less healthcare and more health is the type of transformative reform that the country could rally behind.
At issue is whether America’s hospitals will constructively participate in downsizing and reconfiguring the nation’s healthcare system. If they do so, they can reinvent themselves from the inside out and control their destinies.
Historically, hospitals have preferred to use their political and financial leverage to protect their privileged position rather than advance the nation’s well-being. Like Satan in Milton’s “Paradise Lost,” they have preferred to reign in hell rather than serve in heaven.
Pride comes before the fall. Woe to those hospitals that fight the nation’s natural evolution toward value-based care and healthier communities. They will experience a customer-led revolution from outside in and lose market relevance. Only by admitting and addressing their structural flaws can hospitals truly serve the American people.
In a matter of months, ChatGPT has radically altered our nation’s views on artificial intelligence—uprooting old assumptions about AI’s limitations and kicking the door wide open for exciting new possibilities.
One aspect of our lives sure to be touched by this rapid acceleration in technology is U.S. healthcare. But the extent to which tech will improve our nation’s health depends on whether regulators embrace the future or cling stubbornly to the past.
Why our minds live in the past
In the 1760s, Scottish inventor James Watt revolutionized the steam engine, marking an extraordinary leap in engineering. But Watt knew that if he wanted to sell his innovation, he needed to convince potential buyers of its unprecedented power. With a stroke of marketing genius, he began telling people that his steam engine could replace 10 cart-pulling horses. People at time immediately understood that a machine with 10 “horsepower” must be a worthy investment. Watt’s sales took off. And his long-since-antiquated meaurement of power remains with us today.
Even now, people struggle to grasp the breakthrough potential of revolutionary innovations. When faced with a new and powerful technology, people feel more comfortable with what they know. Rather than embracing an entirely different mindset, they remain stuck in the past, making it difficult to harness the full potential of future opportunities.
Too often, that’s exactly how U.S. government agencies go about regulating advances in healthcare. In medicine, the consequences of applying 20th-century assumptions to 21st-century innovations prove fatal.
Here are three ways regulators do damage by failing to keep up with the times:
1. Devaluing ‘virtual visits’
Established in 1973 to combat drug abuse, the Drug Enforcement Administration (DEA) now faces an opioid epidemic that claims more than 100,000 lives a year.
One solution to this deadly problem, according to public health advocates, combines modern information technology with an effective form of addiction treatment.
Thanks to the Covid-19 Public Health Emergency (PHE) declaration, telehealth use skyrocketed during the pandemic. Out of necessity, regulators relaxed previous telemedicine restrictions, allowing more patients to access medical services remotely while enabling doctors to prescribe controlled substances, including buprenorphine, via video visits.
For people battling drug addiction, buprenorphine is a “Goldilocks” medication with just enough efficacy to prevent withdrawal yet not enough to result in severe respiratory depression, overdose or death. Research from the National Institutes of Health (NIH) found that buprenorphine improves retention in drug-treatment programs. It has helped thousands of people reclaim their lives.
But because this opiate produces slight euphoria, drug officials worry it could be abused and that telemedicine prescribing will make it easier for bad actors to push buprenorphine onto the black market. Now with the PHE declaration set to expire, the DEA has laid out plans to limit telehealth prescribing of buprenorphine.
The proposed regulations would let doctors prescribe a 30-day course of the drug via telehealth, but would mandate an in-person visit with a doctor for any renewals. The agency believes this will “prevent the online overprescribing of controlled medications that can cause harm.”
The DEA’s assumption that an in-person visit is safer and less corruptible than a virtual visit is outdated and contradicted by clinical research. A recent NIH study, for example, found that overdose deaths involving buprenorphine did not proportionally increase during the pandemic. Likewise, a Harvard study found that telemedicine is as effective as in-person care for opioid use disorder.
Of course, regulators need to monitor the prescribing frequency of controlled substances and conduct audits to weed out fraud. Furthermore, they should demand that prescribing physicians receive proper training and document their patient-education efforts concerning medical risks.
But these requirements should apply to all clinicians, regardless of whether the patient is physically present. After all, abuses can happen as easily and readily in person as online.
The DEA needs to move its mindset into the 21st century because our nation’s outdated approach to addiction treatment isn’t working. More than 100,000 deaths a year prove it.
2. Restricting an unrestrainable new technology
Technologists predict that generative AI, like ChatGPT, will transform American life, drastically altering our economy and workforce. I’m confident it also will transform medicine, giving patients greater (a) access to medical information and (b) control over their own health.
So far, the rate of progress in generative AI has been staggering. Just months ago, the original version of ChatGPT passed the U.S. medical licensing exam, but barely. Weeks ago, Google’s Med-PaLM 2 achieved an impressive 85% on the same exam, placing it in the realm of expert doctors.
With great technological capability comes great fear, especially from U.S. regulators. At the Health Datapalooza conference in February, Food and Drug Administration (FDA) Commissioner Robert M. Califf emphasized his concern when he pointed out that ChatGPT and similar technologies can either aid or exacerbate the challenge of helping patients make informed health decisions.
Worried comments also came from Federal Trade Commission, thanks in part to a letter signed by billionaires like Elon Musk and Steve Wozniak. They posited that the new technology “poses profound risks to society and humanity.” In response, FTC chair Lina Khan pledged to pay close attention to the growing AI industry.
Attempts to regulate generative AI will almost certainly happen and likely soon. But agencies will struggle to accomplish it.
To date, U.S. regulators have evaluated hundreds of AI applications as medical devices or “digital therapeutics.” In 2022, for example, Apple received premarket clearance from the FDA for a new smartwatch feature that lets users know if their heart rhythm shows signs of atrial fibrillation (AFib). For each AI product that undergoes FDA scrutiny, the agency tests the embedded algorithms for effectiveness and safety, similar to a medication.
ChatGPT is different. It’s not a medical device or digital therapy programmed to address a specific or measurable medical problem. And it doesn’t contain a simple algorithm that regulators can evaluate for efficacy and safety. The reality is that any GPT-4 user today can type in a query and receive detailed medical advice in seconds. ChatGPT is a broad facilitator of information, not a narrowly focused, clinical tool. Therefore, it defies the types of analysis regulators traditionally apply.
In that way, ChatGPT is similar to the telephone. Regulators can evaluate the safety of smartphones, measuring how much electromagnetic radiation it gives off or whether the device, itself, poses a fire hazard. But they can’t regulate the safety of how people use it. Friends can and often do give each other terrible advice by phone.
Therefore, aside from blocking ChatGPT outright, there’s no way to stop individuals from asking it for a diagnosis, medication recommendation or help with deciding on alternative medical treatments. And while the technology has been temporarily banned in Italy, that’s unlikely to happen in the United States.
If we want to ensure the safety of ChatGPT, improve health and save lives, government agencies should focus on educating Americans on this technology rather than trying to restrict its usage.
3. Preventing doctors from helping more people
Doctors can apply for a medical license in any state, but the process is time-consuming and laborious. As a result, most physicians are licensed only where they live. That deprives patients in the other 49 states access to their medical expertise.
The reason for this approach dates back 240 years. When the Bill of Rights passed in 1791, the practice of medicine varied greatly by geography. So, states were granted the right to license physicians through their state boards.
In 1910, the Flexner report highlighted widespread failures of medical education and recommended a standard curriculum for all doctors. This process of standardization culminated in 1992 when all U.S. physicians were required to take and pass a set of national medical exams. And yet, 30 years later, fully trained and board-certified doctors still have to apply for a medical license in every state where they wish to practice medicine. Without a second license, a doctor in Chicago can’t provide care to a patient across a state border in Indiana, even if separated by mere miles.
The PHE declaration did allow doctors to provide virtual care to patients in other states. However, with that policy expiring in May, physicians will again face overly restrictive regulations held over from centuries past.
Given the advances in medicine, the availability of technology and growing shortage of skilled clinicians, these regulations are illogical and problematic. Heart attacks, strokes and cancer know no geographic boundaries. With air travel, people can contract medical illnesses far from home. Regulators could safely implement a common national licensing process—assuming states would recognize it and grant a medical license to any doctor without a history of professional impropriety.
But that’s unlikely to happen. The reason is financial. Licensing fees support state medical boards. And state-based restrictions limit competition from out of state, allowing local providers to drive up prices.
To address healthcare’s quality, access and affordability challenges, we need to achieve economies of scale. That would be best done by allowing all doctors in the U.S. to join one care-delivery pool, rather than retaining 50 separate ones.
Doing so would allow for a national mental-health service, giving people in underserved areas access to trained therapists and helping reduce the 46,000 suicides that take place in America each year.
Regulators need to catch up
Medicine is a complex profession in which errors kill people. That’s why we need healthcare regulations. Doctors and nurses need to be well trained, so that life-threatening medications can’t fall into the hands of people who will misuse them.
But when outdated thinking leads to deaths from drug overdoses, prevents patients from improving their own health and limits access to the nation’s best medical expertise, regulators need to recognize the harm they’re doing.
Healthcare is changing as technology races ahead. Regulators need to catch up.