As everyone in our industry knows, sluggish volumes amid persistently rising costs, especially for labor, have sent health system margins into a downward spiral across 2022. Using the latest data from consultancy Kaufman Hall, the graphic above shows that by the end of this year, employed labor expenses will have increased more than all non-labor costs combined.
While contract labor usage, namely travel nursing, is declining, the constant battle for nursing talent means travel nurses are still a significant expense at many hospitals. Through the first six months of this year, over half of hospitals reported a negative operating margin, and the median hospital operating margin has dropped over 100 percent from 2019.
Larger health systems are not faring better: all five of the large, multi-regional, not-for-profit systems we’ve highlighted below saw their operating margins tumble this year, with drops ranging from three points (Kaiser Permanente) to nearly seven points (CommonSpirit Health and Providence).
While these unfavorable cost trends have been building throughout COVID, health systems now have neither federal relief nor returns from a thriving stock market to help stabilize their deteriorating financial outlooks.
Health system boards will tolerate negative margins in the short-term (especially given that many have months’ worth of days cash on hand), but if this situation persists into 2023, pressure for service cuts, layoffs, and restructuring will mount quickly.
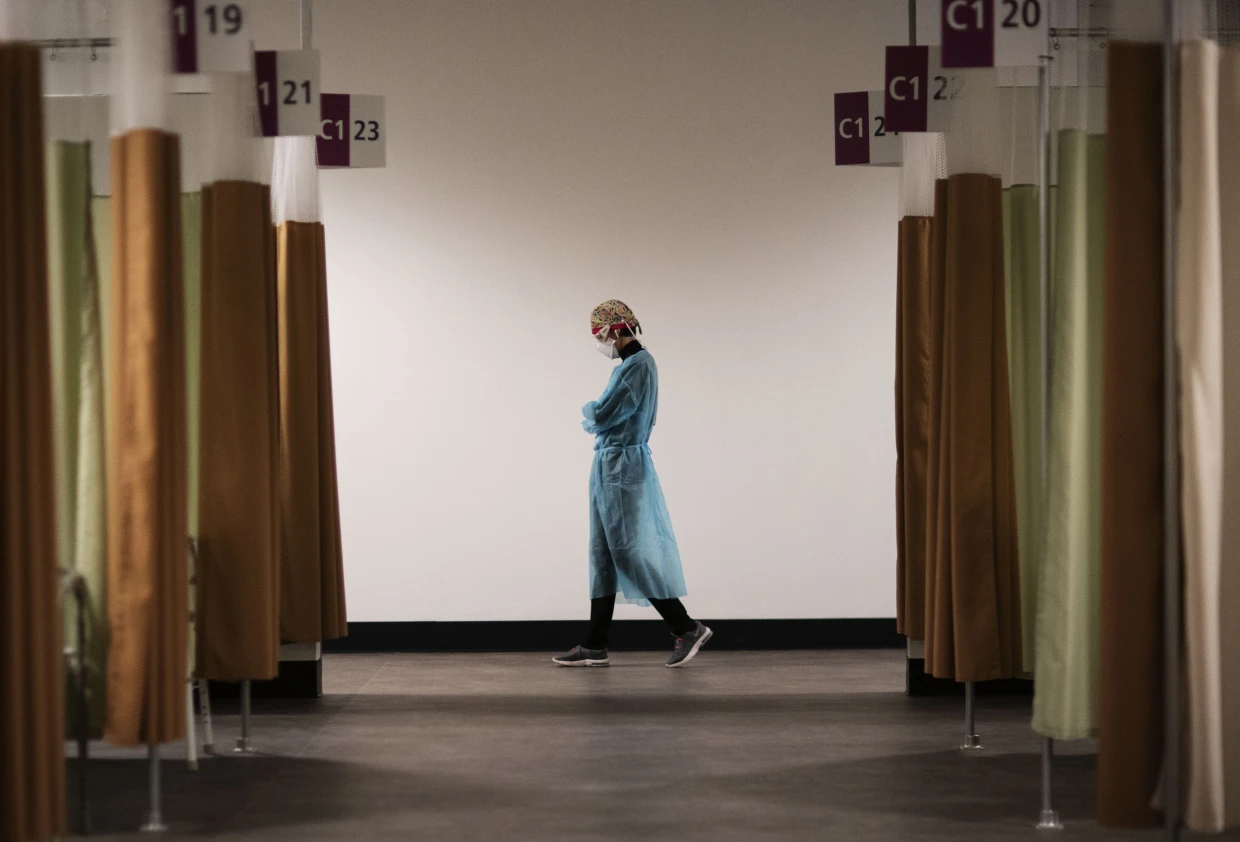
An ICU nurse helps to prepare medicine for a covid patient in St. Cloud, Minn. Nurses in the state are planning to go on a three-day strike starting Sept. 12.
About 15,000 nurses in Minnesota walked off the job Monday to protest understaffing and overwork — marking the largest strike of private-sector nurses in U.S. history.
Slated to last three days, the strike spotlights nationwide nursing shortages exacerbated by the coronavirus pandemic that often result in patients not receiving adequate care. Tensions remain high between nurses and health-care administrators across the country, and there are signs that work stoppages could spread to other states.
Minnesota nurses charge that some units go without a lead nurse on duty and that nurses fresh out of school are delegated assignments typically held by more experienced nurses, across some 16 hospitals where strikes are expected.
The nurses are demanding a role in staffing plans, changes to shift scheduling practices and higher wages.
“I can’t give my patients the care they deserve,” said Chris Rubesch, the vice president of the Minnesota Nurses Association and a nurse at Essentia Health in Duluth. “Call lights go unanswered. Patients should only be waiting for a few seconds or minutes if they’ve soiled themselves or their oxygen came unplugged or they need to go to the bathroom, but that can take 10 minutes or more. Those are things that can’t wait.”
Paul Omodt, a spokesman for the Twin Cities Hospital Group, which represents four hospital systems where nurses are striking in the Minneapolis-St. Paul area, said that the nurses union did not do everything it could to avoid a strike.
“Nurses have steadfastly refused to go to mediation,” Omodt said. “Their choice is to strike. This strike is on the nurses.”
Conny Bergerson, a spokeswoman for Allina Health, another hospital system in the Twin Cities where nurses are on strike, said “rushing to a strike before exhausting all options such as engaging a neutral federal mediator does not benefit our employees, patients or the communities we serve.”
The Minnesota Nurses Association, the nurses union, said hospital administrators have continued to “refuse solutions” on understaffing and safety in contract negotiations. It said nurses have increasingly been asked to take on more patients for bedside care to make up for labor shortages, exacerbating burnout and high turnover.
Some hospitals have offered increased safety protocols for reporting security incidents in negotiations, but have not budged on other safety- and staffing-related demands.
The union has proposed new mechanisms for nurses to have a stronger say in how wards are staffed, including a committee made up of nurses and management at each hospital that would determine appropriate staffing levels. It has also proposed protections against retaliation for nurses who report understaffing. Striking nurses at some hospitals said their shifts are often short five to 10 nurses, forcing nurses to take on more patients than they can handle.
Omodt said that while there was a rise in understaffing reports during the height of covid, conditions have improved, and nurses have made contradictory claims when it comes to staffing at their hospitals since then.
In the lead-up to the strike, Minnesota hospital groups filed unfair labor practices charges against the union for refusing to go to mediation, and asked the National Labor Relations Board to block the strike for a failure to provide enough notice. The NLRB has thrown out at least some of those charges.
Hospitals facing strikes have been recruiting traveling nurses from across the region and plan to maintain staffing levels during the strike, though they are preparing for reduced operations, according to some of the hospital groups facing strike activity.
For years, hospitals in the United States have faced understaffing problems. A surge in demand and increased safety risks for nurses during the pandemic accelerated those trends. The number of health-care workers in the United States has still not recovered to its pre-pandemic levels, down 37,000 workers compared with February 2020.
At the same time, demand for health-care services has steadily increased during the pandemic, with a backlog of people who delayed care now seeking medical attention. During the covid wave that swept across the United States this summer, states such as New York and Florida reported the worst nursing shortages in decades. Research shows that patients are more likely to die because of preventable reasons when health-care providers are overworked.
Nurses, who risked their lives during the pandemic, are quitting and retiring early in droves, because of increased workloads caused by short staffing and demanding schedules that make finding child care and having a life outside of work exceedingly difficult. The understaffing crisis is pronounced in Minnesota in part because of its aging population and its record low unemployment rate.
There are some signs that nurse- and other health-care-worker strikes could spill over to other states in the coming weeks. Four thousand nurses with the Michigan Nurses Association voted earlier this month to authorize a strike related to understaffing concerns, and 7,000 health-care workers in Oregon have also authorized a work stoppage. University of Wisconsin nurses narrowly averted a strike this week. Therapists and clinicians in Hawaii and California are currently in the fourth week of what has become the longest-running mental health care strike, over inadequate staffing levels.
In Minnesota, the Minnesota Nurses Association recorded a 300 percent increase in nurses’ reports of unsafe staffing levels on their shifts since 2014, up to 7,857 reports in 2021.
Kelley Anaas, 37, a nurse who works in the ICU at Abbott Northwestern in Minneapolis said nurses in her unit have been forced to double up on patient assignments and work with lead nurses who have less than a year of experience.
“It eats away at you. If that was my family member in that bed, I wouldn’t want to leave their side,” said Anaas, adding that her workload has increased steadily over her 14 years at Abbott Northwestern.
While the nurses say their main impetus for striking is staffing levels and not pay, they are also at odds with hospitals over wages. The Minnesota Nurses Association has proposed a 30 percent pay increase over the next three years, noting inflation is at a 40-year high, while health-care groups have proposed a pay increase of 10 to 12 percent.
“The union’s wage demands remain at 29 and 30 percent increases over three years, which we’ve told them is unrealistic and unaffordable,” Omodt said, noting that the average Minnesota nurse makes $80,960 a year.
Contracts expired in May and June, and the union has been in negotiations since March.
Nurses said they are frustrated the strike is happening, but the stakes are high for them and their patients.
“We’re really sad and disappointed that it has come to a strike,” said Brianna Hnath, a nurse at North Memorial in Robbinsdale. “But we feel like this is the only thing we can do to show administration how incredibly important a strong nursing core is to a hospital. Hospitals tell us it’s our fault, but we’ve been actively involved and getting nowhere.”
Working as a travel nurse in the early days of the Covid pandemic was emotionally exhausting for Reese Brown — she was forced to leave her young daughter with her family as she moved from one gig to the next, and she watched too many of her intensive care patients die.
“It was a lot of loneliness,” Brown, 30, said. “I’m a single mom, I just wanted to have my daughter, her hugs, and see her face and not just through FaceTime.”
But the money was too good to say no. In July 2020, she had started earning $5,000 or more a week, almost triple her pre-pandemic pay. That was the year the money was so enticing that thousands of hospital staffers quit their jobs and hit the road as travel nurses as the pandemic raged.
Two years later, the gold rush is over. Brown is home in Louisiana with her daughter and turning down work. The highest paid travel gigs she’s offered are $2,200 weekly, a rate that would have thrilled her pre-pandemic. But after two “traumatic” years of tending to Covid patients, she said, it doesn’t feel worth it.
“I think it’s disgusting because we went from being praised to literally, two years later, our rates dropped,” she said. “People are still sick, and people are still dying.”
The drop in pay doesn’t mean, however, that travel nurses are going to head back to staff jobs. The short-lived travel nurse boom was a temporary fix for a long-term decline in the profession that predates the pandemic. According to a report from McKinsey & Co., the United States may see a shortage of up to 450,000 registered nurses within three years barring aggressive action by health care providers and the government to recruit new people. Nurses are quitting, and hospitals are struggling to field enough staff to cover shifts.
Nine nurses around the country, including Brown, told NBC News they are considering alternate career paths, studying for advanced degrees or exiting the profession altogether.
“We’re burned out, tired nurses working for $2,200 a week,” Brown said. People are leaving the field, she said, “because there’s no point in staying in nursing if we’re expendable.”
$124.96 an hour
Travel nursing seems to have started as a profession, industry experts say, in the late 1970s in New Orleans, where hospitals needed to add temporary staff to care for sick tourists during Mardi Gras. In the 1980s and the 1990s, travel nurses were often covering for staff nurses who were on maternity leave, meaning that 13-week contracts become common.
By 2000, over a hundred agencies provided travel contracts, a number that quadrupled by the end of the decade. It had become a lucrative business for the agencies, given the generous commissions that hospitals pay them. A fee of 40 percent on top of the nurse’s contracted salary is not unheard of, according to a spokesperson for the American Health Care Association, which represents long-term care providers.
Just before the pandemic, in January 2020, there were about 50,000 travel nurses in the U.S., or about 1.5 percent of the nation’s registered nurses, according to Timothy Landhuis, vice president of research at Staffing Industry Analysts, an industry research firm. That pool doubled in size to at least 100,000 as Covid spread, and he says the actual number at the peak of the pandemic may have far exceeded that estimate.
By 2021, travel nurses were earning an average of $124.96 an hour, according to the research firm — three times the hourly rate of staff nurses, according to federal statistics.
That year, according to the 2022 National Health Care Retention & RN Staffing Report from Nursing Solutions Inc., a nurse recruiting firm, the travel pay available to registered nurses contributed to 2.47% of them leaving hospital staff jobs.
But then, as the rate of deaths and hospitalizations from Covid waned, the demand for travel nurses fell hard, according to industry statistics, as did the pay.
Demand dropped 42 percent from January to July this year, according to Aya Healthcare, one of the largest staffing firms in the country.
That doesn’t mean the travel nurses are going back to staff jobs.
Brown said she’s now thinking about leaving the nursing field altogether and has started her own business. Natalie Smith of Michigan, who became a travel nurse during the pandemic, says she intends to pursue an advanced degree in nursing but possibly outside of bedside nursing.
Pamela Esmond of northern Illinois, who also became a travel nurse during the pandemic, said she’ll keep working as a travel nurse, but only because she needs the money to retire by 65. She’s now 59.
“The reality is they don’t pay staff nurses enough, and if they would pay staff nurses enough, we wouldn’t have this problem,” she said. “I would love to go back to staff nursing, but on my staff job, I would never be able to retire.”
The coronavirus exacerbated issues that were already driving health care workers out of their professions, Landhuis said. “A nursing shortage was on the horizon before the pandemic,” he said.
According to this year’s Nursing Solutions staffing report, nurses are exiting the bedside at “an alarming rate” because of rising patient ratios, and their own fatigue and burnout. The average hospital has turned over 100.5% of its workforce in the past five years, according to the report, and the annual turnover rate has now hit 25.9%, exceeding every previous survey.
There are now more than 203,000 open registered nurse positions nationwide, more than twice the number just before the pandemic in January 2020, according to Aya Healthcare.
An obvious short-term solution would be to keep using travel nurses. Even with salaries falling, however, the cost of hiring them is punishing.
LaNelle Weems, executive director of Mississippi Hospital Association’s Center for Quality and Workforce, said hospitals can’t keep spending like they did during the peak of the pandemic.
“Hospitals cannot sustain paying these exorbitant labor costs,” Weems said. “One nuance that I want to make sure you understand is that what a travel agency charges the hospitals is not what is paid to the nurse.”
Ultimately, it’s the patients who will suffer from the shortage of nurses, whether they are staff or gig workers.
“Each patient added to a hospital nurse’s workload is associated with a 7%-12% increase in hospital mortality,” said Linda Aiken, founding director of the University of Pennsylvania’s Center for Health Outcomes and Policy Research.
Nurses across the country told NBC News that they chose the profession because they cared about patient safety and wanted to be at the bedside in the first line of care.
“People say it’s burnout but it’s not,” Esmond said about why nurses are quitting. “It’s the moral injury of watching patients not being taken care of on a day-to-day basis. You just can’t take it anymore.”
The COVID-19 pandemic intensified hospitals’ reliance on travel nurses to address staffing shortages and highlighted the gap between full-time workers’ pay and lucrative temporary contracts. In the third year of the pandemic, hospitals continue to rely on travel nurses and grapple with workforce shortages for a variety of reasons. However, some organizations have reduced their reliance on travel nurses, and pay overall is lower compared to certain points of the pandemic, experts told Becker’s.
Here are seven travel nurse pay trends for healthcare leaders to know, per Vivian Health, a national healthcare hiring marketplace used by about 800,000 clinicians, and AMN Healthcare, a medical staffing firm based in Coppell, Texas:
1. The average weekly travel nurse pay in July in the U.S. was $2,997, up 12 percent from $2,681 during the same time in 2021, according to a report from Vivian Health. The report, which was shared with Becker’s, is based on proprietary data of job postings on Vivian Health in July.
2. Among states, Alaska saw thelargest average increase to travel nurse pay in July compared to the same time in 2021, according to the Vivian Health report. Florida saw the largest average decrease.
3. When taking a month-over-month view of 2022, average travel nurse pay is declining and coming back to last year’s levels, according to Vivian Health. The company cited several factors for this trend, such as a shift away from travel roles and toward permanent nursing roles as well as less federal money being shifted toward hospitals for large travel contracts.
4. Rishabh Parmar, head of strategy and operations at Vivian Health, told Becker’s: “Compared with July 2021, we still see that travel rates are higher [year over year] — close to around 12 percent to 15 percent — but it seems to be stabilized. Now, in terms of the demand, there’s still a lot of demand out there.”
5. Mr. Parmar estimated that available travel nurse jobs on Vivian Health’s platform doubled in July 2021 compared to pre-pandemic numbers in March 2020. As of July 2022, they were at 2.7 times the rate of March 2020 job numbers.
6. AMN Healthcare also reported lower rates. “According to a recent earnings call, AMN Healthcare expects the company will exit 2022 with travel nurse and allied healthcare professional bill rates at approximately 30 percent lower than first-quarter levels,” the company told Becker’s. “Though demand for travel nurses and allied professionals has declined from an all-time high in Q1, the company expects persistent vacancies and labor shortages to continue.”
7. Some hospitals “are saying, ‘We need to use travel nurses, we just have to use [travel contracts] at lower rates,'” Mr. Parmar said. Some organizations are also offering internal travel programs amid an opportunity to attract workers while decreasing contract labor expenses.
As RNs struggle to work through staffing shortages, their job satisfaction has sharply declined, with 67% saying they plan to leave their jobs within the next few years, according to a survey from the American Association of Critical-Care Nurses (AACN) published in Critical Care Nurse.
RNs cite poor work environments
For the survey, AACN collected responses from 9,862 nurses, 9,335 of which met the study criteria of being currently practicing RNs, in October 2021. The mean age was 46.5 years, and the mean years of experience was 17.8 years.
Of the participants, 78.3% worked in direct care, and 19.4% worked in a Beacon unit, meaning that their unit had been recognized by an AACN Beacon Award for Excellence. Half of the participants said they spent 50% or less of their time caring for Covid-19 patients, while the other half said they spent 50% or more.
To measure the health of a work environment, AACN looked at six standards:
Skilled communication
True collaboration
Effective decision-making
Meaningful recognition
Authentic leadership
Appropriate staffing
Overall, AACN found that nurses’ perceptions of quality on these six measures had declined across the board since the organization’s 2018 survey.
In particular, appropriate staffing was the lowest rated of all the standards at 2.33 out of 4, which is the lowest rating the standard has received since AACN first began the survey in 2006. Only 24% of RNs said their units had the right number of nurses with the right knowledge and skills more than 75% of the time—down from 39% who said the same in 2018.
In addition, there was a significant decline in how RNs rated the quality of care in their organizations and their units. Only 16% rated their organizations’ quality of care as excellent (compared to 24% in 2018), and 30% rated their units’ quality of care as excellent (compared to 44% in 2018). Over 50% of nurses said quality of care in their organization or unit has gotten somewhat or much worse over the last year.
Many nurses also reported difficulties with their physical and psychological well-being in the survey. For example, less than 50% of RNs said they felt their organization values their health and safety, a significant decline from 68% who said the same in 2018.
In addition, 40% of participants reported that they were not emotionally healthy. The percentage of RNs who reported experiencing moral distress also doubled from 11% in 2018 to 22% in 2021.
A significant portion of RNs also reported experiencing verbal abuse, physical abuse, sexual harassment, or discrimination over the past year. Of the 7,399 RNs who answered this question, 72% said they had experienced at least one negative incident, with verbal abuse being the most common at 65%, followed by physical abuse at 28%.
RN job satisfaction
Only 40% of RNs said they were “very satisfied” with their job, down from 62% who said the same in 2018. Further, a significant number of RNs in the survey reported planning to leave their jobs within the next few years.
Overall, 67% of RNs said they planned to leave their current position within the next three years, compared to 54% in 2018. Of this group, 36% said they planned to leave within the next year, with 20% planning to leave within the next six months.
According to the respondents, the top factors that could lead them to reconsider their decision to leave their job were a higher salary and more benefits (63%), better staffing (57%), and more respect from administration (50%).
“Without improvements in the work environment, the results of this study indicate that nurses will continue to exit the workforce in search of more meaningful, rewarding, and sustainable work,” the survey’s authors wrote. “It is time for bold action, and this study shows the way.” (Firth, MedPage Today, 8/3; Ulrich et al., Critical Care Nurse, 8/1)
Hard truths on the current and future state of the nursing workforce
Concerns about an imbalance in supply and demand in the nursing workforce have been around for years. The number of nursing professionals nationally may be healthy, but many nurses are not in the local areas, sites of care, or roles where they’re needed most. And many of today’s nurses don’t have the specialized skills they need, widening the existing gap between nurse experience and job complexity.
As a result, gaping holes in staffing rosters, prolonged vacancies, unstable turnover rates, and unchecked use of premium labor are now common.
Health care leaders need to confront today’s challenges in the nursing workforce differently than past cyclical shortages. In this report, we present six hard truths about the nursing workforce. Then, we detail tactics for how leaders can successfully address these challenges—stabilizing the nursing workforce in the short term and preparing it for the future.
The rise of ubiquitous self-testing and the paucity of accurate, timely data from the CDC on COVID numbers has left us feeling our way in the dark in terms of the current state of the pandemic. Clearly there’s a new surge underway, driven by the BA.5 variant. What we can report from our experiences on the road over the past few weeks is that the wave is significant.
We’re hearing from our health system members that inpatient COVID volumes and COVID-related ED visits are significantly up again—often double or more what they were just two months ago, although still well below levels of past surges. Length of stay for COVID inpatients is shorter, with fewer ICU visits than during the Delta surge—about the same intensity, proportionally, as during Omicron.
But COVID-related staffing shortages are once again having a real impact on hospitals’ ability to deliver care—clinical and non-clinical staff callouts are at high levels again, as during Omicron.
One piece of good news: masking is back in vogue among many health system executive teams, likely in response to a number of “superspreader” events: gatherings of hospital staff over the past few weeks that resulted in clusters of cases. One system described an all-hands session for anesthesiologists that resulted in more than a dozen cases across the next week—forcing the hospital to cancel procedures.
We’re worried that this BA.5 surge is just getting started, and with booster uptake stagnating and masking all but nonexistent in the general population, the late summer and early autumn situation could be significantly worse.
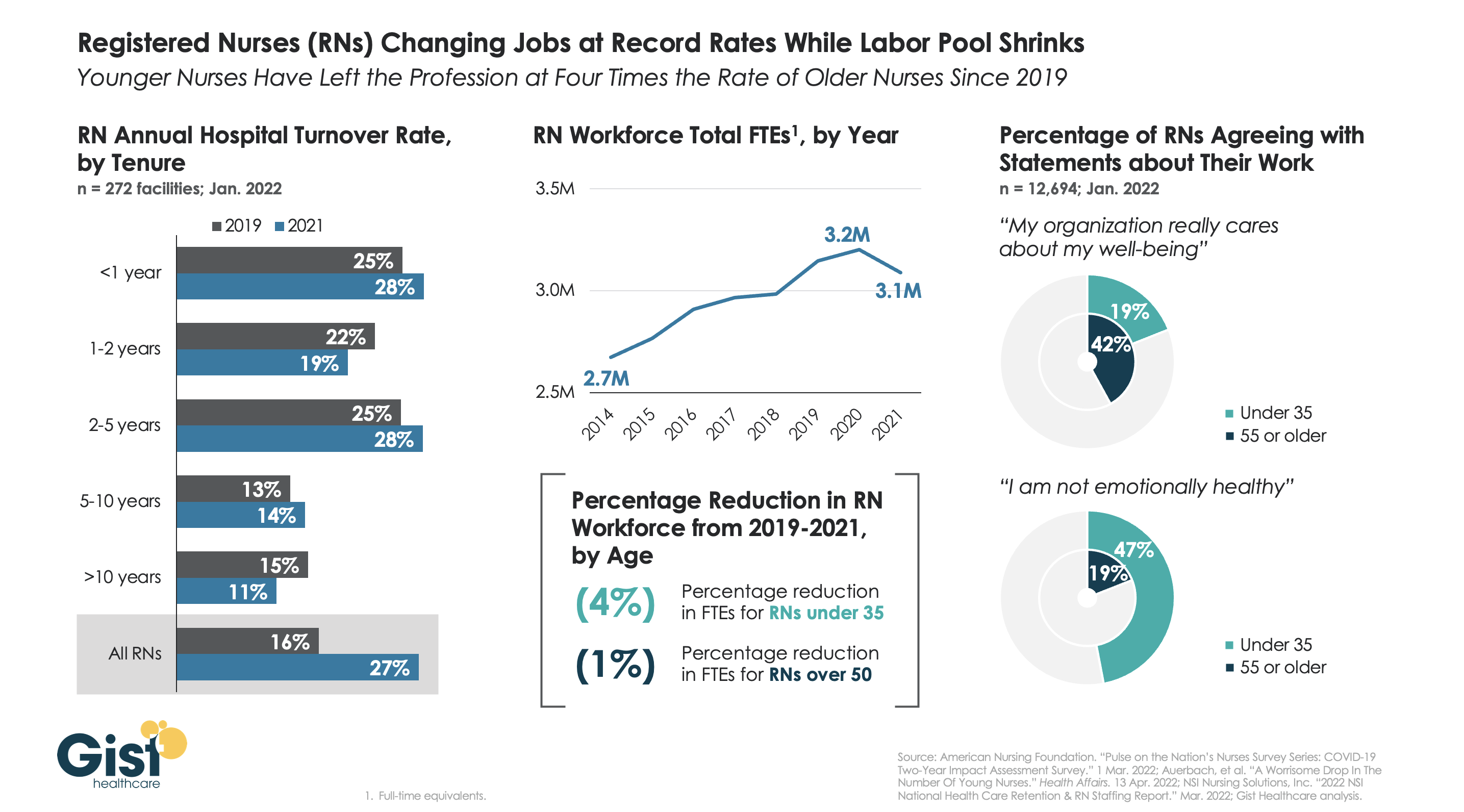
The prevailing opinion earlier this year was that the hospital registered nurse (RN) shortage was being driven by older nurses retiring early or leaving hospital employment for less-demanding care settings during the pandemic. However, recent data shown in the graphic below paint a different picture.
Hospital RNs with over ten years of tenure actually turned over at lower rates in 2021, compared to 2019. Meanwhile, the turnover rate for nurses with less tenure (who are typically younger) increased in 2021. While less-tenured nurses have always turned over at higher rates, we are seeing a new uptick in younger RNs leaving the profession.
The size of the total RN workforce decreased by 1.8 percent between 2019 and 2021—and the decline was twice as steep for hospital-employed RNs. Younger RNs disproportionately drove this decline: nurses under age 35 left the nursing workforce at four times the rate of those over age 50.
A recent survey suggestsyounger RNs are less likely to feel their well-being is supported by their organization, and more likely to define themselves as “emotionally unhealthy.” To keep younger nurses in the profession, hospitals must increase the support available to them. Investments might include expanding preceptorship and mentorship programs, many of which were cut during the pandemic, and increasing behavioral health support and job flexibility.
The popularity of travel nursing is leaving healthcare facilities and the companies serving them susceptible to misclassification accusations and joint-employer disputes, Bloomberg Law reported June 14.
Providers should read contracts to understand who is liable if a travel nurse sues a healthcare facility and staffing company, according to the report. Even if agreements state that a hospital is not a temporary employee’s employer, courts may decide it’s a joint employer. If they are a joint employer, they may have to pay legal fees if a staffing agency is sued.
If classified as an employer, healthcare facilities may be bound by labor laws that didn’t apply to independent contractors. In California, for example, employers are required to pay part of a worker’s cell phone bill if a phone is needed for the job.
“Given the already serious issues with many of these healthcare workers feeling overwhelmed and underpaid, they’re going to turn these questions not just to the individual hospitals, but potentially also to the companies that are hosting these platforms,” Sonya Rosenberg, a labor and employment partner at Neal Gerber Eisenberg, told Bloomberg Law.
Hospitals’ labor costs rose by more than a third from pre-pandemic levels by March 2022, according to a report out Wednesday from Kaufman Hall.
Heightened temporary and traveling labor costs were a main contributor, with contract labor accounting for 11% of hospitals’ total labor expenses in 2022 compared to 2% in 2019, the report found.
Contract nurses’ median hourly wages rose 106% over the period, from $64 an hour to $132 an hour, while employed nurse wages increased 11%, from $35 an hour to $39 an hour, the report found.
Dive Insight:
The new data from Kaufman Hall supports concerns hospital executives expressed while releasing first quarter earnings results, as higher-than expected labor costs spurred some operators, like HCA, to lower their financial full-year guidance.
The ongoing use of contract labor amid shortages driven by heightened turnover was a key factor executives cited for higher costs, and follows the findings from Kaufman Hall’s latest report.
More than a third of nurses surveyed by staffing firm Incredible Health said they plan to leave their current jobs by the end of this year, according to a March report. While burnout is driving them to leave, higher salaries are the top motivating factor for taking other positions, that report found.
Kaufman Hall’s report, which analyzes data from more than 900 hospitals across the country, found hospitals spent $5,494 in labor expenses per adjusted discharge in March compared to $4,009 roughly three years ago.
Costs rose for hospitals in every region, though the South and West experienced the largest increases from pre-pandemic levels as those expenses rose 43% and 42%, respectively.
The West and Northeast/Mid-Atlantic regions saw the highest expenses consistently from 2019 to 2022, according to the report.
“The pandemic made longstanding labor challenges in the healthcare sector much worse, making it far more expensive to care for hospitalized patients over the past two years,” said Erik Swanson, senior vice president of data and analytics at Kaufman Hall.
“Hospitals now face a number of pressures to attract and retain affordable clinical staff, maintain patient safety, deliver quality services and increase their efficiency,” Swanson said.
The report also notes that hospitals are competing with non-hospital employers also pursuing hourly staff, though those companies can pass along wage increases to consumers through higher prices “in a way healthcare organizations cannot,” the report said.
Some hospitals, like HCA Healthcare and Universal Health Services, are looking to raise prices for health plans amid rising nurse salaries, according to reporting from The Wall Street Journal.
Another recent report from group purchasing organization Premier found the CMS underestimated hospital labor spending when making payment adjustments for the 2022 fiscal year, resulting in hospitals receiving only a 2.4% rate increase compared to a 6.5% increase in hospital labor rates.
To match the rates hospitals are now paying staff, an adequate inpatient payment update for fiscal 2023 is needed, that report said.
The CMS proposed its IPPS rule for FY 2023 on April 18 that includes a 3.2% hike to inpatient hospital payments, which provider groups like the American Hospital Association rebuked as “simply unacceptable” considering inflation and rising hospital labor costs.