The U.S. Supreme Court is set to hear a case questioning the legality of the ACA on Nov. 10.
Five things to know:
1. At the center of the case is whether the health law should be struck down. In a brief filed June 25 in Texas v. United States, the Trump administration argues the entire ACA is invalid because in December 2017, Congress eliminated the ACA’s tax penalty for failing to purchase health insurance. The administration argues the individual mandate is inseverable from the rest of the law and became unconstitutional when the tax penalty was eliminated; therefore, the entire health law should be struck down.
2. The administration’s brief was filed in support of a group of Republican-led states seeking to undo the ACA. Meanwhile, California Attorney General Xavier Becerra is leading a coalition of more Democratic states to defend the ACA before the Supreme Court.
3. The case goes before the Supreme Court days after media outlets projected Joe Biden as the next president of the U.S. President-elect Biden has said he seeks to expand government-subsidized insurance coverage and wants to the bring back the ACA’s tax penalty for failing to purchase health insurance, according to The Wall Street Journal. If a change regarding the tax penalty did occur, the publication notes that Republicans’ argument on severability would no longer apply.
4. The case also goes before the Supreme Court about two weeks after the Senate voted Oct. 26 to confirm Amy Coney Barrett to the Supreme Court. Ms. Barrett previously criticized Chief Justice John Roberts’ 2012 opinion sustaining the law’s individual mandate, The New York Times reported, but she said during her confirmation hearings in October that “the issue in the case is this doctrine of severability, and that’s not something that I have ever talked about with respect to the Affordable Care Act.”
5. According to the Journal, the Supreme Court is not expected to make a decision in the case until the end of June.
In swing states from Georgia to Arizona, the Affordable Care Act — and concerns over protecting preexisting conditions — loom over key races for Congress and the presidency.
“I can’t even believe it’s in jeopardy,” says Noshin Rafieei, a 36-year-old from Phoenix. “The people that are trying to eliminate the protection for individuals such as myself with preexisting conditions, they must not understand what it’s like.”
In 2016, Rafieei was diagnosed with colon cancer. A year later, her doctor discovered it had spread to her liver.
“I was taking oral chemo, morning and night — just imagine that’s your breakfast, essentially, and your dinner,” Rafieei says.
In February, she underwent a liver transplant.
Rafieei does have health insurance now through her employer, but she fears whether her medical history could disqualify her from getting care in the future.
“I had to pray that my insurance would approve of my transplant just in the nick of time,” she says. “I had that Stage 4 label attached to my name and that has dollar signs. Who wants to invest in someone with Stage 4?”
“That is no way to feel,” she adds.
After doing her research, Rafieei says she intends to vote for Joe Biden, who helped get the ACA passed in this first place.
“Health care for me is just the driving factor,” she says.
Even 10 years after the Affordable Care Act locked in a health care protection that Americans now overwhelmingly support — guarantees that insurers cannot deny coverage or charge more based on preexisting medical conditions — voters once again face contradicting campaign promises over which candidate will preserve the law’s legacy.
A majority of Democrats, independents and Republicans say they want their new president to preserve the ACA’s provision that protects as many as 135 million people from potentially being unable to get health care because of their medical history.
President Trump has pledged to keep this in place, even as his administration heads to the U.S Supreme Court the week after Election Day to argue the entire law should be struck down.
“We’ll always protect people with preexisting,” Trump said in the most recent debate. “I’d like to terminate Obamacare, come up with a brand new, beautiful health care.”
And yet the Trump administration has not unveiled a health care plan or identified any specific components it might include. In 2017, the administration joined with congressional Republicans to dismantle the Affordable Care Act, but none of the GOP-backed replacement plans could summon enough votes. The Republicans’ final attempt, a limited “skinny repeal” of parts of the ACA, failed in the Senate because of resistance within their own party.
In an attempt to reassure wary voters, Trump recently signed an executive order that asserts protections for preexisting conditions will stay in place, but legal experts say this has no teeth.
“It’s basically a pinky promise, but it doesn’t have teeth,” says Swapna Reddy, a clinical assistant professor at Arizona State University’s College of Health Solutions. “What is the enforceability? The order really doesn’t have any effect because it can’t regulate the insurance industry.”
Since the 2017 repeal and replace efforts, the health care law has continued to gain popularity.
Public approval is now at an all-time high, but polling shows many Republicans still don’t view the ACA as synonymous with its most popular provision — protections for preexisting conditions.
Democrats hope to change that.
“If you have a preexisting condition — heart disease, diabetes, breast cancer — they are coming for you,” said Biden’s running mate, California Sen. Kamala Harris, during her recent debate with Vice President Pence.
Voters support maintaining ACA’s legal protections
In key swing states, many voters say protecting preexisting conditions is their top health concern.
Rafieei, the Phoenix woman with colon cancer, still often has problems getting her treatments covered. Her insurance has denied medications that help quell the painful side effects of chemotherapy or complications related to her transplant.
“During those chemo days, I’d think, wow, I’m really sick, and I just got off the phone with my pharmacy and they’re denying me something that could possibly help me,” she says.
Because of her transplant, she will be on medication for the rest of her life, and sometimes she even has nightmares about being away and running out of it.
“I will have these panic attacks like, ‘Where’s my medicine? Oh my god, I have to get back to get my medicine?'”
Election season and talk of eliminating the ACA has not given Rafieei much reassurance, though.
“I cannot stomach politics. I am beyond terrified,” she says.
And yet she plans to head to the polls — in person — despite having a compromised immune system.
“It might be a long day. But you know what? I want to fix whatever I can,” she says.
A few days after she votes, she’ll get a coronavirus test and go in for another round of surgery.
A key health issue in political swing states
Rafieei’s home state of Arizona is emblematic of the political contradictions around the health care law.
The Republican-led state reaped the benefits of the ACA. Arizona’s uninsured rate dropped considerably since 2010, in part because it expanded Medicaid.
But the state’s governor also embraced the Republican effort to repeal and replace the law in 2017, and now Arizona’s attorney general is part of the lawsuit that will be heard by the Supreme Court on Nov. 10 that could topple the entire law.
Depending on how the Supreme Court rules, ASU’s Reddy says any meaningful replacement for preexisting conditions would involve Congress and the next president.
“At the moment, we have absolutely no national replacement plan,” she says.
Meanwhile, some states have passed their own laws to maintain protections for preexisting conditions, in the event the ACA is struck down. But Reddy says those vary considerably from state to state.
For example, Arizona’s law, passed just earlier this year, only prevents insurers from outright denying coverage — consumers with preexisting conditions can be charged more.
“We are in this season of chaos around the Affordable Care Act,” says Reddy. “From a consumer perspective, it’s really hard to decipher all these details.”
As in the congressional midterm election of 2018, Democrats are hammering away at Republican’s track record on preexisting conditions and the ACA.
In Arizona, Mark Kelly, the Democratic candidate running for Senate, has run ads and used every opportunity to remind voters of Republican Sen. Martha McSally’s votes to repeal the law.
In Georgia, Democratic challenger Jon Ossoff has taken a similar approach.
“Can you look down the camera and tell the people of this state why you voted four times to allow insurance companies to deny us health care coverage because we may suffer from diabetes or heart disease or have cancer in remission?” Ossoff said during a debate with his opponent, Republican Sen. David Purdue.
Republicans have often tried to skirt health care as a major issue this election cycle because there isn’t the same political advantage to pushing the repeal and replace argument, says Mark Peterson, a professor of public policy, political science and law at UCLA.
“It’s political suicide, there doesn’t seem to be any real political advantage anymore,” says Peterson.
But the timing of the Supreme Court case — exactly a week after election day — has somewhat obscured the issue for voters.
Republicans have chipped away at the health care law by reducing the individual mandate — the provision requiring consumers to purchase insurance — to zero dollars.
The premise of the Supreme Court case is that the ACA no longer qualifies as a tax because of this change in the penalty.
“It is an extraordinary stretch, even among many conservative legal scholars, to say that the entire law is predicated on the existence of an enforced individual mandate,” says Peterson.
The court could rule in a very limited way that does not disrupt the entire law or protections for preexisting conditions, he says.
Like many issues this election, Peterson says there is a big disconnect between what voters in the two parties believe is at stake with the ACA.
“Not everybody, particularly Republicans, associates the ACA with protecting preexisting conditions,” he says. “But it is pretty striking that overwhelmingly Democrats and Independents do — and a number of Republicans — that’s enough to give a significant national supermajority.”
Since the Affordable Care Act (ACA) was signed into law a little more than a decade ago, it has fundamentally reshaped the American healthcare system. As the graphic below highlights, the far-reaching law expanded insurance coverage, increased consumer protections, led to new payment models, established minimum coverage standards, reformed the Indian Health Service—and even gave us calorie counts on menus, among myriad other things.
The fate of the ACA is once again in the Supreme Court’s hands—and the nine Justices, now including Amy Coney Barrett, are scheduled to hear arguments starting November 10th. Eighteen states with Republican leadership are asking the court to determine whether the individual mandate is constitutional without a financial penalty, and whether the mandate is severable from the rest of the law.
The process of unwinding a law that touches nearly every facet of the US healthcare system would mean a confusing and financially detrimental road ahead for many.Although we believe it’s unlikely that the entire law will be ruled unconstitutional, if it is—and no replacement legislation is passed—the effects could be devastating.
An estimated 21 million people would be at serious risk of losing their health insurance. This risk is magnified for Hispanic and Black Americans, who are also hardest hit by COVID-19. As many as 133M people with pre-existing conditions could face insurance disqualification or significantly higher premiums.
The lost coverage would result in a significant revenue hit for doctors and hospitals. While the impact would vary by state depending on Medicaid expansion terms, an Urban Institute report projects that total uncompensated care would grow an average of 78 percent for hospitals and 68 percent for physician services if the ACA is struck down. Although the Court is not expected to rule on the fate of the law until mid-2021, the direction and pace of future health reform legislation will be set by the ruling, under either a Trump or Biden administration.
Less than three months from now, either Donald Trump will begin his second term as President, or Joe Biden will begin his first. What the U.S. healthcare system on that date and moving forward could be starkly different depending on who is sworn in.
The policy differences between the two men are essentially on opposite poles. If fully enacted, Trump’s policies could potentially cause tens of millions of Americans to lose their healthcare coverage.Biden’s policies would likely provide healthcare access to tens of millions more Americans compared to today.
In November, the U.S. Supreme Court will hear arguments in a case called California v. Texas. It stems from the 2017 tax bill that zeroed out the penalty individuals paid if they did not obtain health insurance. The argument put forth by the 20 Republican state attorney generals in that case is if the individual mandate no longer has taxing power, the entire law should be declared unconstitutional based upon a lack of severability of the entire law.
Many legal scholars have noted that this case is premised on a shaky argument. But with a 6-3 majority of conservative justices now on the high court, many bets are off as to the ACA’s survival. And President Trump just said in an interview with “60 Minutes” he fervently hoped the ACA is eliminated. He put forth no alternatives to the ACA in that interview.
Should the ACA be declared unconstitutional, health insurance for some 23 million people would be imperiled. That includes some 12 million Americans who are eligible for Medicaid under the ACA’s expanded income guidelines, and another 11 million who purchase insurance on the state and federal health insurance exchanges – roughly 85% of whom receive premium subsidies that make it more affordable. Moreover, another 14 million Americans who are estimated to have lost their employer-based health plans during the COVID-19 pandemic may not have another place to turn for coverage.
Before the ACA case, the Trump administration also promoted so-called “off-exchange” health plans, and health sharing ministries. The first is often a form of short-term health insurance, the second operates as a cooperative serving those of the same religious stripe. Both offer health coverage that is potentially cheaper that what is offered on the exchanges, but both also tend to cap it at low dollar levels. Many also bar applicants for a variety of claims, such as for maternity or cancer care, or if they have pre-existing medical conditions – practices prohibited for ACA plans.
Should Trump be re-elected and the ACA survives constitutional muster, expect to see many states apply for more waivers from that law. Georgia just received approval to modestly expand Medicaid eligibility, primarily for those poor already working 80 hours or more a month. The state is also on the cusp of being able to opt out of the healthcare.gov exchange entirely and have consumers work directly with insurance brokers to purchase coverage. However, there is nothing in the pending waiver to prevent those brokers from offering stripped-down coverage without the ACA protections that the Trump administration is already promoting. There could also be more block grants to states for their Medicaid budgets, which most experts have concluded would reduce the number of enrollees in that program.
If Biden is elected and both incoming houses of Congress are also Democratic, the entire Supreme Court case can be mooted simply by reattaching a financial penalty to the individual mandate. That hasn’t been mentioned at all during the campaign, presumably because Biden does not want to discuss what would essentially be a promise to raise taxes. But it is the most direct way to skirt the risk of an adverse Supreme Court decision.
Biden’s campaign has also put forth numerous proposals to enlarge the ACA and the Medicare program. They include expanded premium subsidies for individuals and families to purchase coverage, and a public health plan option – which would allow those who live in the states that have yet to expand Medicaid to obtain coverage. Biden has also proposed a buy-in to Medicare at age 60.
The estimates are that an expanded ACA and other Biden plans could net another 20 to 25 million Americans healthcare coverage. That would leave fewer than 10 million – 2% to 3% of the population – without access to coverage. It would probably be as close to universal healthcare as the United States could get given its current political realities.
The two different approaches will either lead to a country where virtually everyone has access to healthcare coverage and services, or one where 50 million or more people could potentially be uninsured. It’s a shift that could impact a minimum of 45 million people – and that’s not even counting those who lost their coverage during the current public health crisis.
Elections have consequences. Less than three months from now, this one will determine whether the U.S. healthcare system will take one consequential path over another.
After negotiations for another stimulus package hit a dead end in Washington last week, President Donald Trump signed executive orders to extend relief in the meantime. One order, according to the president, would extend the federal eviction moratorium.
The original moratorium, included in the CARES Act, prohibited landlords or housing authorities from filing eviction actions, charging nonpayment fees or penalties or giving notice to vacate. It expired on July 24 and only applied to federally subsidized or federally backed housing.
But housing advocates are pushing back, saying Trump’s executive order to extend an eviction moratorium actually does nothing at all—and keeps struggling Americans at risk of losing their housing.
Details on the Order
Trump’s order doesn’t actually extend the federal eviction moratorium. Instead, it calls on the Department of Health and Human Services and the Centers for Disease Control and Prevention to “consider” whether an additional eviction ban is needed.
“The Secretary of Health and Human Services and the Director of CDC shall consider whether any measures temporarily halting residential evictions of any tenants for failure to pay rent are reasonably necessary to prevent the further spread of COVID-19 from one State or possession into any other State or possession,” reads the order.
Additionally, the executive order does not provide any new money to help struggling renters during the pandemic. Instead, it says the secretary of Treasury and the secretary of Housing and Urban Development—Steven Mnuchin and Ben Carson, respectively—can identify “any and all available federal funds” to provide temporary rental assistance to renters and homeowners who are facing financial hardships caused by COVID-19.
During a White House press briefing on Monday, Kayleigh McEnany said the president did “did what he can within his executive capacity…to prevent resident evictions.”At the time of publishing, officials mentioned in Trump’s executive order have not released guidelines on extending the federal eviction moratorium.
Housing Advocates React to Trump’s Eviction Order
Housing advocates have not reacted positively to Trump’s executive order, suggesting officials extend an eviction moratorium.
“The executive order that he signed this weekend is really nothing more than an empty shell that creates chaos and confusion, and it offers nothing more than false hope to renters who are at risk of eviction because that executive order does literally nothing to prevent or stop evictions,” Diane Yentel, president and CEO of the National Low Income Housing Coalition, said on Sunday during an MSNBC interview.
The House of Representatives included a more thorough plan to prevent evictions in its HEROES Act proposal. The proposal included $175 billion in rent and mortgage assistance and would replace the original federal eviction moratorium with a 12-month moratorium from all rental housing, not just federally subsidized ones. There also would be funds available to provide homeowners with assistance to cover mortgage and utility payments, property taxes or other resources to help keep Americans housed.
Sen. Richard Shelby (R-AL) introduced the Coronavirus Response Additional Supplemental Appropriations Act as part of the GOP’s HEALS Act proposal. Shelby’s bill included significantly less money for housing assistance than the HEROES Act—$3.2 billion—and would be used for tenant-based rental assistance. Shelby’s proposal did not include any language about extending the CARES Act eviction moratorium.
A recent report by a group of housing advocates finds there could be as much as 40 million renters at risk of eviction in the coming months. The U.S. unemployment rate currently sits at 10.2%.
Individuals who are struggling to pay rent might have assistance options available. Some cities and states have implemented their own eviction moratoriums—you can learn more about them by visiting the Eviction Lab at Princeton University. There are also legal aid options, like Just Shelter, that will help tenants who are facing eviction for low-cost or free.
One in every five workers is now collecting unemployment benefits as the country struggles to get the COVID-19 outbreak under control. A recent Families USA study estimates a quarter of the 21.9M workers that were furloughed or laid off between February and May lost their health insurance. And the payer mix will continue to change as the pandemic wears on.
The graphic below highlights a study from consultancy Oliver Wyman, looking at the impact of rising unemployment (at 15, 20 and 30 percent) on insurance coverage. With each five to ten percent rise in unemployment, the commercially insured population decreases by three to five percent. Those who lose employer-sponsored insurance either remain uninsured, buy coverage on the Obamacare marketplaces, or qualify for Medicaid.
Surprisingly, Washington State and California are reporting little to no enrollment growth in Medicaid programs thus far. Experts point to lack of outreach and consumer awareness as key contributors to the slow growth—but Medicaid enrollment will likely begin to rise quickly in coming months as temporary furloughs convert to more permanent layoffs.
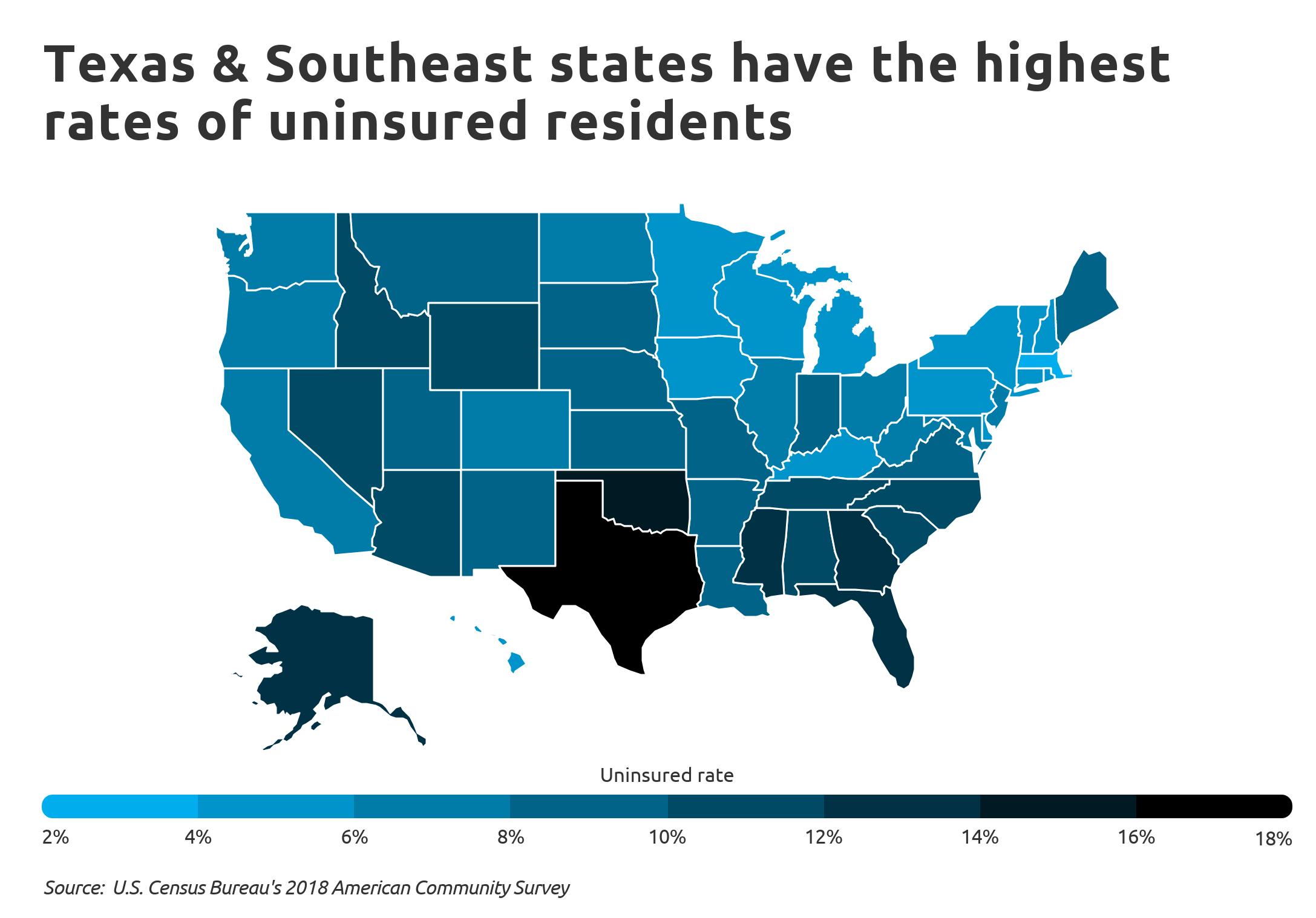
The right side of the graphic spotlights the growing number of uninsured individuals in those states with the highest uninsured rates. The previous record for the largest increase in uninsured adults was between 2008 and 2009, when nearly 4M lost coverage.The current pandemic-driven increase has crushed that record by 39 percent.
On average, states are seeing uninsured populations increase by two percent, with some as high as five percent. And the two states with the highest uninsured rates, Florida and Texas, are also dealing with the largest surge in COVID-19 cases and deaths. The ranks of the uninsured will continue to climb as states reimpose shutdowns, government assistance ends, and layoffs grow.
Texas has the highest uninsured rate in the U.S., with 29 percent of adults uninsured as of May, according to a report from Families USA.
The report compared uninsured rates in 2018 to rates in May 2020 using data from the U.S. Bureau of Labor Statistics and the Urban Institute. Every state saw an increase in the number of uninsured, and the total number of uninsured in the U.S. climbed 21 percent.
The increase was due in part to layoffs tied to the COVID-19 pandemic in recent months. Nearly 5.4 million Americans lost health insurance coverage from February to May of this year due to job losses, according to the report.
Below is the total percentage of all uninsured adults in each state and the District of Columbia as of May.
Roughly 5.4 million adults in the U.S. lost their health insurance from February to May after losing their jobs, according to a new estimate from Families USA, a group that favors the Affordable Care Act.
Why it matters: There are more adults under 65 without insurance in Southern states, which are the same states setting new records for single-day coronavirus infections along with risinghospitalizations, Axios’ Orion Rummler writes.
What they found: 3.9 million adults lost health insurance over one year during the Great Recession, per Families USA’s analysis. It only took four months in this current crisis for an estimated 5.4 million Americans to lose health insurance.
More than 20% of adults in Georgia, Florida, South Carolina, North Carolina, Mississippi, Oklahoma and Texas were without insurance as of May.
All of these states have set new records in the past two weeks for their highest number of coronavirus infections in a single day, per data from the COVID Tracking Project.
46% of adults who lost coverage due to the pandemic came from five states: Florida, New York, Texas, California and North Carolina.
The backdrop: 21 million Americans were unemployed in May, according to the Bureau of Labor Statistics’ nonfarm payrolls report.
One in seven adults worldwide struggle to afford food, shelter with no help
At least some percentage in every country is “highly vulnerable”
Highly vulnerable in developed, developing world as likely to have health problems
This article is the first in series based on results from Gallup’s new Basic Needs Vulnerability Index.
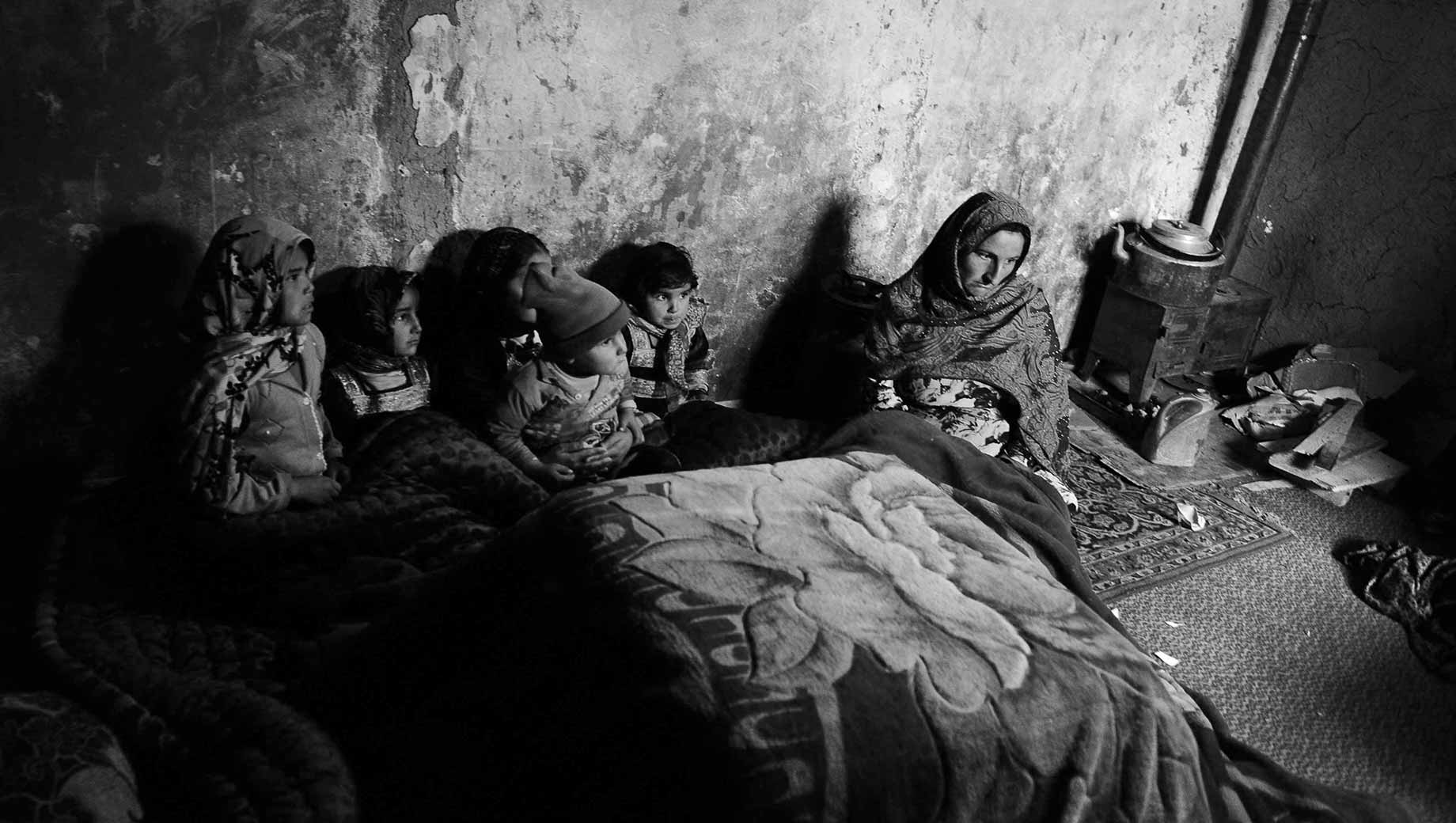
Imagine being unable to afford food or to put a roof over your head, or maybe you are struggling to do both. On top of this, you don’t have family or friends who can help you.
Now, imagine this is all happening and a pandemic hits.
Gallup’s new Basic Needs Vulnerability Index, based on surveys in 142 countries in 2019, suggests this was the reality for hundreds of millions worldwide just as COVID-19 arrived.
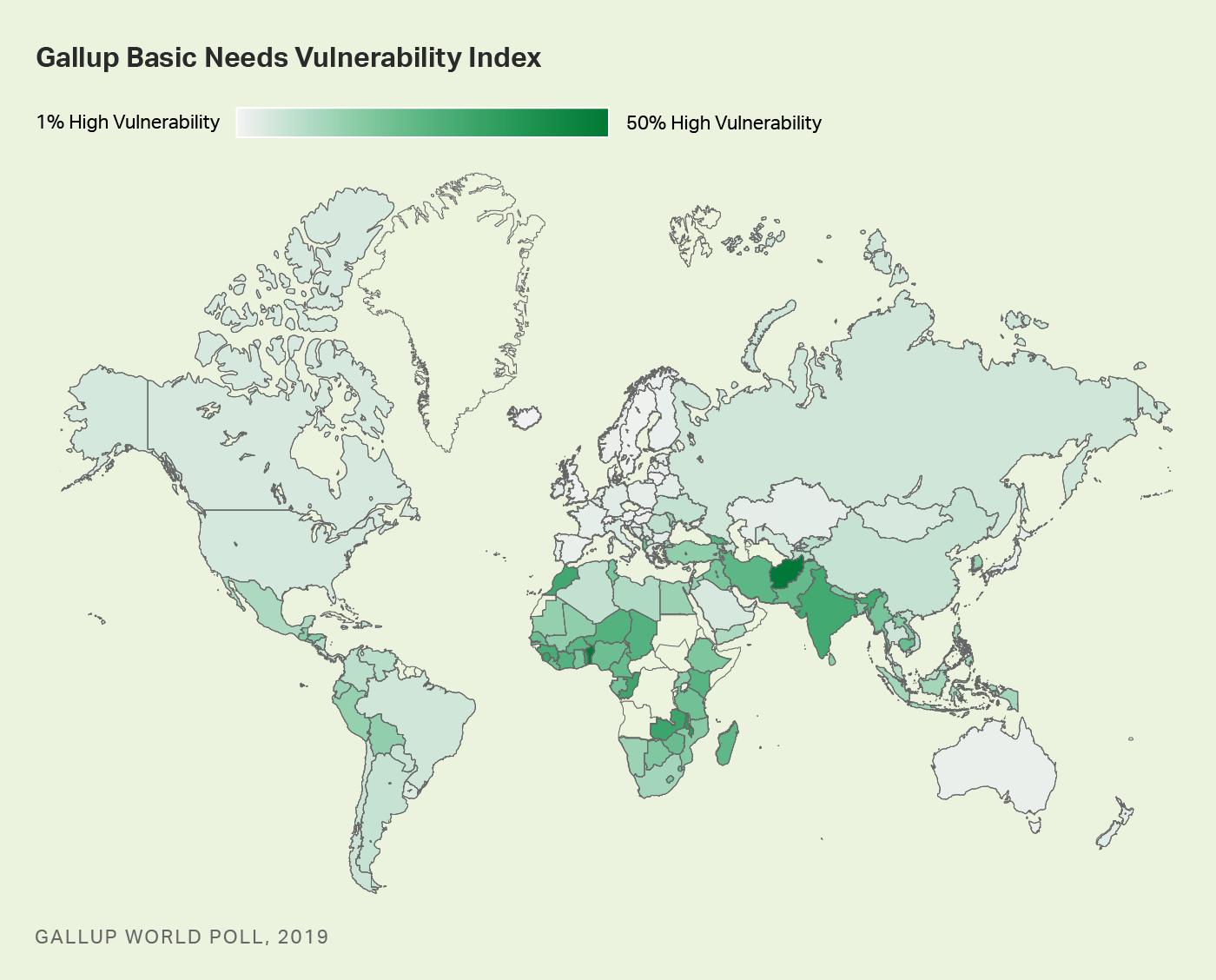
About one in seven of the world’s adults — or about 750 million people — fall into this index’s “High Vulnerability” group, which means they are struggling to afford either food or shelter, or struggling to afford both, and don’t have friends or family to count on if they were in trouble.
Globally, at least some adults in every country fall into the High Vulnerability group, which is important because Gallup finds people in this group are potentially more at risk in almost every area of their lives. Worldwide, these percentages range from 1% in wealthy countries such as Denmark and Singapore to roughly 50% in places such as Benin and Afghanistan.
Gallup’s Basic Needs Vulnerability Index gauges people’s potential exposure to risk from economic and other types of shocks like a pandemic. Beyond measuring people’s ability to afford food and shelter, this index also folds in whether people have personal safety nets — people who can help them when they are in trouble.
People worldwide fall into one of three groups:
High Vulnerability: People in this group say there were times in the past year when they were unable to afford food or shelter or say they struggled to afford both and say they do not have family or friends who could help them in times of trouble.
Moderate Vulnerability: People in this group say there were times in the past year when they were unable to afford food or shelter or say they struggled to afford both, and they do have family or friends to help them in times of trouble.
Low Vulnerability: People in this group say there were not times in the past year when they struggled to afford food or shelter and say they do have family or friends to help them if they were in trouble.
Before the pandemic, most of the world was at least moderately vulnerable, falling into either the High Vulnerability group (14%) or the Moderate Vulnerability group (39%). The rest, 47%, fell into the Low Vulnerability group.
The life experiences in these three groups illustrate the difference that not having family and friends to count on in times of trouble can make in people’s lives.
Highly Vulnerable Most Likely to Experience Health Problems, Experience Pain
While people in the High Vulnerability group are potentially more at risk in almost every area of their lives than those in the other two groups, they are particularly at risk when it comes to their health.
More than four in 10 (41%) of the highly vulnerable say they have health problems that keep them from doing activities that people their age normally do. This percentage drops to 29% among those who are moderately vulnerable and to 14% among those with low vulnerability.
The same is true for experiences of physical pain. The highly vulnerable are also far more likely to say they experienced physical pain the day before the interview (53% have) compared with 37% in the moderately vulnerable and 20% in the lowest vulnerability group.
Looking at who the highly vulnerable are within the global population reinforces why the greater risks to their health are so important. Globally, people in the high vulnerability group are just as likely to be male or female (14% of each fall into this group), and percentages are similar in the 15 to 29 age group (12%) and 60 and older group (14%).
However, the highly vulnerable are more likely to live in rural (16%) rather than urban areas (10%) and be in the poorest 20% of the population (21%) than the richest 20% of the population (7%).
Highly Vulnerable in Developed and Developing Countries Poor Health in Common
As might be expected, most of the countries with the highest percentage in the High Vulnerability group are a mix of developing economies and notably one emerging economy — India — and the countries with the lowest percentage are developed, high-income economies.
However, regardless of where they are located or their level of development, the highly vulnerable populations look a lot alike. In fact, when it comes to health problems, among the highly vulnerable populations, almost the exact same percentage in developing economies (41%) and high-income economies (42%) report having them.
The highly vulnerable in developing countries are only slightly more likely to report experiencing physical pain (53%) than this group in developed, high-income economies (47%).
Implications
As massive as the highly vulnerable group was before the pandemic, it could have been even larger, taking children and other household members into account.
As such, this new layer of vulnerability among populations will be important to monitor as the pandemic threatens to push tens of millions more people into extreme poverty and hunger this year and beyond.
Lucy Dadayan of the Urban-Brookings Tax Policy Center breaks down the good, the bad and the ugly of the fiscal crisis facing states as the coronavirus pandemic crushes revenues and raises costs.
“Prior to the onset of the COVID-19 pandemic, most states were generating solid revenue growth. And many built up robust rainy day funds. But the pandemic has largely wiped out earlier revenue gains and most states now anticipate substantial revenue shortfalls for the current fiscal year and for fiscal year 2021,” she writes.
The good: Preliminary April tax revenue data show a steep drop in estimated and final annual tax payments as the tax-filing deadline got pushed back from April 15 to July 15. But taxes withheld from paychecks grew in 17 states compared to April 2019. “Tax withholding is usually a better indicator of the current strength of the economy and of the path for personal income tax revenue because it comes largely from current wages,” Dadayen explains. On the other hand, 16 states reported declines of less than 10%, while five states posted double-digits drops, so the bright spots are limited.
The bad: “Declines in sales tax revenues have been fast, steep, and widespread across the states,” Dadayen writes. How steep? April sales tax revenues fell by 16% across 42 states for which the Tax Policy Center has complete data. Twenty-three states reported double-digit declines, while just five states reported year-over-year growth. And since the April data mostly reflect March sales, the May numbers are likely to be even worse.
The ugly: For the fiscal year so far, total state tax revenue has fallen sharply — and next year is expected to be worse. “With two months remaining in the fiscal year for 46 states, total state tax revenues are now down about $57 billion, compared to last year,” Dadayen writes.
After the sharp pandemic-related plunge in April, tax revenues have fallen in 34 states compared to 2019 and risen in 12. (NewYork, the state hit hardest by the virus, is surprisingly among those dozen, but Dadayen says that’s only because its fiscal year 2020 ended in March, so April’s devastation isn’t reflected in the data. The state reported that net taxes and fees collected in April, the first month of its new fiscal year, fell by 69% compared with April 2019.)