

Cartoon – Coronavirus Job Market
https://finance.yahoo.com/news/jobless-claims-coronavirus-unemployment-week-ended-september-5-2020-165121299.html?.tsrc=fin-notif
Another 884,000 Americans filed for first-time unemployment insurance benefits last week, matching the previous week’s level.
The U.S. Department of Labor (DOL) released its weekly jobless claims report at 8:30 a.m. ET Thursday. Here were the main metrics from the report, compared to consensus estimates compiled by Bloomberg:
Last week’s new jobless claims were upwardly revised slightly to 884,000, from the 881,000 previously reported. This marked the first time since March that jobless claims came in below 1 million for back-to-back weeks, as claims remained stubbornly elevated but off their peak from the worst point of the pandemic.
The past couple weeks of jobless claims appeared to improve considerably from the more than 1 million new weekly claims reported in mid-August. However, this was due to a technical change in the way the Labor Department made its seasonal adjustments, which applied for the first time to claims counted during the week ended August 28. Previous weeks’ claims were not revised to reflect the new counting method.
The change was made to account for the fact that the pandemic generated a far greater level of new claims per week than would typically occur over the course of a year, throwing off the Labor Department’s usual system of making adjustments for seasonal hiring trends.
Most economists agreed that the new methodology would produce a more accurate dataset on jobless claims during the pandemic period. It also produced a lower reported number of seasonally adjusted jobless claims than would have been generated under the previous method. Under the old method of seasonally adjusting claims, new jobless claims for the week ended August 29 would have risen to 1.02 million, according to an analysis by Ian Shepherdson, chief economist for Pantheon Macroeconomics.
“Interpreting the seasonally adjusted figures is complicated by a recent change in methodology, but in both an SA [seasonally adjusted] sense and an NSA [non-seasonally adjusted] sense, it looks like the trends for both initial and continuing claims filings have flattened out lately after a period with more notable declines,” JPMorgan economist Daniel Silver said in a note Thursday. “This flattening out has been evident in the initial claims data for a few months and in the continuing claims data for a few weeks and it is broadly consistent with the idea that the labor market recovery has lost momentum lately.”
Unadjusted claims have shown a clearer picture of the stalling recovery in the labor market. Last week, unadjusted new weekly jobless claims totaled 857,148, for an increase of 20,140 over the prior week. This was the fourth straight week of increases in unadjusted new claims.
Other economic indicators offered a more upbeat picture of the U.S. labor market. The Labor Department’s monthly jobs report released last Friday showed the U.S. economy added a greater-than-expected 1.371 million payrolls in August, and that the unemployment rate dipped more than anticipated to 8.4%. Wednesday morning, the JOLTS jobs report showed employers had more than 6.6 million job openings in July, topping expectations by over 600,000.




Surprise medical bills have become a major issue for Americans, but federal legislation to protect consumers continues to stall. Is Congress getting closer to halting this practice?
Listen to the full episode below, read the transcript or scroll down for more information.
Over the past two years, Congress has considered at least four bipartisan bills to protect patients from surprise charges, but all four have stalled. The proposals offer different approaches to determine how much insurers will pay out-of-network providers. These bills typically address the problem by adopting a payment standard, arbitration process or a hybrid of the two.
Insurers reimburse providers for out-of-network bills based on a set amount. Most bills propose using established in-network rates.
This process requires an insurer and provider to submit payment offers to a neutral party who makes the final call.
This approach combines the payment standard with arbitration to resolve disputes. An insurer pays a set amount, and if the provider disagrees, it can initiate arbitration.
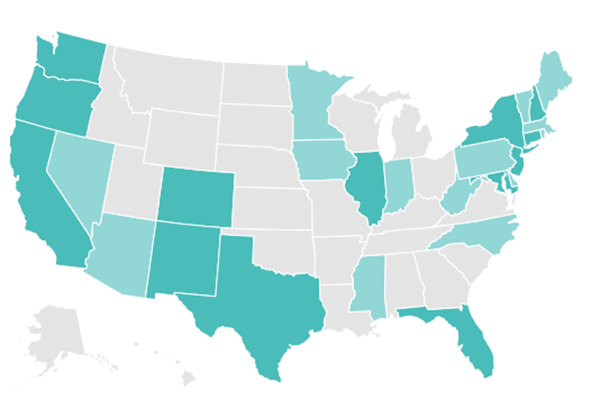
With federal solutions at a standstill, 30 states have passed varying levels of protections from surprise billing. As of July, 2020, 16 states have more comprehensive protections, which ensure that insured patients are only responsible for paying in-network costs, even when receiving care from out-of-network providers or emergency services at an out-of-network facility. Georgia was the latest state to pass such a law in July 2020. The other 14 states offer far more limited protections.
But even states with comprehensive protections cannot protect all patients from surprise medical bills. States are not able to regulate job-based coverage that falls under a federal law known as the Employee Retirement Income Security Act, which applies to most employer sponsored insurance. These patients remain vulnerable to surprise medical bills until Congress takes action to ban the practice.
Click on the map below for an interactive map from the Commonwealth Fund that details each state’s protections.
Despite strong bipartisan support for protecting patients from surprise bills, disagreement comes over how much physician groups should charge and how much insurers should pay. Essentially, resolving this issue may mean Congress has to pick sides.
As a result, stakeholders such as hospitals and private equity-backed physician groups, in particular, have pushed back on federal legislation, arguing that banning surprise billing will cripple their bottom line. These equity-backed physician groups have powerful lobbying groups, and in 2019, spent at least $5 million to persuade lawmakers to halt the legislation.
The pandemic has increased the risk that patients will unknowingly receive care from an out-of-network provider or at an out-of-network facility. The Trump administration tried to limit surprise bills for those in need of COVID-19 treatment by banning hospitals and providers that receive money from its Provider Relief Fund from sending balance bills to patients. But this approach leaves significant gaps and has had mixed success.
https://us3.campaign-archive.com/?u=6ab1fc39a0b1b15521551487c&id=6f9ac3fd86&e=ad91541e82
https://www.nejm.org/doi/full/10.1056/NEJMp2023312

This week’s contributor is Larry Levitt, the Executive Vice President for Health Policy at the Kaiser Family Foundation.
The study – by Sumit Agarwal and Benjamin Sommers, published in the New England Journal of Medicine – compares people who lost their jobs before and after the ACA went into effect in 2014 to see if there is a difference in how many people retained health insurance. During the pre-ACA period (2011-2013), there was about a 5% increase in the uninsured rate for people following a job loss. After the ACA went into effect (2014-2016), no such increase occurred. Instead, Medicaid and the marketplaces saw large increases in utilization.
If the economic crisis persists, the number of people losing job-based health insurance will climb, making the ACA’s role as a safety net more relevant than ever.

About half of Americans in the COVID-19 era fear a health-related incident could drive them into bankruptcy, according to a new survey Tuesday by Gallup and West Health.
Gallup and West Health said 50% of respondents said they’re concerned about medical bankruptcy — a 5% increase from early this year, before the pandemic. That concern rose 12 points among U.S. adults between 18 and 29 and non-White Americans.
“Dovetailing with the new health-related concerns brought on by the coronavirus outbreak is the economic catastrophe that — despite the recouping of millions of jobs since May — persists in form of 28 million people receiving some form of unemployment aid at the end of July,” Gallup wrote.
“As such, Americans’ concerns about a major health event putting them in bankruptcy, while substantial in early 2019, are likely only intensified today because of the pandemic.”
The study found that 15% of respondents said at least one person in their home currently has medical debt that will not be repaid in the next 12 months.
“Those in households earning less than $40,000 per year are more than four times as likely as those in households earning $100,000 or more to be carrying long-term medical debt (28% vs. 6%, respectively),” Gallup added. “The rate is also about twice as high among self-identified political independents (18%) and Democrats(16%) as among Republicans (8%).”
More than a quarter of adults said they’d need to borrow to pay a medical bill of just $500. Many others said they would have to go into debt.
Gallup polled more than 1,000 U.S. adults for the survey, which has a margin of error of 4 points.

Those on the front lines of the fight against the novel coronavirus worry about keeping themselves, their families and their patients safe.
This story is part of a series examining the state of healthcare six months into the public health emergency declared for COVID-19.
There’s no end in sight for the country as it grapples with another surge of COVID-19 cases.
That’s especially true for nurses seeking the reprieve of their hospitals returning to normal operations sometime this year. Many in the South and West are now treating ICUs full of COVID-19 patients they hoped would never arrive in their states, largely spared from spring’s first wave.
And like many other essential workers, those in healthcare are falling ill and dying from COVID-19. The total number of nurses stricken by the virus is still unclear, though the Centers for Disease Control and Prevention has reported 106,180 cases and 552 deaths among healthcare workers. That’s almost certainly an undercount.
National Nurses United, the country’s largest nurses union, told Healthcare Dive it has counted 165 nurse deaths from COVID-19 and an additional 1,060 healthcare worker deaths.
Safety concerns have ignited union activity among healthcare workers during the pandemic, and also given them an opportunity to punctuate labor issues that aren’t new, like nurse-patient ratios, adequate pay and racial equality.
At the same time, the hospitals they work for are facing some of their worst years yet financially, after months of delayed elective procedures and depleted volumes that analysts predict will continue through the year. Many have instituted furloughs and layoffs or other workforce reduction measures.
Healthcare Dive had in-depth conversations with three nurses to get a clearer picture of how they’re faring amid the once-in-a-century pandemic. Here’s what they said.
Elizabeth Lalasz has worked at John H. Stroger Hospital in Chicago for the past 10 years. Her hospital is a safety net facility, catering to those who are “Black, Latinx, the homeless, inmates,” Lalasz told Healthcare Dive. “People who don’t actually receive the kind of healthcare they should in this country.”
Data from the CDC show racial and ethnic minority groups are at increased risk of getting COVID-19 or experiencing severe illness, regardless of age, due to long-standing systemic health and social inequities.
CDC data reveal that Black people are five times more likely to contract the virus than white people.
This spring Lalasz treated inmates from the Cook County Jail, an epicenter in the city and also the country. “That population gradually decreased, and then we just had COVID patients, many of them Latinx families,” she said.

Once Chicago’s curve began to flatten and the hospital could take non-COVID patients, those coming in for treatment were desperately sick. They’d been delaying care for non-COVID conditions, worried a trip to the hospital could risk infection.
A Kaiser Family Foundation poll conducted in May found that 48% of Americans said they or a family member had skipped or delayed medical care because of the pandemic. And 11% said the person’s condition worsened as a result of the delayed care.
When patients do come into Lalasz’s hospital, many have “chest pain, then they also have diabetes, asthma, hypertension and obesity, it just adds up,” she said.
“So now we’re also treating people who’ve been delaying care. But after the recent southern state surges, the hospital census started going down again,” she said.
Amy Arlund works the night shift at Kaiser Fresno as an ICU nurse, which she’s done for the past two decades.
She’s also on the hospital’s infection control committee, where for years she’s fought to control the spread of clostridium difficile colitis, or C. diff., in her facility. The highly infectious disease can live on surfaces outside the body for months or sometimes years.
The measures Arlund developed to control C. diff served as her litmus test, as “the top, most stringent protocols we could adhere to,” when coronavirus patients arrived at her hospital, she told Healthcare Dive.
But when COVID-19 cases surged in northern states this spring, “it’s like all those really strict isolation protocols that prior to COVID showing up would be disciplinable offenses were gone,” Arlund said.
Widespread personal protective equipment shortages at the start of the pandemic led the CDC and the Occupational Safety and Health Administration to change their longstanding guidance on when to use N95 respirator masks, which have long been the industry standard when dealing with novel infectious diseases.
The CDC also issued guidance for N95 respirator reuse, an entirely new concept to nurses like Arlund who say those changes go against everything they learned in school.
“I think the biggest change is we always relied on science, and we have always relied heavily on infection control protocols to guide our practice,” Arlund said. “Now infection control is out of control, we can no longer rely on the information and resources we always have.”

The CDC says experts are still learning how the coronavirus spreads, though person-to-person transmission is most common, while the World Health Organization recently acknowledged that it wouldn’t rule out airborne transmission of the virus.
In Arlund’s ICU, she’s taken care of dozens of COVID positive patients and patients ruled out for coronavirus, she said. After a first wave in the beginning of April, cases dropped, but are now rising again.
Other changing guidance weighing heavily on nurses is how to effectively treat coronavirus patients.
“Are we doing remdesivir this week or are we going back to the hydroxychloroquine, or giving them convalescent plasma?”Arlund said. “Next week I’m going to be giving them some kind of lavender enema, who knows.”
Erik Andrews, a rapid response nurse at Riverside Community Hospital in California, has treated coronavirus patients since the pandemic started earlier this year. He likens ventilating them to diffusing a bomb.
“These types of procedures generate a lot of aerosols, you have to do everything in perfectly stepwise fashion, otherwise you’re going to endanger yourself and endanger your colleagues,” Andrews, who’s been at Riverside for the past 13 years, told Healthcare Dive.
He and about 600 other nurses at the hospital went on strike for 10 days this summer after a staffing agreement between the hospital and its owner, HCA Healthcare, and SEIU Local 121RN, the union representing RCH nurses, ended without a renewal.
The nurses said it would lead to too few nurses treating too many patients during a pandemic. Insufficient PPE and recycling of single-use PPE were also putting nurses and patients at risk, the union said, and another reason for the strike.
But rapidly changing guidance around PPE use and generally inconsistent information from public officials are now making the nurses at his hospital feel apathetic.
“Unfortunately I feel like in the past few weeks it’s gotten to the point where you have to remind people about putting on their respirator instead of face mask, so people haven’t gotten lax, but definitely kind of become desensitized compared to when we first started,” Andrews said.

With two children at home, Andrews slept in a trailer in his driveway for 12 weeks when he first started treating coronavirus patients. The trailer is still there, just in case, but after testing negative twice he felt he couldn’t spend any more time away from his family.
He still worries though, especially about his coworkers’ families. Some coworkers he’s known for over a decade, including one staff member who died from COVID-19 related complications.
“It’s people you know and you know that their families worry about them every day,” he said. “So to know that they’ve had to deal with that loss is pretty horrifying, and to know that could happen to my family too.”

“It’s new territory, which is why we’re taking that measured approach on rating actions,” Suzie Desai, senior director at S&P, said.
The healthcare sector has been bruised from the novel coronavirus and the effects are likely to linger for years, but the first half of 2020 has not resulted in an avalanche of hospital and health system downgrades.
At the outset of the pandemic, some hospitals warned of dire financial pressures as they burned through cash while revenue plunged. In response, the federal government unleashed $175 billion in bailout funds to help prop up the sector as providers battled the effects of the virus.
Still, across all of public finance — which includes hospitals — the second quarter saw downgrades outpacing upgrades for the first time since the second quarter of 2017.
S&P characterized the second quarter as a “historic low” for upgrades across its entire portfolio of public finance credits.
“While only partially driven by the coronavirus, the second quarter was the first since Q2 2017 with the number of downgrades surpassing upgrades and by the largest margin since Q3 2014,” according to a recent Moody’s Investors Service report.

Through the first six months of this year, Moody’s has recorded 164 downgrades throughout public finance and, more specifically, 27 downgrades among the nonprofit healthcare entities it rates.
By comparison, Fitch Ratings has recorded 14 nonprofit hospital and health system downgrades through July and just two upgrades, both of which occurred before COVID-19 hit.
“Is this a massive amount of rating changes? By no means,” Kevin Holloran, senior director of U.S. Public Finance for Fitch, said of the first half of 2020 for healthcare.
Also through July, S&P Global recorded 22 downgrades among nonprofit acute care hospitals and health systems, significantly outpacing the six healthcare upgrades recorded over the same period.
“It’s new territory, which is why we’re taking that measured approach on rating actions,” Suzie Desai, senior director at S&P, said.
Still, other parts of the economy lead healthcare in terms of downgrades. State and local governments and the housing sector are outpacing the healthcare sector in terms of downgrades, according to S&P.

Earlier this year when the pandemic hit the U.S., some made dire predictions about the novel coronavirus and its potential effect on the healthcare sector.
Reports from the ratings agencies warned of the potential for rising covenant violations and an outlook for the second quarter that would result in the “worst on record,“ one Fitch analyst said during a webinar in May.
That was likely “too broad of a brushstroke,” Holloran said. “It has not come in and wiped out the healthcare sector,” he said. He attributes that in part to the billions in financial aid that the federal government earmarked for providers.
Though, what it has revealed is the gaps between the strongest and weakest systems, and that the disparities are only likely to widen, S&P analysts said during a recent webinar.
The nonprofit hospitals and health systems pegged with a downgrade have tended to be smaller in size in terms of scale, lower-rated already and light on cash, Holloran said.
Still, some of the larger health systems were downgraded in the first half of the year by either one of the three rating agencies, including Sutter Health, Bon Secours Mercy Health, Geisinger, University of Pittsburgh Medical Center and Care New England.
“This is something that individual management of a hospital couldn’t control,” said Rick Gundling, senior vice president of Healthcare Financial Management Association, which has members from small and large organizations. “It wasn’t a bad strategy — that goes into a downgrade. This happened to everybody.”
Looking forward, some analysts say they’re more concerned about the long-term effects for hospitals and health systems that were brought on by the downturn in the economy and the virus.
One major concern is the potential shift in payer mix for providers.
As millions of people lose their job they risk losing their employer-sponsored health insurance. They may transition to another private insurer, Medicaid or go uninsured.
For providers, commercial coverage typically reimburses at higher rates than government-sponsored coverage such as Medicare and Medicaid. Treating a greater share of privately insured patients is highly prized.
If providers experience a decline in the share of their privately insured patients and see a growth in patients covered with government-sponsored plans, it’s likely to put a squeeze on margins.
The shift also poses a serious strain for states, and ultimately providers. States are facing a potential influx of Medicaid members at the same time state budgets are under tremendous financial pressure. It raises concerns about whether states will cut rates to their Medicaid programs, which ultimately affects providers.
Some states have already started to re-examine and slash rates, including Ohio.

