https://www.healthaffairs.org/do/10.1377/hblog20200529.449762/full/

The COVID-19 pandemic has transformed the landscape of ambulatory care with rapid shifts to telehealth. Well-resourced hospitals have quickly made the transition. Community health centers (CHCs), which serve more than 28 million low-income and disproportionately uninsured patients in rural and underserved urban areas of the United States, have not fared as well since ambulatory visits have disappeared, resulting in furloughs, layoffs, and more than 1,900 temporary site closures throughout the country. Government officials have taken notice, and the Coronavirus Aid, Relief, and Economic Security (CARES) Act infused $1.32 billion toward COVID-19 response and maintaining CHC capacity.
Many states have directed insurers to temporarily cover COVID-19-related services via telehealth while mandating parity of reimbursement for telehealth visits with in-person visits for their Medicaid program.
Preparedness Of Community Health Centers For Telehealth
Despite the changes, many health centers may not be ready to implement high-quality telehealth. A study using 2016 data showed that only 38 percent of CHCs used any telehealth. In our review of 2018 Uniform Data System data—the most recent available—from a 100 percent sample of US CHCs, we found that our nation’s health centers are largely unprepared for this transformation.
Across the US, 56 percent of 1,330 CHCs did not have any telehealth use in 2018 (exhibit 1). Of those without telehealth use, only about one in five were in the process of actively implementing or exploring telehealth. Meanwhile, 47 percent of the centers using telehealth were doing so only with specialists such as those at referral centers, rather than with patients. Of those using telehealth, the majority (68 percent) used it to provide mental health services; fewer used it for primary care (30 percent) or management of chronic conditions (21 percent), suggesting that most CHCs with telehealth capabilities prior to COVID-19 were not using it for the most frequent types of services provided at CHCs.
CHCs not using telehealth reported several barriers to implementation (exhibit 2). Thirty-six percent cited lack of reimbursement, 23 percent lacked funding for equipment, and 21 percent lacked training for providing telehealth. Although most barriers were similar in both urban and rural regions, a greater proportion of rural clinics compared to urban clinics (18 percent versus 7 percent) reported inadequate broadband services as an issue.
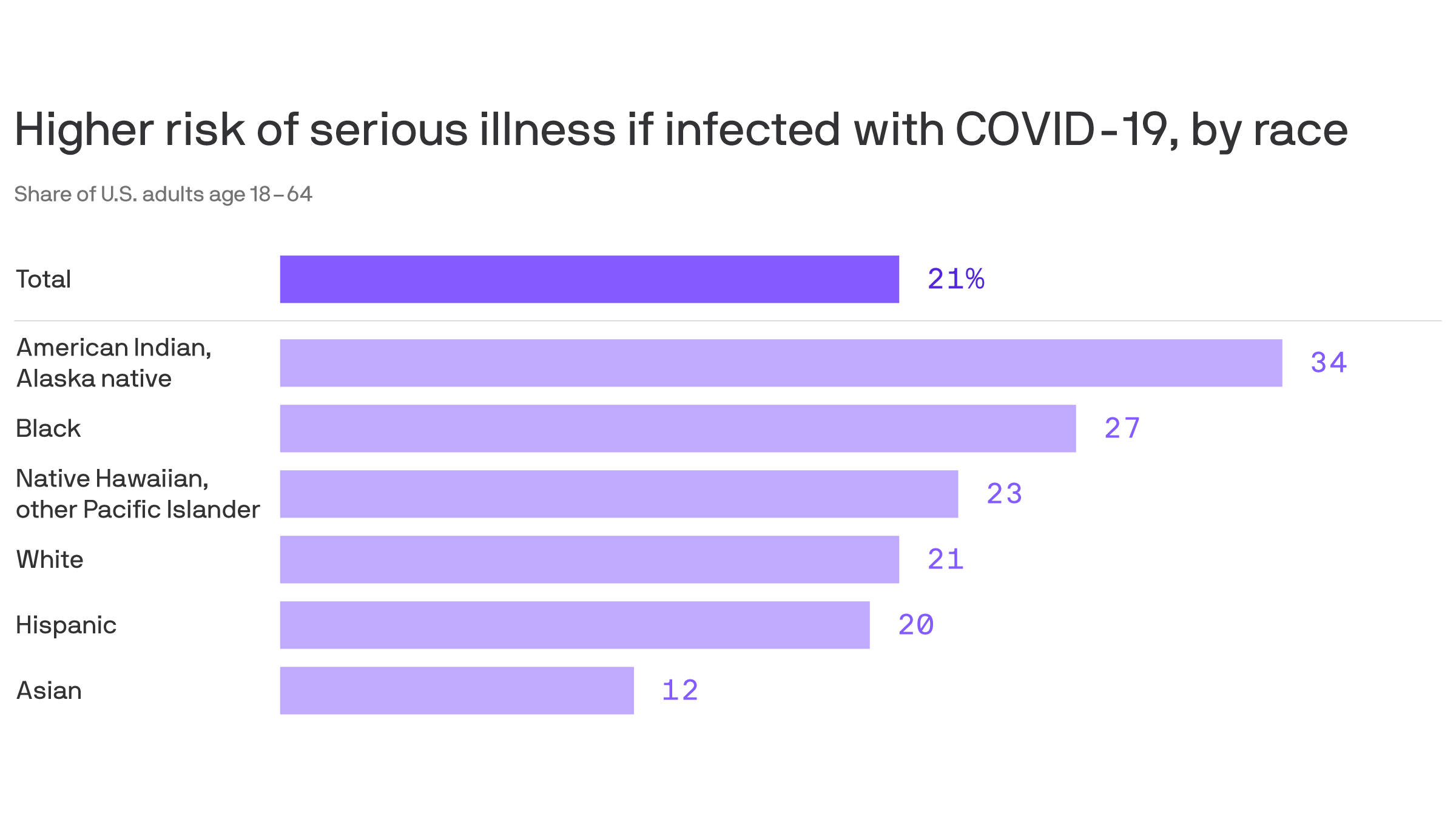
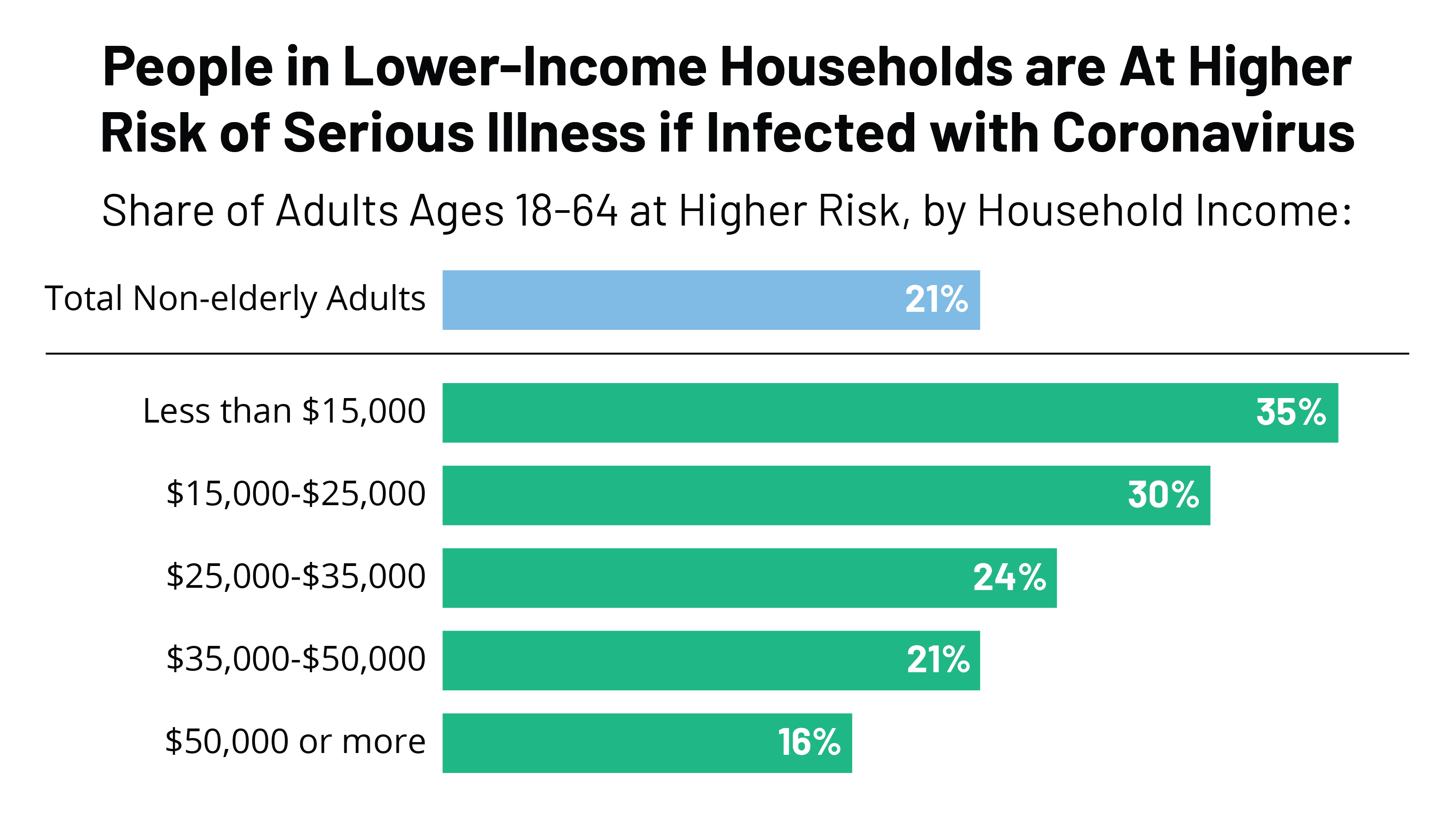
The COVID-19 pandemic has laid bare the enormous disparities in telehealth capacity. Without adequate telehealth capacity and support, many CHCs will be left without means of providing the continuous preventive and chronic disease care that can keep communities healthy and out of the hospital. During the crisis, the Health Resources and Services Administration estimates that CHCs have seen 57 percent of the number of weekly visits compared to pre-COVID-19 visit rates, 51 percent of which have been conducted virtually, suggesting that many CHC patients have forgone care that they would have otherwise received. Given CHCs serve a disproportionate share of low-income, racial/ethnic minority, and immigrant populations—populations hardest hit by the COVID-19 pandemic—any disruption to CHC capacity may exacerbate the racial disparities that have rapidly emerged.
While an important first step, policy makers cannot simply infuse more funding to CHCs and expect them to withstand the challenges of the COVID-19 era. We recommend three targeted strategies to help CHCs adapt and perhaps even thrive beyond COVID-19: legislate permanent parity in telehealth reimbursement for all insurers; allocate sufficient funding and guidance for telehealth equipment, personnel, training, and protocols; and implement telehealth systems tailored to vulnerable populations.
Permanent All-Payer Parity For Telehealth Reimbursement
Payment parity—where telehealth is reimbursed at the same level as an in-person visit—is a crucial issue that must be addressed and instituted beyond the current public health emergency. Without commensurate reimbursement for telehealth, CHCs cannot maintain patient volume or make the long-term investments necessary to remain financially viable. A “global budget” of paying CHCs a fixed payment per patient per month would give practices flexibility in how and where to treat the patient, although this may be politically and practically challenging. Meanwhile, payment parity has already been implemented and could simply be permanently codified into existing reimbursement schemes, giving providers the option to select the best mode of treatment without making financial trade-offs.
In reviewing state telehealth policies during COVID-19, all states have implemented temporary executive orders or released guidance on telehealth access—although with significant variations. At least 22 states have explicitly implemented telehealth parity for Medicaid. For Medicare, the Centers for Medicare and Medicaid Services (CMS) expanded access to telehealth beyond designated rural areas, loosened HIPAA requirements around telehealth platforms, and instituted parity in reimbursement with in-person visits.
To build on these significant steps, states should mandate telehealth parity across all payers and cover all services provided at CHCs, not just COVID-19-related care. At least 12 states have mandated all-payer parity for telehealth. Meanwhile, private insurers have individually adjusted telehealth policies on a state-by-state basis if there was no statewide mandate. Nevertheless, all payers should reimburse at parity given the patchwork quilt of insurance plans that exists at CHCs.
Furthermore, state legislatures and CMS should look to extend parity beyond the current COVID-19 emergency so that CHCs can make sustainable investments that continue to benefit patients. Even as states reopen, in-person visits are unlikely to return to their previous volume as the threat of infection continues to loom. Temporary measures should be made permanent so that CHCs can make sustainable investments that continue to benefit patients.
Funding And Guidance For Equipment, Personnel, Training, And Protocols
For telehealth to function smoothly and reduce errors, proper hardware and software are critical, including telephone service, computers, broadband internet access, and electronic health records. The Federal Communications Commission (FCC) released funding to procure telehealth services and devices and some CHCs have received private funding; similar targeted funding mechanisms from states and the federal government are necessary at scale to equip hundreds of CHCs with the necessary telehealth capabilities.
However, merely having technology is not sufficient. Proper personnel with appropriate training are key to a high-functioning telehealth system along with support from information technology specialists. Additionally, CHCs need ancillary systems in place to allow for the effective use of phone and video visits. Empanelment systems to attribute patients to providers can allow for longitudinal follow-up even with telehealth. Daily huddles and team-based care can enhance the inherent complexities of coordinating care remotely. Protocols should be tailored for different specialties and services such as nutrition management and social work. Meanwhile, a robust e-consult referral network should allow primary care providers at CHCs to easily connect patients to specialty care when necessary. Adding robust protocols and systems will allow for the successful implementation and scaling of telehealth.
For example, groups of CHCs called the Health Center Controlled Networks (HCCNs), which have traditionally collaborated to leverage health information technology, are positioned to harness their economies of scale and group purchasing power to widely adopt new infrastructure while standardizing protocols. They could be a means to accelerate the adoption of telehealth technologies, trainings, and care models to optimize the use of telehealth across CHCs.
Telehealth Support For Vulnerable Patients
The patient population seen by CHCs presents unique challenges that not all ambulatory practices, particularly those in affluent neighborhoods, may face. Health centers care for many immigrant patients with limited English proficiency. Thus, clinics need financial support to contract with telehealth interpreter and translation services to provide equitable access and care. Better yet, all telehealth platforms contracting with CHCs should be required to provide multilingual support to deliver equitable access to telehealth services.
Moreover, many low-income patients lack health and digital literacy. Virtual telehealth platforms should design applications such that interfaces are intuitive and easy to navigate. They should provide specialized support to guide patients who are not familiar with telehealth systems. Additionally, insurers can reimburse CHCs that provide patient navigators, care coordinators, and shared decision-making support that bridge the health literacy divide.
Many around the US also do not have access to high-speed internet, consistent telephone services, and phones or computers with video conferencing capabilities. First, to allow for flexible access to telehealth for all patients, insurers should permanently waive geographic and originating site restrictions that limit the type and location of facilities from which patients can use telehealth. Second, insurers should waive audio-video requirements and consistently reimburse for phone-only visits to accommodate patients without video conferencing. Third, the type of services covered by telehealth should be expanded—ranging from primary care to physical therapy to nutrition counseling to behavioral health.
To address disparities in ownership of digital devices, taking a page out of the book of educators in low-income neighborhoods, local governments could loan laptops and smartphones or supply internet hotspots and phone-charging stations for these communities to enable access. Additionally, insurers could reimburse for the FCC Lifeline program to provide affordable communication services and cellular data to low-income populations to maintain their outpatient care.
Conclusions
As the COVID-19 pandemic sweeps through the US, health care delivery will never be the same. Health centers are struggling as many have been largely unprepared for the abrupt swing toward telehealth. COVID-19 may pose long-lasting damaging effects on CHCs and the patient populations that they serve. Nonspecific federal and state funding will allow CHCs to survive; however, deliberate action is needed to enhance telehealth capacities and ensure long-term resilience.
Similar to the Association of American Medical Colleges’ recent letter to CMS to make various telehealth changes permanent, both CMS and state governments should take immediate action by making permanent parity in reimbursement for telehealth services by all payers. State and federal policy should direct payers to lift onerous restrictions on the types of services covered via telehealth, audio/video requirements, and geographic and originating sites of telehealth services. States and payers should also explore innovative solutions to expand access to cellular data services and digital devices that allow low-income patients to digitally “get to their appointment,” similar to non-emergency medical transportation. Local governments should invest in digital infrastructure that expands broadband coverage and provides internet or cellular access points for people to engage in telehealth. Additionally, CHCs should come together under HCCNs to harness their group purchasing power to rapidly implement telehealth infrastructure that provides multilingual support and other tools that bridge gaps in digital literacy. Finally, best practices, trainings, and protocols should be standardized and disseminated across CHC networks to optimize the quality of telehealth.
By reorienting the goals for implementing telehealth, policy makers, payers, and providers can empower health centers to thrive into the future and meet the nation’s underserved patients where they are, even during the pandemic. In the long run, telehealth can increase access and equity—but only if the right investments are made now to fill the gaps laid bare by COVID-19.