Robert Wood Johnson University Hospital in New Brunswick, N.J., said it plans to temporarily cut off healthcare benefits for striking union workers, effective Sept. 1.
Hospital spokesperson Wendy Gottsegen described the move as unfortunate.
“We have said all along that no one benefits from a strike — least of all our nurses. We hope the union considers the impact a prolonged strike is having on our nurses and their families,” Ms. Gottsegen said in an Aug. 28 news release shared with Becker’s. “As of Sept. 1, RWJUH nurses must pay for their health benefits through COBRA. This hardship, in addition to the loss of wages throughout the strike, is very unfortunate and has been openly communicated to the union and the striking nurses since prior to the walkout on Aug. 4.”
The ongoing strike involves the United Steelworkers Local 4-200, which represents about 1,700 nurses at the facility.
Union members voted to authorize a strike in July. The union and hospital have been negotiating a new agreement for months, with the last bargaining session occurring Aug. 16.
During negotiations, the union has said it seeks a contract that provides safe staffing standards, living wages and quality, affordable healthcare.
Local 4-200 President Judy Danella, RN, said in a previous union release, “Our members remain deeply committed to our patients. However, we must address urgent concerns, like staffing. We need enough nurses on each shift, on each floor, so we can devote more time to each patient and keep ourselves safe on the job.”
Several nurses told TAPinto New Brunswick last week that they began preparing for the current situation ahead of the strike, taking overtime shifts and saving as much money as possible. Others told the publication they are taking part-time jobs or temporary employment elsewhere in the nursing field or adjacent roles.
“I think it’s important that you [remember] you might not get the job you want to do at that moment, but people have to do what they have to do to get it done,” Jessica Newcomb, RN, told TAPinto New Brunswick.
Meanwhile, the hospital has contracted with an agency to hire replacement nurses during the strike.
“As always, our top priority is to our patients. RWJUH is open, fully operational and completely staffed, and we remain steadfast in our commitment to deliver the highest quality and always-safe patient care,” Ms. Gottsegen said.
As of Aug. 28, no further dates for negotiations were scheduled by mediators.
Healthcare expenses declined in July, but not by enough to offset revenue losses, Kaufman Hall said in its latest National Hospital Flash Report.
Key Takeaways
Hospital performance declined on a month-over-month basis in July. All volume indicators registered declines this month. However, when compared to 2022, there is some slight improvement in operating margins.
Outpatient volumes decreased slightly more than inpatient. Some of this decline may be attributed to less patients seeking elective procedures in summer.
Expenses declined, but not enough to offset revenue losses. Labor continues to be the biggest share of hospital expenses, and expenses will likely continue to fluctuate due to inflation.
Bad debt and charity care rose month-over-month. Medicaid eligibility redetermination continues to affect hospitals and patients, with more than 30 states disenrolling people in June and July.
Action Steps
In an environment where hospitals continue to feel the effects of Medicaid disenrollment and labor expenses, those that have been more successful have made care transition a priority.
Hospitals should consider:
Starting off right by obtaining the necessary pre-certifications and payer authorizations before the patient comes in the door, as well as planning for discharge as soon as they are admitted.
Collecting data and using it to inform process improvement. Hospitals need to quantify lengths-of-stay and related data, and more importantly, use this data to make change.
Establishing relationships with post-acute care settings and having a clear pathway for patients’ post-discharge transition.
Albert Einstein determined that time is relative. And when it comes to healthcare, five years can be both a long and a short amount of time.
In August 2018, I launched the Fixing Healthcare podcast. At the time, the medium felt like the perfect auditory companion to the books and articles I’d been writing. By bringing on world-renowned guests and engaging in difficult but meaningful discussions, I hoped the show would have a positive impact on American medicine. After five years and 100 episodes, now is an opportune time to look back and examine how healthcare has improved and in what ways American medicine has become more problematic.
Here’s a look at the good, the bad and the ugly since episode one of Fixing Healthcare:
The Good
Drug breakthroughs and government actions headline medicine’s biggest wins over the past five years.
At first, health experts expressed doubts that Pfizer, Moderna and others could create a safe and effective Covid-19 vaccine with messenger RNA (mRNA) technology. After all, no one had succeeded in more than two decades of trying.
Thanks in part to Operation Warp Speed, the government-funded springboard for research, our nation produced multiple vaccines within less than a year. Previously, the quickest vaccine took four years to develop (mumps). All others required a minimum of five years.
The vaccines were pivotal in ending the coronavirus pandemic, and their success has opened the door to other life-saving drugs, including those that might prevent or fight cancer. And, of course, our world is now better prepared for when the next viral pandemic strikes.
Weight-Loss Drugs
Originally designed to help patients manage Type 2 diabetes, drugs like Ozempic have been helping people reverse obesity—a condition closely correlated with diabetes, heart disease and cancer.
For decades, America’s $150 billion a year diet industry has failed to curb the nation’s continued weight gain. So too have calls for increased exercise and proper nutrition, including restrictions on sugary sodas and fast foods.
In contrast, these GLP-1 medications are highly effective. They help overweight and obese people lose 15 to 25 pounds on average with side effects that are manageable for nearly all users.
The biggest stumbling block to their widespread use is the drug’s exorbitant price (upwards of $16,000 for a year’s supply).
Drug-Pricing Laws
With the Inflation Reduction Act of 2022, Congress took meaningful action to lower drug prices, a move the CBO estimates would reduce the federal deficit by $237 billion over 10 years.
It’s a good start. Americans today pay twice as much for the same medications as people in Europe largely because of Congressional legislation passed in 2003.
That law, the Medicare Prescription Drug Price Negotiation Act, made it illegal for Health and Human Services (HHS) to negotiate drug prices with manufacturers—even for the individuals publicly insured through Medicare and Medicaid.
Now, under provisions of the new Inflation Reduction Act, the government will be able to negotiate the prices of 10 widely prescribed medications based on how much Medicare’s Part D program spends. The lineup is expected to include prescription treatments for arthritis, cancer, asthma and cardiovascular disease. Unfortunately, the program won’t take effect until 2026. And as of now, several legal challenges from both drug manufacturers and the U.S. Chamber of Commerce are pending.
The Bad
Spiking costs, ongoing racial inequalities and millions of Americans without health insurance make up three disappointing healthcare failures of the past five years.
Cost And Quality
The U.S. spends nearly twice as much on healthcare per citizen as other countries, yet our nation lags 10 of the wealthiest countries in medical performance and clinical outcomes. As a result, Americans die younger and experience more complications from chronic diseases than people in peer nations.
As prices climb ever-higher, at least half of Americans can’t afford to pay their out-of-pocket medical bills, which remain the leading cause of U.S. bankruptcy. And with rising insurance premiums alongside growing out-of-pocket expenses, more people are delaying their medical care and rationing their medications, including life-essential drugs like insulin. This creates a vicious cycle that will likely prolong today’s healthcare problems well into the future.
Health Disparities
Inequalities in American medicine persist along racial lines—despite action-oriented words from health officials that date back decades.
Today, patients in minority populations receive unequal and inequitable medical treatment when compared to white patients. That’s true even when adjusting for differences in geography, insurance status and socioeconomics.
Racism in medical care has been well-documented throughout history. But the early days of the Covid-19 pandemic provided several recent and deadly examples. From testing to treatment, Black and Latino patients received both poorer quality and less medical care, doubling and even tripling their chances of dying from the disease.
The problems can be observed across the medical spectrum. Studies show Black women are still less likely to be offered breast reconstruction after mastectomy than white women. Research also finds that Black patients are 40% less likely to receive pain medication after surgery. Although technology could have helped to mitigate health disparities, our nation’s unwillingness to acknowledge the severity of the problem has made the problem worse.
Uninsurance
Although there are now more than 90 million Americans enrolled in Medicaid, there are still 30 million people without any health insurance. This disturbing reality comes a full decade after the passage of the Affordable Care Act.
On Capitol Hill, there is no plan in place to reduce the number of uninsured.
Moreover, many states are looking to significantly rollback their Medicaid enrollment in the post-Covid era. Kaiser Family Foundation estimates that between 8 million and 24 million people will lose Medicaid coverage during the unwinding of the continuous enrollment provisions implemented during the pandemic. Without coverage, people have a harder time obtaining the preventive services they need and, as a result, they suffer more chronic diseases and die younger.
The Ugly
An overall decrease in longevity, along with higher maternal mortality and a worsening mental-health crisis, comprise the greatest failures of U.S. healthcare over the past five years.
Life Expectancy
Despite radical advances in medical science over the past five years, American life expectancy is back to where it was at the turn of the 20th century, according to CDC data.
Alongside environmental and social factors are a number of medical causes for the nation’s dip in longevity. Research demonstrated that many of the 1 million-plus Covid-19 deaths were preventable. So, too, was the nation’s rise in opioid deaths and teen suicides.
Regardless of exact causation, Americans are living two years less on average than when we started the Fixing Healthcare podcast five years ago.
Maternal Mortality
Compared to peer nations, the United States is the only country with a growing rate of mothers dying from childbirth. The U.S. experiences 17.4 maternal deaths per 100,000 live births. In contrast, Norway is at 1.8 and the Netherlands at 3.0.
The risk of dying during delivery or in the post-partum period is dramatically higher for Black women in the United States. Even when controlling for economic factors, Black mothers still suffer twice as many deaths from childbirth as white women.
And with growing restrictions on a woman’s right to choose, the maternal mortality rate will likely continue to rise in the United States going forward.
Mental Health
Finally, the mental health of our country is in decline with rates of anxiety, depression and suicide on the rise.
These problems were bad prior to Covid-19, but years of isolation and social distancing only aggravated the problem. Suicide is now a leading cause of death for teenagers. Now, more than 1 in every 1,000 youths take their own lives each year. The newest data show that suicides across the U.S. have reached an all-time high and now exceed homicides.
Even with the expanded use of telemedicine, mental health in our nation is likely to become worse as Americans struggle to access and afford the services they require.
The Future
In looking at the three lists, I’m reminded of a baseball slugger who can occasionally hit awe-inspiring home runs but strikes out most of the time. The crowd may love the big hitter and celebrate the long ball, but in both baseball and healthcare, failing at the basics consistently results in more losses than wins.
Over the past five years, American medicine has produced a losing record. New drugs and surgical breakthroughs have made headlines, but the deeper, more systemic failures of American healthcare have rarely penetrated the news cycle.
If our nation wants to make the next five years better and healthier than the last five, elected officials and healthcare leaders will need to make major improvements. The steps required to do so will be the focus of my next article.
Last Monday, four U.S. Senators took aim at the tax exemption enjoyed by not-for-profit (NFP) hospitals in a letter to the IRS demanding detailed accounting for community benefits and increased agency oversight of NFP hospitals that fall short.
Last Tuesday, the Elevance Health Policy Institute released a study concluding that the consolidation of hospitals into multi-hospital systems (for-profit/not-for-profit) results in higher prices without commensurate improvement in patient care quality. “
Friday, Kaiser Health News Editor in Chief Elizabeth Rosenthal took aim at Ballad Health which operates in TN and VA “…which has generously contributed to performing arts and athletic centers as well as school bands. But…skimped on health care — closing intensive care units and reducing the number of nurses per ward — and demanded higher prices from insurers and patients.”
And also last week, the Pharmaceuticals’ Manufacturers Association released its annual study of hospital mark-ups for the top 20 prescription drugs used on hospitals asserting a direct connection between hospital mark-ups (which ranged from 234% to 724%) and increasing medical debt hitting households.
(Excerpts from these are included in the “Quotables” section that follows).
It was not a good week for hospitals, especially not-for-profit hospitals.
In reality, the storm cloud that has gathered over not-for-profit health hospitals in recent months has been buoyed in large measure by well-funded critiques by Arnold Ventures,Lown Institute, West Health, Patient Rights Advocate and others. Providence, Ascension, Bon Secours and now Ballad have been criticized for inadequate community benefits, excessive CEO compensation, aggressive patient debt collection policies and price gauging attributed to hospital consolidation.
This cloud has drawn attention from lawmakers: in NC, the State Treasurer Dale Folwell has called out the state’s 8 major NFP systems for inadequate community benefit and excess CEO compensation.
In Indiana, State Senator Travis Holdman is accusing the state’s NFP hospitals of “hoarding cash” and threatening that “if not-for-profit hospitals aren’t willing to use their tax-exempt status for the benefit of our communities, public policy on this matter can always be changed.” And now an influential quartet of U.S. Senators is pledging action to complement with anti-hospital consolidation efforts in the FTC leveraging its a team of 40 hospital deal investigators.
In response last week, the American Hospital Association called out health insurer consolidation as a major contributor to high prices and,
in a US News and World Report Op Ed August 8, challenged that “Health insurance should be a bridge to medical care, not a barrier.
Yet too many commercial health insurance policies often delay, disrupt and deny medically necessary care to patients,” noting that consumer medical debt is directly linked to insurer’ benefits that increase consumer exposure to out of pocket costs.
My take:
It’s clear that not-for-profit hospitals pose a unique target for detractors: they operate more than half of all U.S. hospitals and directly employ more than a third of U.S. physicians.
But ownership status (private not-for-profit, for-profit investor owned or government-owned) per se seems to matter less than the availability of facilities and services when they’re needed.
And the public’s opinion about the business of running hospitals is relatively uninformed beyond their anecdotal use experiences that shape their perceptions. Thus, claims by not-for-profit hospital officials that their finances are teetering on insolvency fall on deaf ears, especially in communities where cranes hover above their patient towers and their brands are ubiquitous.
Demand for hospital services is increasing and shifting, wage and supply costs (including prescription drugs) are soaring, and resources are limited for most.
The size, scale and CEO compensation for the biggest not-for-profit health systems pale in comparison to their counterparts in health insurance and prescription drug manufacturing or even the biggest investor-owned health system, HCA…but that’s not the point.
NFPs are being challenged to demonstrate they merit the tax-exempt treatment they enjoy unlike their investor-owned and public hospital competitors and that’s been a moving target.
Thus, the methodology for consistently defining and accounting for community benefits needs attention. That would be a good start but alone it will not solve the more fundamental issue: what’s the future for the U.S. health system, what role do players including hospitals and others need to play, and how should it be structured and funded?
The issues facing the U.S. health industry are complex. The role hospitals will play is also uncertain. If, as polls indicate, the majority of Americans prefer a private health system that features competition, transparency, affordability and equitable access, the remedy will require input from every major healthcare sector including employers, public health, private capital and regulators alongside others.
It will require less from DC policy wonks and sanctimonious talking heads and more from frontline efforts and privately-backed innovators in communities, companies and in not-for-profit health systems that take community benefit seriously.
No sector owns the franchise for certainty about the future of U.S. healthcare nor its moral high ground. That includes not-for-profit hospitals.
The darkening cloud that hovers over not-for-profit health systems needs attention, but not alone, despite efforts to suggest otherwise.
Clarifying the community-benefit standard is a start, but not enough.
Are NFP hospitals a problem? Some are, most aren’t but all are impacted by the darkening cloud.
Last week, six notable associations representing health insurers and large employers announced Better Solutions for Healthcare (BSH):“An advocacy organization dedicated to bringing together employers, consumers, and taxpayers to educate lawmakers on the rising cost of healthcare and provide ideas on how we can work together to find better solutions that lower healthcare costs for ALL Americans.”
BSH, which represents 492 large employers, 34 Blue Cross plans, 139 insurers and 42 business coalitions, blames hospitals asserting that “over the last ten years alone, the cost of providing employee coverage has increased 47% with hospitals serving as the number one driver of healthcare costs.”
Its members, AHIP, the Blue Cross Blue Shield Association, the Business Group on Health, Public Sector Health Care Roundtable, National Alliance of Healthcare Purchaser Coalitions and the American Benefits Council, pledge to…
Promote hospital competition
Enforce Federal Price Transparency Laws for Hospital Charges
Rein in Hospital Price Mark-ups
Insure Honest Billing Practices
And, of particular significance, BSH calls out “the growing practice of corporate hospitals establishing local monopolies and leveraging their market dominance to charge patients more…With hospital consolidation driving down competition, there’s no pressure for hospitals to bring costs back within reach for employees, retirees and their families…prices at monopoly hospitals are 12% higher than in markets with four or more competitors.”
The BSH leadership team is led by DC-based healthcare policy veterans with notable lobbying chops: Adam “Buck” Buckalew, a former Sen. Lamar Alexander (R-TN) staffer who worked on the Health Education, Labor and Pensions (HELP) committee and is credited with successfully spearheading the No Surprises Act legislation that took effect in January 2022, and Kathryn Spangler, another former HELP staffer under former Sen. Mike Enzi (R-WY) who most recently served as Senior Policy Advisor at the American Benefits Council.
It’s a line in the sand for hospitals, especially large not-for-profit systems that are on the defensive due to mounting criticism.
Examples from last week: Atrium and Caremont were singled in NC by the state Treasurer for their debt collection practices based on a Duke study that got wide media coverage. Allina’s dispute with 550 of its primary care providers seeking union representation based on their concerns about patient safety. Jefferson Health was called out for missteps under its prior administration’s “growth at all costs” agenda and the $35 million 2021 compensation for Common Spirit’s CEO received notice in industry coverage.
My take:
BSH represents an important alignment of health insurers with large employers who have shouldered a disproportionate share of health costs for years through the prices imposed for the hospitals, prescriptions and services their employees and dependents use.
Though it’s too early to predict how BSH vs. Corporate Hospitals will play out, especially in a divided Congress and with 2024 elections in 14 months, it’s important to inject a fair and balanced context for this contest as the article of war are unsealed:
Health insurers and hospitals share the blame for high health costs along with prescription drug manufacturers and others. The U.S. system feasts on opaque pricing, regulated monopolies and supply-induced demand. Studies show unit costs for hospitals along with prescription drug costs bear primary responsibility for two-thirds of health cost increases in recent years—the result of increased demand and medical inflation. But insurers are complicit: benefits design strategies that pre-empt preventive health and add administrative costs are parts of the problem.
Corporatization of the U.S. system cuts across every sector: Healthcare’s version of Moneyball is decidedly tilted toward bigger is better: in healthcare, that’s no exception. 3 of the top 10 in the Fortune 100 are healthcare (CVS-Aetna, United, McKesson)) and HCA (#66) is the only provider on the list. The U.S. healthcare industry is the largest private employer in the U.S. economy: how BSH addresses healthcare’s biggest employers which include its hospitals will be worth watching. And Big Pharma companies pose an immediate challenge: just last week, HHS called out the U.S. Chamber of Commerce for siding with Big Pharma against implementation of drug price controls in the Inflation Reduction Act—popular with voters but not so much in Big Pharma Board rooms.
The focus will be on Federal health policies. BSH represents insurers and employers that operate across state lines–so do the majority of major health systems. Thus, federal rules, regulations, administrative actions, executive orders, and court decisions will be center-stage in the BSH v. corporate hospitals war. Revised national policies around Medicare and federal programs including military and Veterans’ health, pricing, equitable access, affordability, consolidation, monopolies, data ownership, ERISA and tax exemptions, patent protections and more might emerge from the conflict. As consolidation gets attention, the differing definitions of “markets” will require attention: technology has enabled insurers and providers to operate outside traditional geographic constraints, so what’s next? And, complicating matters, federalization of healthcare will immediately impact states as referenda tackle price controls, drug pricing, Medicaid coverage and abortion rights—hot buttons for voters and state officials.
Boards of directors in each healthcare organization will be exposed to greater scrutiny for their actions: CEO compensation, growth strategies, M&A deals, member/enrollee/patient experience oversight, culture and more are under the direct oversight of Boards but most deflect accountability for major decisions that pose harm. Balancing shareholder interests against the greater good is no small feat, especially in a private health system which depends on private capital for its innovations.
8.6% of the U.S. population is uninsured, 41% of Americans have outstanding medical debt, and the majority believe health costs are excessive and the U.S. system is heading in the wrong direction.
Compared to other modern systems in the world, ours is the most expensive for its health services, least invested in social determinants that directly impact 70% of its costs and worst for the % of our population that recently skipped needed medical care (39.0% (vs. next closest Australia 21.2%), skipped dental care (36.2% vs. next closest Australia 31.7%) and had serious problems/ were unable to pay medical bills (22.4% next closest France 10.1%). Thus, it’s a system in which costs, prices and affordability appear afterthoughts.
Who will win BSH vs. Corporate Hospitals? It might appear a winner-take all showdown between lobbyists for BSH and hospital hired guns but that’s shortsighted. Both will pull out the stops to win favor with elected officials but both face growing pushback in Congress and state legislatures where “corporatization” seems more about a blame game than long-term solution.
Each side will use heavy artillery to advance their positions discredit the other. And unless the special interests that bolster efforts by payers are hospitals are subordinated to the needs of the population and greater good, it’s not the war to end all healthcare wars. That war is on the horizon.
On Tuesday, Verona, WI-based Epic and Redmond, WA-based Microsoft announced a suite of new AI-powered solutions available to users of Epic’s electronic health records (EHR) system.
In April 2023, Epic began integrating Microsoft’s Azure OpenAI Service, which utilizes GPT-4 capabilities, into its EHR. This next phase builds on that collaboration, introducing tools that support ambient notetaking, create clinical documentation summaries, and offer medical coding suggestions, all through generative AI. Epic is rolling out these services as it debuts its revamped third-party app market, which now hosts programs developed by Microsoft-owned Nuance as well as smaller startups.
The Gist: Given the massive datasets required to train these AI programs, the competition to deploy AI-powered healthcare workforce at scale will likely be driven by the largest tech and healthcare data companies rather than smaller start-ups.
Epic’s new app marketplace for third-party vendors is meant to ensure just that, by positioning it as the primary hub for many healthcare-specific AI programs in development.
Health systems will race to take advantage of the cost savings unlocked by these technologies, which they will hope integrate seamlessly into their EHRs.
As physicians stand to benefit from eased administrative burdens, but also have justified concerns over generative AI’s reliability, health systems should keep an open dialogue with frontline providers as they implement these new tools.
At a meeting last week, a surgeon (and loyal Weekly Gist reader) shared his thoughts on our recent coverage of research evaluating physician earnings, and analysis comparing the incomes of American doctors with those in other Western countries.
(The gist: unsurprisingly, American doctors make more money—and one of the primary reasons is that there are simply fewer physicians per capita here than in most other Western nations.)
His retort: “It sounds like you’re rooting for doctors to get paid less!” Given the number of emails we received on the piece, it’s clear that the topic touched a nerve.
A few doctors pointed out the limitations of simple supply and demand in driving physician salaries. Of course there are important structural differences between our delivery and payment system and those in other nations: fee-for-service versus global payment; length of training and degree of student debt; and relative salaries of specialists versus primary care physicians, just to name a few.
But if anything, the effects of supply and demand are amplified in a more market-driven system like the US. Plus, there are factors, like regulation of the number of residency training slots, that keep supply artificially low—and physician incomes in competitive specialties high.
At a high level, the data do show that prices—both physician and hospital—are higher in the US than other countries, whereas utilization is roughly similar.
Over time, we’d expect that there will be continued price pressure driving down doctors’ incomes, but large swings in physician salaries will take a generation or more to emerge.
And should physicians experience more salary pressure, expect more of them to seek additional sources of entrepreneurial and investment income—further increasing the spread between the lowest- and highest-paid doctors.
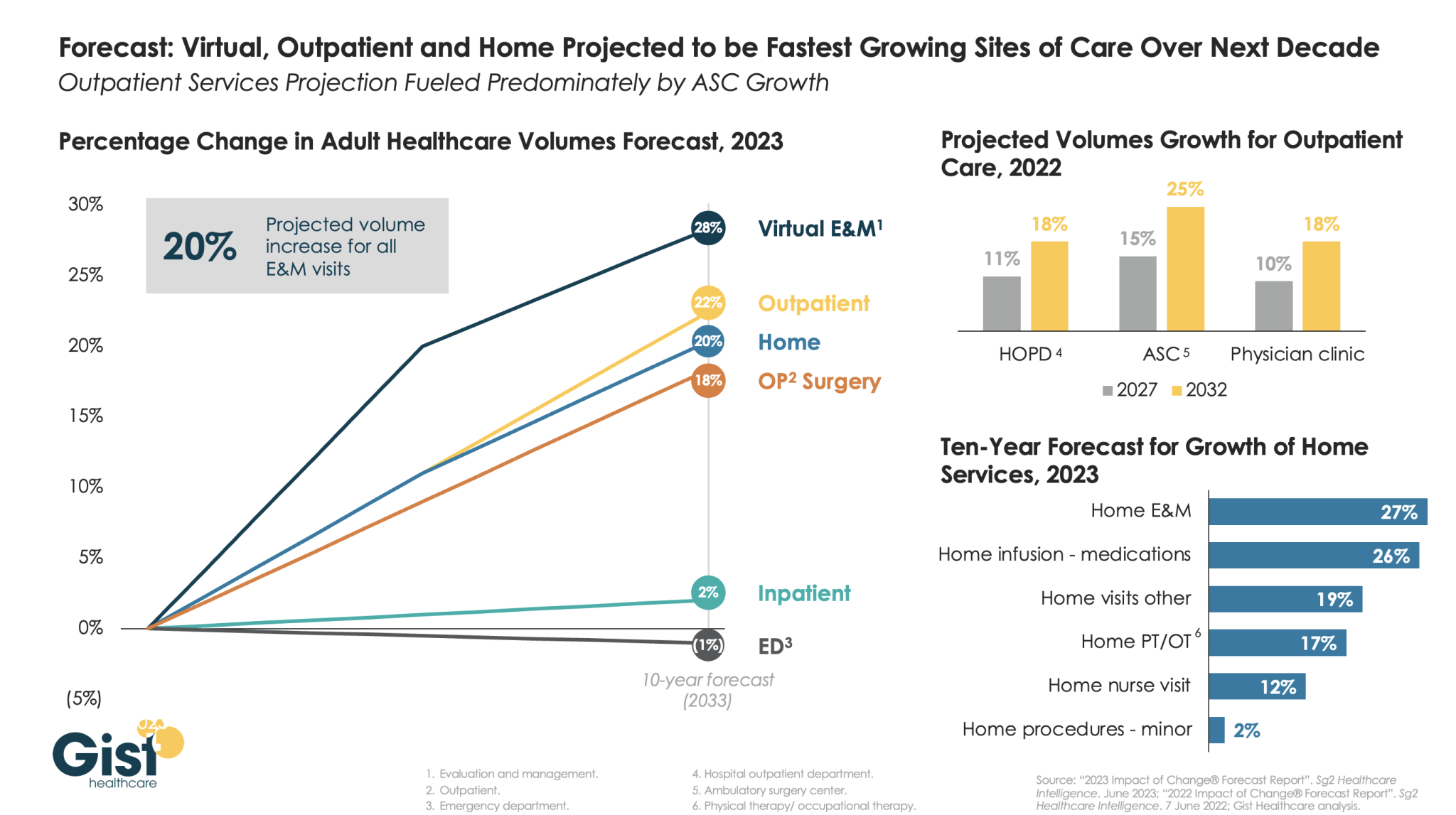
The pandemic accelerated the outpatient shift, which had been progressing steadily for decades, into a new gear, as safety-minded consumers avoided inpatient settings.
Using the latest forecasting data from strategic healthcare consulting firm Sg2, the graphic above illustrates how the outpatient shift will continue to accelerate in the coming years. With each projected to grow by 20 percent or more, outpatient, virtual, and home-based care services will continue far outpace growth in hospital-based care over the next decade.
Ambulatory surgery centers (ASCs) will be at the center of this care shift, reflected by a projected 25 percent rise in ASC volumes by 2032.
The breadth of care available at home will also expand as care delivery technology improves. With the population becoming older and sicker, higher incidence of chronic disease will be met by a rapid expansion of home evaluation and management services (E&M),reflecting a shift away from hospitals and doctors’ offices as hubs for complex care management.
Instead, the patients still coming to hospitals will present with increasingly acute conditions, driving up demand for resource-intensive critical care, as broader inpatient volume remains relatively flat.
An investigative piece published this month by ProPublica documents how it came to be that nearly 60 percent of healthcare providers report being charged fees to receive electronic payments from insurers.
The fees, which can be as high as five percent of total reimbursement, were briefly forbidden by the Centers for Medicare and Medicaid Services (CMS), before the agency reversed its policy in 2018. The article follows one dogged physician’s efforts to uncover why CMS allows these fees. His voluminous stream of public records requests revealed a highly coordinated pressure campaign, mounted by the insurance industry through one particularly influential regulator-turned-lobbyist.
While the American Medical Association has urged the Biden administration to protect physicians from these fees, and the Veterans Health Administration is refusing to pay them, CMS is so far maintaining the position that electronic-payment claims-processing fees are permissible.
The Gist: Through partnerships with payment companies, who charge double the average fees of electronic bank transfers and share the spoils of their “virtual credit cards”, insurers are essentially using the same business model as credit card companies, skimming revenue from physician payments just as Visa and MasterCard do to merchants.
With the increasing consolidation of both insurers and claims processors, physicians are left with little recourse but to pay these fees, as nonelectronic payments come with infrastructure costs and payment delays.
While the shift to electronic payments spurred on by the Affordable Care Act was supposed to improve efficiency, this article offers yet another example of how efficiency gains can be captured by industry middlemen before they can be translated into provider and consumer benefits.