
Cartoon – Thanks for Giving
Jobless claims plunge to 199K, lowest level since 1969
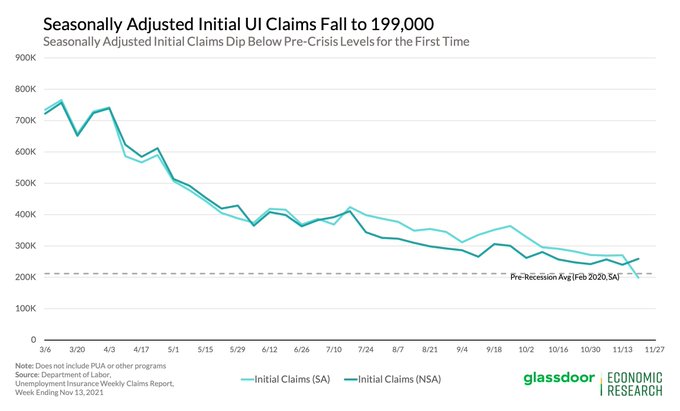
For the 1st time during the pandemic, initial UI claims have dipped below pre-crisis levels, falling to 199,000 (vs the Feb 2020 avg: 211,700). Layoffs are hitting new lows amid ongoing labor shortages as employers look to hold onto hard-to-find workers.
New weekly claims for jobless aid plunged to the lowest level in more than 50 years last week, according to data released Wednesday by the Labor Department.
In the week ending Nov. 20, there were 199,000 initial applications for unemployment insurance, according to the seasonally adjusted figures, a decline of 71,000 from the previous week. Claims fell to the lowest level since November 1969 and are now well below the pre-pandemic trough of 225,000 applications received the week of March 14, 2020.
The steep drop in unemployment applications comes after several strong months of job growth and rising consumer spending heading into the holiday shopping season. While high inflation has stressed many household budgets, U.S. job growth, economic production, stock values and corporate profits have all steamed ahead.
“Getting new claims below the 200,000 level for the first time since the pandemic began is truly significant, portraying further improvement,” said Mark Hamrick, chief economic analyst at Bankrate.com.
“The strains associated with higher prices, shortages of supplies and available job candidates are weighed against low levels of layoffs, wage gains and a falling unemployment rate,” he continued. “Growth will likely be above par for the foreseeable future, but within the context of historically high inflation which should relax its grip on the economy to some degree in the year ahead.”
The U.S. added 531,000 jobs in October and job growth in the previous months was revised substantially higher after a string of what first appeared to be meager gains. While businesses have struggled to hire enough workers to meet surging consumer demand, the decline in jobless claims appears to be a sign of an improving labor market.
“Layoffs are hitting new lows amid ongoing labor shortages as employers look to hold onto hard-to-find workers,” said Daniel Zhao, senior economist at Glassdoor, in a Wednesday thread on Twitter.
Even so, Zhao said the sharp decline below pre-pandemic levels may have been due to a lower than expected seasonal impact on hiring.
“As you can see from the above chart, this is in part due to the seasonal adjustment expecting a much larger jump in non-seasonally adjusted claims, so this dip below pre-crisis levels may be short-lived,” he explained.


“Please pass the green beans.” “What kind of pie is that?”“What about spike proteins!?”These are some of the phrases that may be uttered during your Thanksgiving and holiday dinners this season. But! We have prepared a glossary for you. Swipe through a quick guide to some of the most misused terms around vaccines that PolitiFact has noticed in our fact-checking. And because we know that shouts of “that’s wrong!” don’t go over smooth like gravy, we’re including an expert’s advice on how to talk about vaccine falsehoods with family and friends.The big thing to know: It’s better to respond with facts than to offer corrections.”If they said something like ‘the vaccine is dangerous,’ include a statistic about how 75% of the people in their state have gotten vaccinated and none have died, or how severe and dangerous COVID-19 is,” said Rupali Limaye, an associate scientist at Johns Hopkins School of Public Health. “And, ultimately, make sure you’re saying it all with empathy.”







After months of negotiations, House Democrats on Friday passed their version of the Build Back Better bill—an expansive $1.7 trillion package that contains some of the largest health reforms since the Affordable Care Act’s passage in 2010.
While the overall scope of the bill is roughly half the size of President Biden’s original $3 trillion proposal, many of Democrats’ key health care provisions made it in, albeit with some modifications. What’s more, the Congressional Budget Office projected that while the overall bill would add $367 billion to the deficit over the 10 year period, the health care provisions would all be largely paid for by provisions aimed at lowering drug prices.
Below, I round up the five biggest health care changes included in the House bill.
Find out where the states stand on Medicaid expansion
The House bill leverages the ACA’s exchanges and federal tax credits to expand access to coverage in two ways. First, the bill would extend the American Rescue Plan’s enhanced ACA tax credits through 2025. The enhanced tax credits, which are currently slated to expire in 2023, fully subsidize coverage for people with annual incomes up to 150% of the federal poverty level (FPL) and have enabled people above 400% FPL to qualify for subsidies and capped their premium costs at 8.5% of their incomes.
While Democrats had originally proposed to permanently expand those subsidies, they ultimately had to scale back this—and other proposals—to ensure they could cover the costs. But as we’ve seen in the past, it is much harder to take away an existing benefit or subsidy than it is to create a new one—so while the current bill was able to cover the cost of the health care provisions by making them temporary, lawmakers will have to revisit the tax credits before 2025 and find new money to either further extend them or permanently authorize them. This is one of several health care provisions we could see the Senate take a closer week at in the coming weeks.
Second, the House bill takes aim at the so-called Medicaid coverage gap. The bill would enable residents below 138% FPL who live in states that have not expanded their Medicaid programs to qualify for fully subsidized exchange plans through 2025. While an earlier version of the House bill included language for a new federal Medicaid program covering those below 138% FPL who live in non-expansion states to begin in 2025, the final House bill contains no such program.
Instead, the bill aims to encourage non-expansion states to expand their Medicaid programs by reducing their Disproportionate Share Hospital (DSH) payments by 12.5% beginning in 2023—a significant cut that the American Hospital Association (AHA) estimates would reduce DSH payments in those states by $2.2 billion over five years and $4.7 billion over 10 years. At the same time, expansion states would see their federal match for spending on the Medicaid expansion population rise from 90% to 93% from 2023 through 2025.
While the AHA and others are pushing back against the proposed DSH payment cuts—the move addresses the moral hazard component that critics raised about earlier versions. It no longer rewards holdout states for not expanding their programs—effectively punishing those who did and are now on the hook for 10% of their expansion population’s costs. It’s a clever move, and one we’ll be watching to see if it survives the Senate.
The House bill adds a hearing benefit to Medicare beginning in 2023. The hearing benefits would cover hearing aids and aural rehabilitation, among other services. While this is certainly a win for many Medicare beneficiaries who do not have or cannot afford private Medicare Advantage plans, this is significantly scaled back from the original proposal to add hearing, as well as dental and vision benefits.
However, given that Sen. Bernie Sanders (I-Vt.) has named Medicare benefit expansions as one of his top priorities, it’s possible we could see this topic revisited in the Senate. But any meaningful change would mean Democrats need to find more money to cover the costs—and so far, that has proved challenging.
The House bill allocates $150 billion for home- and community-based care. The funding would be used to help increase home care provider reimbursement rates and help states bolster home- and community-based care infrastructure.
While the funding is down from an original proposal of $400 billion, the Biden administration—and the Covid-19 pandemic—have made it clear that home-based health care will continue to grow and be a key player in the U.S. health care delivery system. Providers looking at their offerings should keep an eye on how states are investing these funds and building out home-based health care delivery in their areas.
Democrats scored a huge win in the House bill, and that is securing Medicare authority—albeit narrower authority than they sought—to negotiate prices for some of the highest-priced Part B or Part D drugs. Under the bill, HHS would be able to select 10 drugs to negotiation in 2025, up to 15 drugs in 2026 and 2027, and then up to 20 drugs per year in 2028. To be eligible for negotiation, a drug could no longer be subject to market exclusivity.
Drug manufacturers that do not negotiate eligible drug prices could be subject to an excise tax. This was perhaps one of the most contentious provisions debated in the health care portions of this bill. Democrats for years have been seeking to give Medicare drug pricing authority, but intense lobbying and Republican—and some Democrat—objections have kept this proposal on the shelf. While it’s not the first time the House has passed a bill with drug price negotiation—it is the first time we are in a place where the Senate could reasonably pass either this or a modified version of the proposal.
The bill also would redesign the Medicare Part D benefit to create an annual cap of $2,000 on seniors’ out-of-pocket drug costs, and impose an inflation rebate on drug manufacturers’ whose drug prices rise faster than inflation (based on 2021) in a given year.
The House bill also includes provisions to permanently fund CHIP, bolster the country’s pandemic preparedness and response, and bolster the health care workforce through new training and workforce programs, the nation’s first permanent federal paid family and medical leave program, investments in childcare, and more.
While the health care provisions in the House bill are notable, it’s important to remember that this is not the end of the road. The House bill now goes to the Senate, where the Senate parliamentarian will check provisions against the Byrd rule—a Senate rule requiring reconciliation bills to meet certain budgetary requirements.
Democrats also will enter a new round of negotiations, and industry groups—including PhRMA and AHA—are expected to launch a new round of lobbying. PhRMA objects to the bill’s drug price negotiation provision and AHA is fighting the provision to reduce DSH payments in non-Medicaid expansion states by 12.5%. Any Senate-passed reconciliation bill will need to go back to the House for final approval before it can go to Biden’s desk.
But this is not the only thing on lawmakers’ plates in December. Members of Congress also face several other deadlines, including addressing looming physician payment cuts and passing end of the year spending bills. The short-version is, while there’s a lot to learn from the House-passed bill, it’s possible the Senate version could look very different—and it may take several weeks before we see that bill take shape.

Amid a nationwide staffing shortage, rising demand for nurses has led hospitals to increase salaries and other benefits to attract and retain workers, Melanie Evans reports for the Wall Street Journal.
Hospitals across the country have been struggling amid staffing shortages, particularly of nurses, Evans reports. According to health care consultancy Premier, nurse turnover rates have increased to around 22% this year, up from the annual rate of about 18% in 2019.
“We are employing more nurses now than we ever have, and we also have more vacancies than we ever had,” said Greg Till, chief people officer at Providence Health & Services.
To retain their current nurses and attract new staff, many hospitals have increased their nurses’ salaries to remain competitive in the job market, Evans reports.
For example, HCA Healthcare, one of the largest hospital chains in the country, said it increased nurse pay this year to keep up with Covid-19 surges and compete with rivals also trying to fill vacant positions.
Similarly, Jefferson Health in May raised salaries for its nearly 10,000 nurses by 10% after the system discovered that rivals had increased their compensation. “The circumstances required it,” said Kate Fitzpatrick, Jefferson’s chief nurse executive.
In addition, Citizens Memorial Hospital in Bolivar, Mo., this month raised its nurses’ salaries by up to 5% after rivals in other nearby cities increased their workers’ wages. Sarah Hanak, Citizen Memorial’s CNO, said the hospital also increased the hourly wages of nurses working overnight shifts by around 15% to ensure sufficient staffing for those shifts.
“We were forced to,” Hanak said. “We absolutely have to stay competitive.”
Overall, the average annual salary for RNs, not including bonus pay, grew to $81,376, according to Premier—a 4% increase across the first nine months of the year. This is larger than the 3.3% increase in the average annual nurse salary for 2020 and the 2.6% increase in 2019, Evans writes.
In addition to salary increases, some organizations, such as Providence, are also offering other benefits to attract and retain nurses, such as more time off, greater schedule flexibility, and new career development opportunities. Many hospitals are also hiring new graduates to work in specialized roles in ORs and other areas, allowing them to advance their careers more quickly than they would have before.
Overall, this rising demand for nurses has allowed those entering the workforce to negotiate higher salaries, more flexible working hours, and other benefits, Evans writes.
“I think you get to write your ticket,” said Tessa Johnson, president of the North Dakota Nurses Association.
Nurse compensation increases were inevitable—here’s why
It was inevitable that we would get to this point: baseline nurse compensation on a clear upward trajectory. Inevitable because this boils down to laws of supply and demand. Amid a clear nursing shortage, organizations are being forced to raise baseline compensation to compete for increasingly scarce qualified nurses. This is true in nearly every market, even for those considered to be ‘destination employers.’
If anything, what’s most surprising in the data from Premier is the moderated increase of around 4%. From a worker’s perspective, that’s not even covering cost of living increases due to inflation. However, amid this new data, it’s important to keep two things in mind:

The American Hospital Association, the American Medical Association and the American Nurses Association teamed up to release a new “Forever Grateful” TV and digital ad campaign on Monday to thank health care workers.
Why it matters: The campaign comes in the face of record levels of reported health care worker burnout tied, in part, to the prolonged emergency response to COVID-19.
https://www.axios.com/axios-ipsos-poll-thanksgiving-covid-7a043049-d25c-4d3a-9bab-2853973f67af.html

Two-in-three Americans will celebrate this Thanksgiving with friends or family outside their immediate households, and about half of those say their gatherings could include unvaccinated people, according to the latest installment of the Axios/Ipsos Coronavirus Index.
Why it matters: Vaccinations and booster shots are giving more people confidence to resume traditions like sitting around a packed table with masks off. But many are doing so with heightened awareness of what they don’t know when it comes to their holiday companions.
What they’re saying: “We’re just in a holding pattern,” said Cliff Young, president of Ipsos U.S. Public Affairs.
By the numbers: 67% of U.S. adults surveyed said they’ll see friends or family outside their households. That’s 73% of Republicans, 70% of independents and 63% of Democrats.
Between the lines: There’s a modest partisan gap around openness to returning to the communal Thanksgiving table — but a gulf around who you’re willing to sit with.
The big picture: This week’s findings show overwhelming support (86%) for every vaccinated American who wants a booster being able to get one. But only about one in four respondents said they knew much about an anti-viral COVID-19 pill awaiting FDA approval.
https://www.axios.com/covid-vaccine-boosters-thanksgiving-5851be4a-79a7-423a-93bb-390d1eb7d4d3.html

Federal officials waited months before making all American adults eligible for a COVID-19 booster shot — meaning millions of Americans may not have the strongest possible protection as they head into holiday travel.
Why it matters: Critics say the confusing process undermined what has now become a critical effort to stave off another wave of the pandemic.
What they’re saying: “We have a consensus. Boosters are very important in maintaining people’s defenses against COVID. We need to get as many people vaccinated and boosted [as possible] as the winter sets in,” David Kessler, the chief science officer of Biden’s COVID response, said in an interview.
Context: Preliminary data released months ago suggested a significant decline in the vaccines’ effectiveness at preventing infection, although they held up well against severe disease.
In the meantime, red and blue states alike decided to ignore the CDC and open up booster eligibility on their own, and breakthrough infections have become increasingly common.
“Some of us were there several months ago. Some wanted more data. In the end, there’s a convergence of opinions. It’s the way an open scientific public health process should work,” Kessler said.
Between the lines: The U.S. drug approval process — with its insistence on high-quality data and careful expert reviews — is the world’s gold standard precisely because it moves deliberately. Regulators have been trying this whole time to figure out how to adapt that system to a fast-moving pandemic.
Some federal officials, as well as many outside experts, said there wasn’t enough data to make a broad booster recommendation earlier this fall.
What they’re saying: “Some argued early on that the primary series was good enough and we should conserve doses for the world. What’s emerging is that all people in the world are going to need to be boosted,” a senior administration official said.

