The undercurrent of the VP debate is the age and health of the two men vying for the presidency.
The two remaining presidential debates, scheduled for October 15 and 22, are in question due to President Trump’s positive COVID-19 and quarantine status, making the vice presidential debate this Wednesday at 9 p.m. even more important than VP debates of past elections.
The undercurrent in the debate consists of the ages of challenger Biden, who is 77 and turning 78 before the end of the year, and Trump, 74, who has been hospitalized for COVID-19 and was released from Walter Reed Army Medical Center on Monday afternoon. Trump has said he plans to debate Biden on October 15.
This VP debate is big, said Paul Keckley, a healthcare policy analyst and managing editor of the Keckley Report.
“The reason is not so much the two are debating,” Keckley said. “We have a 77- year-old challenger and a 74-year-old incumbent. Voters are expecting the odds are one will become disabled and the vice president is going to step in. That’s the undercurrent of this debate.”
Healthcare is an obvious dominant theme Wednesday night beyond the health of the two men seeking the presidency.
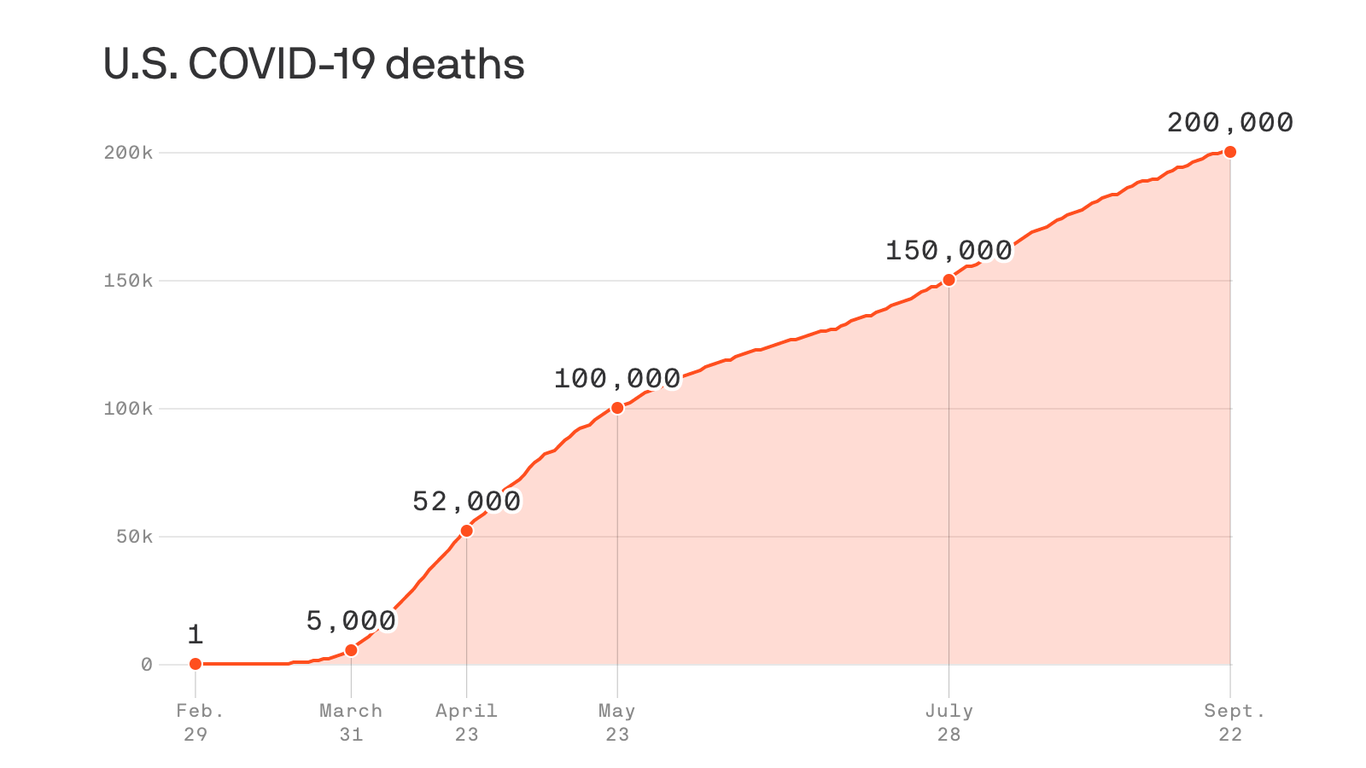
It is expected that Biden’s running mate, Kamala Harris will challenge Vice President Mike Pence on his role heading the coronavirus task force when close to 7.5 million people in this country have been infected with COVID-19 and more than 200,000 have died.
Pence will likely challenge Harris on her support for Medicare for All before she backtracked to support Biden’s public-private option for healthcare coverage.
Pence and Harris are expected to lay out the healthcare plans of their respective Republican and Democratic nominees less than four weeks before the election, in a way the lead candidates failed to get across during the first presidential debate that presented more chaos than clarity.
TRUMP AND BIDEN PLANS
Trump and Biden differ fundamentally on whether the federal government should be involved in the business of providing healthcare coverage.
Trump’s guiding principles rest on the pillar of state autonomy as opposed to a federalized healthcare system and Biden’s maxim that healthcare is a right, not a privilege.
Trump believes that private solutions are better than government solutions, according to Keckley. He is much less restrained on private equity and the Federal Trade Commission’s scrutiny of vertical integration. States become the gateway to the market as private solutions are sold to states as innovation.
Trump’s other concept is that the door to engaging consumers in healthcare is price transparency. His view is that price transparency will spawn consumer engagement.
Centers for Medicare and Medicaid Services Administrator Seema Verma, who was appointed by Trump in 2016 based largely on the recommendation of Pence, is instituting a rule, starting January 1, 2021, requiring hospitals to have price transparency for 300 shoppable services. Hospitals are being required to make their contract terms with payer accessible.
This is separate from CMS’s interoperability rule aimed at payers that also goes into effect on January 1.
Trump believes healthcare is a personal responsibility, not a public obligation. To Trump, healthcare is a marketplace where there are winners and losers, according to Keckley.
Biden has a more developed policy platform on making healthcare a universal right, starting with strengthening the Affordable Care Act that was passed while Biden was vice president during President Barack Obama’s terms.
Biden wants to increase the eligibility for tax subsidies in the ACA up to 400% of the federal poverty level, which would expand access to subsidized health insurance.
He also wants to reduce the affordability threshold for employer insurance. Currently, if employees pay more than 9.7% of their adjusted income for their workplace coverage, they can seek a plan in the ACA marketplace. Biden would lower that eligibility for ACA coverage to 8.5%, opening the door for many more consumers to be insured through the ACA, at a lower cost.
Biden would also lower the age of eligibility for Medicare from 65 to 60.
For companies such as manufacturing and transportation, in which individuals can retire after 30 years of service, this lets them into the Medicare system earlier to fill that gap between retirement and Medicare eligibility.
Biden’s public option would create insurance plans that would compete with private plans.
The other factor to watch on the Biden side, Keckley said, is his clear focus on equity and diversity in healthcare.
AFFORDABLE CARE ACT
Biden wants to strengthen Obamacare while Trump is actively pursuing a repeal of the law through the Supreme Court.
President Trump’s debate prep and the White House Rose Garden event announcing the nomination of Judge Amy Coney Barrett to replace the late Supreme Court Justice Ruth Bader Ginsburg, border on the definition of super spreader events.
The Justices, perhaps with the addition of Trump’s pick, Amy Coney Barrett, if there are enough Republican senators well enough and in attendance to vote for confirmation, are scheduled to hear oral arguments in the case brought by 18 GOP-led states on November 10, the week after the election.
Senators must be present to vote, and Republicans, who have a majority of 53 to 47 seats, need a four-vote majority. Two Republican senators – Susan Collins of Maine and Lisa Murkowski of Alaska – have said they wouldn’t vote on a nominee prior to the election. Vice President Mike Pence could cast the deciding vote in a tie.
Three Republican senators have tested positive for the coronavirus. Sens. Mike Lee of Utah and Thom Tillis of North Carolina, who sit on the Judiciary Committee, tested positive for COVID-19 days after attending the White House Rose Garden event on September 26. Republican Sen. Ron Johnson of Wisconsin is now the third to test positive, though he did not attend that event.
There was a lack of social distancing and mask wearing at both the Rose Garden nomination and at a meeting between Trump and staff for debate prep. Twelve people in Trump’s inner circle, including his wife Melania, former New Jersey governor Chris Christie and White House Press Secretary Kayleigh McEnany, have tested positive since attending.
Senate Majority Leader Mitch McConnell wrote in an email to GOP senators obtained by CNN that he needs all Republican senators back in Washington by October 19.
COVID-19
Trump announced in a tweet Monday that he would be leaving Walter Reed later in the afternoon, saying he felt “really good!” and adding, “Don’t be afraid of Covid. Don’t let it dominate your life. We have developed, under the Trump Administration, some really great drugs & knowledge. I feel better than I did 20 years ago!”
Trump has been criticized for leaving the hospital on Monday to take a drive-by ride to wave to supporters. Attending physician Dr. James Phillips called the action “insanity” and “political theater” that put the lives of Secret Service agents in the car with him at risk.
Trump has downplayed the virus in an effort to reopen the country and the economy, and has put the blame on China, where the coronavirus originated.
Trump told Biden during the debate, “We got the gowns; we got the masks; we made the ventilators. You wouldn’t have made ventilators – and now we’re weeks away from a vaccine.”
Biden puts the blame squarely on Trump for delaying action to stop the spread.
Biden said during the debate: “Look, 200,000 dead. You said over seven million infected in the United States. We in fact have 5% or 4% of the world’s population – 20% of the deaths. Forty thousand people a day are contracting COVID. In addition to that, about between 750 and 1,000 people, they’re dying. When [Trump] was presented with that number he said ‘It is what it is’ – what it is what it is – because you are who you are. That’s why it is. The president has no plan. He hasn’t laid out anything.”
Biden said that back in July he laid out a plan for providing protective gear and providing money the House passed to get people the help they need to keep their businesses open and open schools.
Under Trump’s Administration, Congress passed $175 billion in provider relief funds for hospitals, small businesses, individuals and others – $100 billion from the CARES Act and $75 billion from the Paycheck Protection Program and Healthcare Enhancement Act.
MEDICAID EXPANSION
CMS Administrator Seema Verma was healthcare advisor to Pence while he was governor of Indiana. Her consulting firm, SVC, Inc., worked closely with Pence to design Indiana’s Medicaid expansion under the Affordable Care Act. They developed a unique Medicaid expansion program called Health Indiana Plan 2.0, which mandated low income adults above the poverty level pay monthly premiums for their healthcare.
Members who did not pay faced being disenrolled for six months.
As administrator, Verma has initiated similar work requirements for Medicaid coverage nationwide.
While as governor Pence implemented Medicaid expansion, as vice president he has supported torpedoing the ACA, and has pushed the Graham-Cassidy plan for healthcare reform that would have replaced the ACA.
DRUG PRICES
Neither Trump nor Biden has taken on the pharmaceutical industry in a meaningful way, though both have voiced a strong belief that drug manufacturers are egregious to the system, according to Keckley.
“Both camps are saying, we’re really going to take them on,” he said.
During the debate, Trump said he was cutting drug prices by allowing American consumers to buy drugs from Canada and other countries under a favored nation status.
“Drug prices will be coming down, 80 or 90 percent,” Trump said during the debate, telling Biden he hadn’t done anything similar during his 47 years in government.
If Trump gets a second term, there will likely be more industry folks in his circle, following up on his first term of stacking his cabinet with business people.
Biden would be more likely to lean toward a blend of public health officials and industry executives. There would be more of a spotlight on wealth creation in healthcare and executive pay.
In the $1.1 trillion world of prescription drugs, the United States makes up 40% of the market.
“We’re the hub of the prescription drug industry,” Keckley said.