One hesitates to elevate obviously bad arguments, even to point out how bad they are. This is a conundrum that comes up a lot these days, as members of the media measure the utility of reporting on bad faith, disingenuous or simply bizarre claims.
If someone were to insist, for example, that they were not going to get the coronavirus vaccine solely to spite the political left, should that claim be elevated? Can we simply point out how deranged it is to refuse a vaccine that will almost certainly end an international pandemic simply because people with whom you disagree think that maybe this is a good route to end that pandemic? If someone were to write such a thing at some attention-thirsty website, we certainly wouldn’t want to link to it, leaving our own readers having to figure out where it might be found should they choose to do so.
In this case, it’s worth elevating this argument (which, to be clear, is actually floating out there) to point out one of the myriad ways in which the effort to vaccinate as many adults as possible has become interlaced with partisan politics. As the weeks pass and demand for the vaccine has tapered off, the gap between Democratic and Republican interest in being vaccinated seems to be widening — meaning that the end to the pandemic is likely to move that much further into the future.
Consider, for example, the rate of completed vaccinations by county, according to data compiled by CovidActNow. You can see a slight correlation between how a county voted in 2020 — the horizontal axis — and the density of completed vaccinations, shown on the vertical. There’s a greater density of completed vaccinations on the left side of the graph than on the right.
If we shift to the percentage of the population that’s received even one dose of the vaccine, the effect is much more obvious.
This is a relatively recent development. At the beginning of the month, the density of the population that had received only one dose resulted in a graph that looked much like the current density of completed doses.
If we animate those two graphs, the effect is obvious. In the past few weeks, the density of first doses has increased much faster in more-Democratic counties.
If we group the results of the 2020 presidential contest into 20-point buckets, the pattern is again obvious.
It’s not a new observation that Republicans are less willing to get the vaccine; we’ve reported on it repeatedly. What’s relatively new is how that hesitance is showing up in the actual vaccination data.
A Post-ABC News poll released on Monday showed that this response to the vaccine holds even when considering age groups. We’ve known for a while that older Americans, who are more at risk from the virus, have been more likely to seek the vaccine. But even among seniors, Republicans are significantly more hesitant to receive the vaccine than are Democrats.
This is a particularly dangerous example of partisanship. People 65 or older have made up 14 percent of coronavirus infections, according to federal data, but 81 percent of deaths. That’s among those for whom ages are known, a subset (though a large majority) of overall cases. While about 1.8 percent of that overall group has died, the figure for those aged 65 and over is above 10 percent.
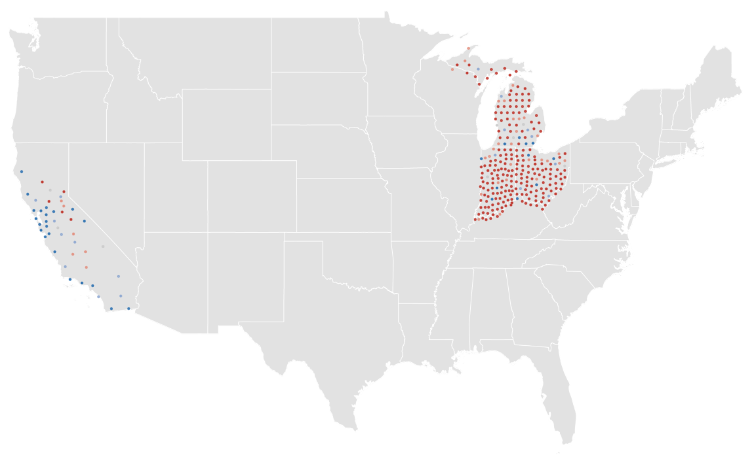
As vaccines have been rolled out across the country, you can see how more-heavily-blue counties have a higher density of vaccinations in many states.
This is not a universal truth, of course. Some heavily Republican counties have above-average vaccination rates. (About 40 percent of counties that preferred former president Donald Trump last year are above the average in the CovidActNow data. The rate among Democratic counties is closer to 80 percent.) But it is the case that there is a correlation between how a county voted and how many of its residents have been vaccinated. It is also the case that the gap between red and blue counties is widening.
Given all of that, it probably makes sense to point out that an argument against vaccines based on nothing more than “lol libs will hate this” is an embarrassing argument to make.
The CDC and FDA on Friday lifted the recommended pause on use of Johnson & Johnson’s coronavirus vaccine, saying the benefits of the shot outweigh the risk of a rare blood clot disorder.
Why it matters: The move clears the way for states to immediately resume administering the one-shot vaccine.
The Johnson & Johnson shot had been seen as an important tool to fill gaps in the U.S. vaccination effort. But between the pause in its use and repeated manufacturing problems, its role in that effort is shrinking.
Driving the news:J&J shots have been paused for about two weeks, in response to reports that they may have caused serious blood clots in a small number of patients.
Only six people had experienced those blood clots at the time of the pause. The CDC said Friday that there have been nine additional cases.
Regulators said the number is small enough to safely resume the use of J&J’s vaccine.
What they’re saying: “Safety is our top priority. This pause was an example of our extensive safety monitoring working as they were designed to work — identifying even these small number of cases,” said acting FDA Commissioner Janet Woodcock.
“We’ve lifted the pause based on the FDA and CDC’s review of all available data and in consultation with medical experts and based on recommendations from the CDC’s Advisory Committee on Immunization Practices,” she said.
“We are confident that this vaccine continues to meet our standards for safety, effectiveness and quality.”
What’s next: Regulators said health care providers administering the shot and vaccine recipients should review revised fact sheets about the J&J vaccine, which includes information about the rare blood clot disorder.
That heightened attention is important because the standard treatment for blood clots can make this particular type of clot worse.
Yes, but:J&J was already a relatively small part of the overall domestic vaccination effort, in part because the company missed some of its early manufacturing targets.
Multiple problems have since emerged at a Baltimore facility that makes a key ingredient for the vaccine, which could sideline production for weeks.
Of 26 health systems surveyed by MedCity News, nearly half used automated tools to respond to the Covid-19 pandemic, but none of them were regulated. Even as some hospitals continued using these algorithms, experts cautioned against their use in high-stakes decisions.
A year ago, Michigan Medicine faced a dire situation. In March of 2020, the health system predicted it would have three times as many patients as its 1,000-bed capacity — and that was the best-case scenario. Hospital leadership prepared for this grim prediction by opening a field hospital in a nearby indoor track facility, where patients could go if they were stable, but still needed hospital care. But they faced another predicament: How would they decide who to send there?
Two weeks before the field hospital was set to open, Michigan Medicine decided to use a risk model developed by Epic Systems to flag patients at risk of deterioration. Patients were given a score of 0 to 100, intended to help care teams determine if they might need an ICU bed in the near future. Although the model wasn’t developed specifically for Covid-19 patients, it was the best option available at the time, said Dr. Karandeep Singh, an assistant professor of learning health sciences at the University of Michigan and chair of Michigan Medicine’s clinical intelligence committee. But there was no peer-reviewed research to show how well it actually worked.
Researchers tested it on over 300 Covid-19 patients between March and May. They were looking for scores that would indicate when patients would need to go to the ICU, and if there was a point where patients almost certainly wouldn’t need intensive care.
“We did find a threshold where if you remained below that threshold, 90% of patients wouldn’t need to go to the ICU,” Singh said. “Is that enough to make a decision on? We didn’t think so.”
But if the number of patients were to far exceed the health system’s capacity, it would be helpful to have some way to assist with those decisions.
“It was something that we definitely thought about implementing if that day were to come,” he said in a February interview.
Thankfully, that day never came.
The survey Michigan Medicine is one of 80 hospitals contacted by MedCity News between January and April in a survey of decision-support systems implemented during the pandemic. Of the 26 respondents, 12 used machine learning tools or automated decision systems as part of their pandemic response. Larger hospitals and academic medical centers used them more frequently.
Faced with scarcities in testing, masks, hospital beds and vaccines, several of the hospitals turned to models as they prepared for difficult decisions. The deterioration index created by Epic was one of the most widely implemented — more than 100 hospitals are currently using it — but in many cases, hospitals also formulated their own algorithms.
They built models to predict which patients were most likely to test positive when shortages of swabs and reagents backlogged tests early in the pandemic. Others developed risk-scoring tools to help determine who should be contacted first for monoclonal antibody treatment, or which Covid patients should be enrolled in at-home monitoring programs.
MedCity News also interviewed hospitals on their processes for evaluating software tools to ensure they are accurate and unbiased. Currently, the FDA does not require some clinical decision-support systems to be cleared as medical devices, leaving the developers of these tools and the hospitals that implement them responsible for vetting them.
Among the hospitals that published efficacy data, some of the models were only evaluated through retrospective studies. This can pose a challenge in figuring out how clinicians actually use them in practice, and how well they work in real time. And while some of the hospitals tested whether the models were accurate across different groups of patients — such as people of a certain race, gender or location — this practice wasn’t universal.
As more companies spin up these models, researchers cautioned that they need to be designed and implemented carefully, to ensure they don’t yield biased results.
An ongoing review of more than 200 Covid-19 risk-prediction models found that the majority had a high risk of bias, meaning the data they were trained on might not represent the real world.
“It’s that very careful and non-trivial process of defining exactly what we want the algorithm to be doing,” said Ziad Obermeyer, an associate professor of health policy and management at UC Berkeley who studies machine learning in healthcare. “I think an optimistic view is that the pandemic functions as a wakeup call for us to be a lot more careful in all of the ways we’ve talked about with how we build algorithms, how we evaluate them, and what we want them to do.”
Algorithms can’t be a proxy for tough decisions Concerns about bias are not new to healthcare. In a paper published two years ago, Obermeyer found a tool used by several hospitals to prioritize high-risk patients for additional care resources was biased against Black patients. By equating patients’ health needs with the cost of care, the developers built an algorithm that yielded discriminatory results.
More recently, a rule-based system developed by Stanford Medicine to determine who would get the Covid-19 vaccine first ended up prioritizing administrators and doctors who were seeing patients remotely, leaving out most of its 1,300 residents who had been working on the front lines. After an uproar, the university attributed the errors to a “complex algorithm,” though there was no machine learning involved.
Both examples highlight the importance of thinking through what exactly a model is designed to do — and not using them as a proxy to avoid the hard questions.
“The Stanford thing was another example of, we wanted the algorithm to do A, but we told it to do B. I think many health systems are doing something similar,” Obermeyer said. “You want to give the vaccine first to people who need it the most — how do we measure that?”
The urgency that the pandemic created was a complicating factor. With little information and few proven systems to work with in the beginning, health systems began throwing ideas at the wall to see what works. One expert questioned whether people might be abdicating some responsibility to these tools.
“Hard decisions are being made at hospitals all the time, especially in this space, but I’m worried about algorithms being the idea of where the responsibility gets shifted,” said Varoon Mathur, a technology fellow at NYU’s AI Now Institute, in a Zoom interview. “Tough decisions are going to be made, I don’t think there are any doubts about that. But what are those tough decisions? We don’t actually name what constraints we’re hitting up against.”
The wild, wild west There currently is no gold standard for how hospitals should implement machine learning tools, and little regulatory oversight for models designed to support physicians’ decisions, resulting in an environment that Mathur described as the “wild, wild west.”
How these systems were used varied significantly from hospital to hospital.
Early in the pandemic, Cleveland Clinic used a model to predict which patients were most likely to test positive for the virus as tests were limited. Researchers developed it using health record data from more than 11,000 patients in Ohio and Florida, including 818 who tested positive for Covid-19. Later, they created a similar risk calculator to determine which patients were most likely to be hospitalized for Covid-19, which was used to prioritize which patients would be contacted daily as part of an at-home monitoring program.
Initially, anyone who tested positive for Covid-19 could enroll in this program, but as cases began to tick up, “you could see how quickly the nurses and care managers who were running this program were overwhelmed,” said Dr. Lara Jehi, Chief Research Information Officer at Cleveland Clinic. “When you had thousands of patients who tested positive, how could you contact all of them?”
While the tool included dozens of factors, such as a patient’s age, sex, BMI, zip code, and whether they smoked or got their flu shot, it’s also worth noting that demographic information significantly changed the results. For example, a patient’s race “far outweighs” any medical comorbidity when used by the tool to estimate hospitalization risk, according to a paper published in Plos One. Cleveland Clinic recently made the model available to other health systems.
Others, like Stanford Health Care and 731-bed Santa Clara County Medical Center, started using Epic’s clinical deterioration index before developing their own Covid-specific risk models. At one point, Stanford developed its own risk-scoring tool, which was built using past data from other patients who had similar respiratory diseases, such as the flu, pneumonia, or acute respiratory distress syndrome. It was designed to predict which patients would need ventilation within two days, and someone’s risk of dying from the disease at the time of admission.
Stanford tested the model to see how it worked on retrospective data from 159 patients that were hospitalized with Covid-19, and cross-validated it with Salt Lake City-based Intermountain Healthcare, a process that took several months. Although this gave some additional assurance — Salt Lake City and Palo Alto have very different populations, smoking rates and demographics — it still wasn’t representative of some patient groups across the U.S.
“Ideally, what we would want to do is run the model specifically on different populations, like on African Americans or Hispanics and see how it performs to ensure it’s performing the same for different groups,” Tina Hernandez-Boussard, an associate professor of medicine, biomedical data science and surgery at Stanford, said in a February interview. “That’s something we’re actively seeking. Our numbers are still a little low to do that right now.”
Stanford planned to implement the model earlier this year, but ultimately tabled it as Covid-19 cases fell.
‘The target is moving so rapidly’ Although large medical centers were more likely to have implemented automated systems, there were a few notable holdouts. For example, UC San Francisco Health, Duke Health and Dignity Health all said they opted not to use risk-prediction models or other machine learning tools in their pandemic responses.
“It’s pretty wild out there and I’ll be honest with you — the dynamics are changing so rapidly,” said Dr. Erich Huang, chief officer for data quality at Duke Health and director of Duke Forge. “You might have a model that makes sense for the conditions of last month but do they make sense for the conditions of next month?”
That’s especially true as new variants spread across the U.S., and more adults are vaccinated, changing the nature and pace of the disease. But other, less obvious factors might also affect the data. For instance, Huang pointed to big differences in social mobility across the state of North Carolina, and whether people complied with local restrictions. Differing social and demographic factors across communities, such as where people work and whether they have health insurance, can also affect how a model performs.
“There are so many different axes of variability, I’d feel hard pressed to be comfortable using machine learning or AI at this point in time,” he said. “We need to be careful and understand the stakes of what we’re doing, especially in healthcare.”
Leadership at one of the largest public hospitals in the U.S., 600-bed LAC+USC Medical Center in Los Angeles, also steered away from using predictive models, even as it faced an alarming surge in cases over the winter months.
At most, the hospital used alerts to remind physicians to wear protective equipment when a patient has tested positive for Covid-19.
“My impression is that the industry is not anywhere near ready to deploy fully automated stuff just because of the risks involved,” said Dr. Phillip Gruber, LAC+USC’s chief medical information officer. “Our institution and a lot of institutions in our region are still focused on core competencies. We have to be good stewards of taxpayer dollars.”
When the data itself is biased Developers have to contend with the fact that any model developed in healthcare will be biased, because the data itself is biased; how people access and interact with health systems in the U.S. is fundamentally unequal.
How that information is recorded in electronic health record systems (EHR) can also be a source of bias, NYU’s Mathur said. People don’t always self-report their race or ethnicity in a way that fits neatly within the parameters of an EHR. Not everyone trusts health systems, and many people struggle to even access care in the first place.
“Demographic variables are not going to be sharply nuanced. Even if they are… in my opinion, they’re not clean enough or good enough to be nuanced into a model,” Mathur said.
The information hospitals have had to work with during the pandemic is particularly messy. Differences in testing access and missing demographic data also affect how resources are distributed and other responses to the pandemic.
“It’s very striking because everything we know about the pandemic is viewed through the lens of number of cases or number of deaths,” UC Berkeley’s Obermeyer said. “But all of that depends on access to testing.”
At the hospital level, internal data wouldn’t be enough to truly follow whether an algorithm to predict adverse events from Covid-19 was actually working. Developers would have to look at social security data on mortality, or whether the patient went to another hospital, to track down what happened.
“What about the people a physician sends home — if they die and don’t come back?” he said.
Researchers at Mount Sinai Health System tested a machine learning tool to predict critical events in Covid-19 patients — such as dialysis, intubation or ICU admission — to ensure it worked across different patient demographics. But they still ran into their own limitations, even though the New York-based hospital system serves a diverse group of patients.
They tested how the model performed across Mount Sinai’s different hospitals. In some cases, when the model wasn’t very robust, it yielded different results, said Benjamin Glicksberg, an assistant professor of genetics and genomic sciences at Mount Sinai and a member of its Hasso Plattner Institute for Digital Health.
They also tested how it worked in different subgroups of patients to ensure it didn’t perform disproportionately better for patients from one demographic.
“If there’s a bias in the data going in, there’s almost certainly going to be a bias in the data coming out of it,” he said in a Zoom interview. “Unfortunately, I think it’s going to be a matter of having more information that can approximate these external factors that may drive these discrepancies. A lot of that is social determinants of health, which are not captured well in the EHR. That’s going to be critical for how we assess model fairness.”
Even after checking for whether a model yields fair and accurate results, the work isn’t done yet. Hospitals must continue to validate continuously to ensure they’re still working as intended — especially in a situation as fast-moving as a pandemic.
A bigger role for regulators All of this is stirring up a broader discussion about how much of a role regulators should have in how decision-support systems are implemented.
Of the hospitals surveyed by MedCity News, none of the models they developed had been cleared by the FDA, and most of the external tools they implemented also hadn’t gone through any regulatory review.
“My experience suggests that most models are put into practice with very little evidence of their effects on outcomes because they are presumed to work, or at least to be more efficient than other decision-making processes,” Kellie Owens, a researcher for Data & Society, a nonprofit that studies the social implications of technology, wrote in an email. “I think we still need to develop better ways to conduct algorithmic risk assessments in medicine. I’d like to see the FDA take a much larger role in regulating AI and machine learning models before their implementation.”
Developers should also ask themselves if the communities they’re serving have a say in how the system is built, or whether it is needed in the first place. The majority of hospitals surveyed did not share with patients if a model was used in their care or involve patients in the development process.
In some cases, the best option might be the simplest one: don’t build.
In the meantime, hospitals are left to sift through existing published data, preprints and vendor promises to decide on the best option. To date, Michigan Medicine’s paper is still the only one that has been published on Epic’s Deterioration Index.
Care teams there used Epic’s score as a support tool for its rapid response teams to check in on patients. But the health system was also looking at other options.
“The short game was that we had to go with the score we had,” Singh said. “The longer game was, Epic’s deterioration index is proprietary. That raises questions about what is in it.”
There’s a lot of anxiety about the AstraZeneca vaccine thanks to recent reports of incomplete data, as well as reports on blood clot risks. Let’s take a look at both issues in context, understanding the efficacy data before and after numbers were updated, and understanding blood clot risk in relation to other common situations where blood clots are a potential concern.
As states rush to fully reopen businesses, and Americans leave their masks at home in greater numbers, it appears that the feared “fourth surge” of COVID is now underway in many parts of the country.Coronavirus cases are up in half of all states, and up nationally by 9 percent compared to last week. While the latest wave appears to be much less deadly—largely targeting younger people who haven’t yet been vaccinated—it adds urgency to the effort to get shots in arms as quickly as possible.
The good news: that’s happening. Today the US surpassed the milestone of 200M vaccinations given, with nearly a quarter of the population now fully vaccinated (including nearly two-thirds of those over age 65). The progress on vaccines comes as the Johnson & Johnson COVID jab is sidelined, over safety concerns stemming from a small number of rare blood-clotting cases in younger women that caused the Food and Drug Administration (FDA) and the Centers for Disease Control and Prevention (CDC) to urge states to pause the use of the shot. Wednesday’s inconclusive meeting of the FDA’s Advisory Committee on Immunization Practices meant an additional 7 to 10 days of limbo for the J&J vaccine, drawing criticism from experts who warned that the negative publicity could undermine confidence in vaccines among the general population, both in the US and around the world.
Count us among those skeptical of the decision to pull back on the J&J vaccine, which plays a pivotal role in the campaign against COVID, given that it’s a single-dose vaccine that can be stored at normal refrigerator temperatures, making it more easily distributed than the two-dose mRNA vaccines. While the blood clotting cases are serious, and merit investigation, the odds of suffering a vaccine-related blood clot are far outweighed by an individual’s risk of death or severe complications from COVID itself, let alone the chances of getting a blood clot from other medications (such as oral contraceptives).
It was a big week for innumeracy, unfortunately: headlinesabounded about the CDC’s discovery of 5,800 “breakthrough” COVID cases, in which fully vaccinated people still contracted the disease. Unsurprisingly, the numerator got the headlines, not the denominator—the 80M people who’ve been fully vaccinated. Your chances of hitting a hole-in-one as an amateur golfer are better than the chances of getting COVID after being fully vaccinated. Furthermore, of those 5,800 people infected after being fully vaccinated, only 7 percent were hospitalized, and 74 died. Each a tragedy, to be sure—but we’ll take those odds any day.
It was a relatively quiet week on the COVID front—so quiet that President Biden held his first White House press conference last week and wasn’t asked a single question about the pandemic, which continues to be a race between vaccinations and virus variants.
Not that nothing happened this week: it was a rocky week for AstraZeneca, which was hoping to change the narrative over its vaccine, which has stumbled in its rollout in Europe, by reporting positive results from US trials.
After a press release announcing that the vaccine was found to be 79 percent effective against symptomatic COVID, an independent review board called the results into question, pointing out that the report was based on data that had not been fully updated. That earned a swift and unusual rebuke from the National Institutes of Health (NIH), forcing the company to correct its findings—to 76 percent.
A relatively minor difference, but the dust-up served to further undermine confidence in the company’s COVID jab, especially troubling in Europe where hesitancy and distribution have been a vexing problem, and concerns about blood clots associated with the AstraZeneca shot caused several countries to pause inoculations. Given the supply of already-approved vaccines from other manufacturers in the US, it’s not clear that the AstraZeneca shot will play a big role here, but it is critical in other parts of the world, especially as part of the global COVAX initiative targeted at developing countries, since the vaccine can be stored at normal refrigerator temperatures.
The company’s set-to with American regulators also highlighted another challenge that’s become common during the COVID pandemic: conducting scientific review by press release, as the global emergency has required the otherwise slow-moving research community to move at lightning pace.
Meanwhile, back at that relatively dull White House press conference, one piece of encouraging news:President Biden doubled his “first 100 days” goal for vaccinations to 200M shots, a goal that seemswholly achievable, given that 2.5M Americans are being vaccinated every day, on average.
Xavier Becerra narrowly won confirmation Thursday to lead the Department of Health and Human Services, the agency pivotal to President Biden’s urgent goal of defeating the coronavirus pandemic and expanding access to health care.
Becerra, a congressman from Los Angeles for two dozen years and then California attorney general, squeaked by on a vote of 50 to 49, the closest margin for any of the Biden cabinet members the Senate has confirmed so far.
He becomes the first Latino secretary of HHS, the largest federal department in terms of spending. The department includes agencies at the core of the federal response to the pandemic that has infected more than 29.5 million people in the United States and killed more than 535,000. They include the National Institutes of Health, the Centers for Disease Control and Prevention, the vaccine-approving Food and Drug Administration, and the Centers for Medicare and Medicaid Services, which oversees the country’s vast public insurance programs.
Sen. Ron Wyden (D-Ore.), chairman of the Senate Finance Committee, which considered the nomination, said that “after four years of going in reverse,” Becerra will make it “possible to go to drive and actually make progress for the American people, progress in terms of lowering the cost of health care.”
Republican Sen. John Barrasso (Wyo.), countered that Becerra is “an aggressive culture warrior from the radical left,” who is “out of touch with the views of the American people.” Barrasso noted that, as state attorney general, Becerra sued the Trump administration more than 150 times over immigration, environmental and health policies.
“In this time of crisis, our secretary of Health and Human Services may be the single most important member of the president’s cabinet,” Barrasso said, contending that “the president has chosen a nominee, no public health experience, extremely partisan record.”
Sen. Susan Collins (R-Maine) was the only member of the GOP to vote for Becerra’s confirmation along with a solid wall of Senate Democrats.
During his confirmation hearing last month before the Senate Finance Committee, Becerra said, “The mission of HHS — to enhance the health and well-being of all Americans — is core to who I am.”
In keeping with Biden’s emphasis on portraying his administration’s top rung as diverse and having working-class roots like his own, Becerra told the senators his immigrant parents had insurance through his father’s laborers union, making his family more fortunate when he was a boy than many of their neighbors.
As a longtime member of the House Ways and Means Committee, Becerra testified, he worked on several major pieces of health-care legislation, including the Children’s Health Insurance Program created in the late 1990s and changes to the way Medicare is run and financed, as well as the Affordable Care Act.
He did not mention that he was a longtime advocate of a single-payer health-care system, akin to the Medicare-for-all proposals backed by several Democratic candidates in last year’s presidential election, but rejected by Biden. Becerra has renounced his previous support since his nomination, echoing the president’s view that affordable insurance coverage should be widened by building upon the ACA.
Becerra, 63, became a lightning rod for conservatives immediately after Biden announced his selection in early December.
Senate Republicans targeted his defense of abortion rights. They contended he is unqualified because he is not a physician, though few HHS secretaries have had medical training. And they have denounced his previous advocacy of a larger government role in health insurance.
An undercurrent running through opposition to his nomination was Becerra’s leadership in recent years of a coalition of Democratic attorneys general fighting to preserve the ACA. Republicans, including President Donald Trump, are seeking to overturn the 2010 law in a case now before the Supreme Court.
Sen. James Inhofe (R-Okla.) lambasted Becerra, saying he has “an appalling track record disrespecting the sanctity of life. . . . He has no shame when it comes to his pro-abortion beliefs.”
Inhofe also criticized Becerra’s support last year for California’s ban on indoor worship services as part of the state’s efforts to slow the cornavirus’s spread. And the senator criticized Becerra’s position that undocumented immigrants should be allowed public benefits, such as Medicaid.
Senate Majority Leader Charles E. Schumer (D-N.Y.) said Republicans’ arguments against Becerra “almost verge on the ridiculous.”
Schumer said Republicans challenging Becerra’s qualifications for the job had embraced the nomination of Alex Azar as Trump’s second HHS secretary, though he was a pharmaceutical executive who also was an attorney and had no medical training.
In addition to working to tame the pandemic, which Biden has identified as the government’s job number one for now, Becerra will face many major decisions at the helm of the sprawling department over whether to continue or reverse policies established by the Trump administration.
CMS has already announced it was rescinding a significant Medicaid policy of the Trump era that had allowed states to require some residents to hold a job or be preparing for work to qualify for the safety-net insurance program. HHS officials are reviewing other Trump-era Medicaid policies.
Another HHS agency, the Administration for Children and Families, oversees the nation’s policies regarding welfare and unaccompanied children coming across the country’s borders — a flashpoint during the Trump administration.
The CDC, the government’s public-health agency, has been working to regain its footing and scientific moorings after repeated intrusions into its advice to the public by the Trump White House. The agency has been involved in the largest mass vaccination campaign in U.S. history to immunize the public against the coronavirus. And it is developing guidance on aspects of American life — and ongoing public safety measures — as research findings evolve for the virus and vaccine’s effects.
The FDA is in the thick of decisions about coronavirus vaccines, developed in record time, as additional manufacturers, such as AstraZeneca, have devised them and tested their safety and effectiveness. The three vaccines being given to about 2 million Americans a day — by Pfizer-BioNTech, Moderna and Johnson & Johnson — are being allowed so far for emergency use and have not yet secured full FDA approval.
Becerra almost certainly will continue to face hostility from social conservatives after his swearing in, expected Friday.
Roger Severino, who led HHS’s Office for Civil Rights during the Trump administration and created a division to promote “conscience and religious freedom,” is building an “HHS Accountability Project” within the conservative Ethics and Public Policy Center.
While at HHS, Severino tangled directly with Becerra during his tenure as attorney general of the nation’s most populous state, twice citing him in violation of federal laws for upholding California statutes involving abortion rights.
Severino said this week he believes those on the right might find common ground with Biden health officials on disability rights. But on matters of abortion and deference to religion, Severino said, “We will be watching.”
The COVID-19 pandemic has accelerated the pace of artificial intelligence adoption, and healthcare leaders are confident AI can help solve some of today’s toughest challenges, including COVID-19 tracking and vaccines.
The majority of healthcare and life sciences executives (82%) want to see their organizations more aggressively adopt AI technology, according to a new survey from KPMG, an audit, tax and advisory services firm.
Healthcare and life sciences (56%) business leaders report that AI initiatives have delivered more value than expected for their organizations. However, life sciences companies seem to be struggling to select the best AI technologies, according to 73% of executives.
As the U.S. continues to navigate the pandemic, life sciences business leaders are overwhelmingly confident in AI’s ability to monitor the spread of COVID-19 cases (94%), help with vaccine development (90%) and aid vaccine distribution (90%).
KPMG’s AI survey is based on feedback from 950 business or IT decision-makers across seven industries, with 100 respondents each from healthcare and life sciences companies.
Despite the optimism about the potential for AI, executives across industries believe more controls are needed and overwhelmingly believe the government has a role to play in regulating AI technology. The majority of life sciences (86%) and healthcare (84%) executives say the government should be involved in regulating AI technology.
And executives across industries are optimistic about the new administration in Washington, D.C., with the majority believing the Biden administration will do more to help advance the adoption of AI in the enterprise.
“We are seeing very high levels of support this year across all industries for more AI regulation. One reason for this may be that, as the technology advances very quickly, insiders want to avoid AI becoming the ‘Wild Wild West.’ Additionally, a more robust regulatory environment may help facilitate commerce. It can help remove unintended barriers that may be the result of other laws or regulations, or due to lack of maturity of legal and technical standards,” said Rob Dwyer, principal, advisory at KPMG, specializing in technology in government.
Healthcare and pharma companies seem to be more bullish on AI than other industries are.
The survey found half of business leaders in industrial manufacturing, retail and tech say AI is moving faster than it should in their industry. Concerns about the speed of AI adoption are particularly pronounced among small companies (63%), business leaders with high AI knowledge (51%) and Gen Z and millennial business leaders (51%).
“Leaders are experiencing COVID-19 whiplash, with AI adoption skyrocketing as a result of the pandemic. But many say it’s moving too fast. That’s probably because of current debate surrounding the ethics, governance and regulation of AI. Many business leaders do not have a view into what their organizations are doing to control and govern AI and may fear risks are developing,” Traci Gusher, principal of artificial intelligence at KPMG, said in a statement.
Future AI investment
Healthcare organizations are ramping up their investments in AI in response to the COVID-19 pandemic. In a Deloitte survey, nearly 3 in 4 healthcare organizations said they expect to increase their AI funding, with executives citing making processes more efficient as the top outcome they are trying to achieve with AI.
Healthcare executives say current AI investments at their organizations have focused on electronic health record (EHR) management and diagnosis.
To date, the technology has proved its value in reducing errors and improving medical outcomes for patients, according to executives. Around 40% of healthcare executives said AI technology has helped with patient engagement and also to improve clinical quality. About a third of executives said AI has improved administrative efficiency. Only 18% said the technology helped uncover new revenue opportunities.
But AI investments will shift over the next two years to prioritize telemedicine (38%), robotic tasks such as process automation (37%) and delivery of patient care (36%), the survey found. Clinical trials and diagnosis rounded out the top five investment areas.
At life sciences companies, AI is primarily deployed during the drug development process to improve record-keeping and the application process, the survey found. Companies also have leveraged AI to help with clinical trial site selection.
Moving forward, pharmaceutical companies will likely focus their AI investments on discovering new revenue opportunities in the next two years, a pivot from their current strategy focusing on increasing profitability of existing products, according to the survey. About half of life sciences executives say their organizations plan to leverage AI to reduce administrative costs, analyze patient data and accelerate clinical trials.
Industry stakeholders are taking steps to advance the use of AI and machine learning in healthcare.
The Consumer Technology Association (CTA) created a working group two years ago to develop some standardization on definitions and characteristics of healthcare AI. Last year, the CTA working group developed a standard that creates a common language so industry stakeholders can better understand AI technologies. A group also recently developed a new standard to advance trust in AI solutions.
On the regulatory front, the U.S. Food and Drug Administration (FDA) last month released its first AI and machine learning action plan, a multistep approach designed to advance the agency’s management of advanced medical software. The action plan aims to force manufacturers to be more rigorous in their evaluations, according to the FDA.
Although the nation reached a grim and long-dreaded milestone on Monday, surpassing 500,000 lives lost to COVID—more than were killed in two World Wars and the Vietnam conflict combined—the news this week was mostly good, as key indicators of the pandemic’s severity continued to rapidly improve.
Over the past two weeks, hospitalizations for COVID were down 30 percent, deaths were down 22 percent, and new cases declined by 32 percent—the lowest levels since late October. This week’s numbers declined somewhat more slowly than last week’s, leading Dr. Rachel Walensky, director of the Centers for Disease Control and Prevention, to caution people against letting their guard down just yet: “Things are tenuous. Now is not the time to relax restrictions.” Of particular concern are new variants of the coronavirus that have emerged in numerous states, including one in New York and another in California, that may be more contagious than the original virus.
The best news of the week was surely a report from the Food and Drug Administration (FDA) evaluating the new, single-shot COVID vaccine from Johnson & Johnson (J&J), showing it to be highly effective at preventing severe disease, hospitalization, and death caused by COVID, including variants. On Friday, a panel of outside experts met to assess whether to approve the J&J vaccine for emergency use, which would make it the third in the nation’s arsenal of COVID vaccines. If approved, the vaccine will be rolled out next week, according to the White House, with up to 4M doses available immediately.
The sooner the better: new data show that since vaccinations began in late December, new cases among nursing home residents have fallen more than 80 percent—a hopeful glimpse at the future that lies ahead for the general population once vaccines become widely available.