The latest Altarum Health Sector Economic Indicators show that health spending as a percent of GDP has stabilized near 17.5%, health care price growth and economywide inflation recently converged, and the health sector added over 60,000 jobs in July. See the highlights below.
Health spending as a percent of GDP has stabilized at 17.5%
In June 2023, national health spending grew by 5.0%, year over year, and now represents 17.5% of GDP, equal to the average percent of GDP for the previous 12 months.
Nominal GDP in June 2023 was 5.8% higher than in June 2022, and grew 0.8 percentage points faster than health spending.
Neglecting government subsidies, spending on personal health care in June increased by 8.1%, year over year, and by 7.3% when subsidies are included, exceeding the GDP growth rate for the fifth consecutive month.
Neglecting government subsidies, year-over-year spending on home health care (12.2%) and nursing home care (12.0%) grew fastest in June, while physician and clinical services spending increased the least (6.9%) among major categories.
Personal health care growth (neglecting government subsidies), which continues to be dominated by growth in utilization rather than price increases, has slowed somewhat in the past 4 months.
Health care price growth and economywide inflation finally converge
The overall Health Care Price Index (HCPI) increased by 2.7% year over year in July, slowing 0.1 percentage points from the slightly revised rate in June (2.8%).
For the first time in over two years, health care price growth exceeded overall inflation as economywide price growth (measured by the GDP Deflator) fell to 2.6% in June, its lowest growth rate since March 2021.
In new data for July, overall year-over-year CPI growth actually increased slightly to 3.2%, the first increase in its growth rate since June 2022, driven primarily by changes in commodities price growth.
Among the major health care categories, prices for nursing home care (5.5%) and dental care (5.1%) grew fastest, while physician and clinical services (0.7%) price growth was the slowest in July.
Year-over-year growth in hospital prices paid by private payers fell nearly 2.5 percentage points over the past two months (from 6.1% in May to 3.7% in July), beginning to converge with public payer price growth. In July, growth in Medicare and Medicaid hospital prices reached 2.6% and 2.3% growth respectively.
Our implicit measure of health care utilization growth declined in June, up 4.5% year over year, and down somewhat from slightly revised data (4.9% growth) a month prior.
Health care adds 63,000 jobs in July, the largest increase since July 2022
Health care added 63,000 jobs in July 2023, exceeding the average of 43,700 jobs added per month for the first 6 months of the year and the largest monthly increase in the past year.
July’s health sector job growth was led by growth in ambulatory care settings, which added 35,400 jobs, followed by hospitals, which added 16,100 jobs.
Nursing and residential care facilities added 11,500 jobs in July, with growth occurring in both nursing homes (6,300 jobs) and other nursing and residential care settings (5,200 jobs).
The economy added 187,000 jobs in July, somewhat below the 12-month average of 280,200 jobs. The unemployment rate, at 3.5%, changed little in July.
Health care wage growth in June 2023 was 3.7% year over year, somewhat below the total private sector wage growth of 4.4%.
Wage growth in health care settings is now highest in nursing and residential care, at 4.8% year over year in June 2023. Wage growth in hospitals was 4.3%, while wage growth in ambulatory care settings was 3.0% in June.
The U.S. health system is big and getting bigger. It is labor intense, capital intense, and highly regulated. Each sector operates semi-independently protected by local, state and federal constraints that give incumbents advantages and dissuade insurgents.
Competition has been intramural:
Growth by horizontal consolidation within sectors has been the status quo for most to meet revenue and influence targets. In tandem, diversification aka vertical consolidation and, for some, globalization in each sector has distanced bigger players from smaller:
insurers + medical groups + outpatient facilities + drug benefit managers
retail pharmacies + primary & preventive care + health & wellbeing services + OTC products/devices
regulated medical devices + OTC products for clinics, hospitals, homes, workplaces and schools.
The landscape is no man’s land for the faint of heart but it’s golden for savvy private investors seeking gain at the expense of the system’s dysfunction and addictions—lack of price transparency, lack of interoperability and lack of definitive value propositions.
What’s ahead?
Everyone in the U.S. health system is aware that funding is becoming more scarce and regulatory scrutiny more intense, but few have invested in planning beyond tomorrow and the day after. Unlike drug and device manufacturers with global markets and long-term development cycles, insurers and providers are handicapped. Insurers respond by adjusting coverage, premiums and co-pays annually. Providers—hospitals, physicians, long-term care providers and public health programs– have fewer options. For most, long-range planning is a luxury, and even when attempted, it’s prone to self-protection and lack of objectivity.
Changes to the future state of U.S. healthcare are the result of shifts in these domains:
They apply to every sector in healthcare and define the context for the future of each organization, sector and industry as a whole:
The Clinical Domain: How health, diseases and treatments are defined and managed where and by whom; how caregivers and individuals interact; how clinical data is accessed, structured and translated through AI enabled algorithms; how medication management and OTC are integrated; how social determinants are recognized and addressed by caregivers and communities: and so on. The clinical domain is about more than doctors, nurses, facilities and pills.
The Technology Domain: How information technologies enable customization in diagnostics and treatments; how devices enable self-care; how digital platforms enable access; how systemness facilitates integration of clinical, claims and user experience data; how operating environments shift to automation lower unit costs; how sites of care emerge; how caregivers are trained and much more. Proficiency in the integration of technologies is the distinguishing feature of organizations that survive and those that don’t. It is the glue that facilitates systemness and key to the system’s transformation.
The Regulatory Domain: How affordability, value, competition, choice, healthcare markets, not-for-profit and effectiveness are defined; how local, state and federal laws, administrative orders by government agencies and executive actions define and change compliance risks; how elected officials assess and mitigate perceived deficiencies in a sector’s public accountability or social responsibility; how courts adjudicate challenges to the status quo and barriers to entry by outsiders/under-served populations; how shareholder ownership in healthcare is regulated to balance profit and the public good; et al. Advocacy on behalf of incumbents geared to current regulatory issues (especially in states) is compulsory table stakes requiring more attention; evaluating potential regulatory environment shifts that might fundamentally change the way a system is structured, roles played, funded and overseen is a luxury few enjoy.
The Capital Domain: how needed funding for major government programs (Medicare, Medicaid, Children’s, Military, Veterans, HIS, Dual Eligibles et al) is accessed and structured; how private investment in healthcare is encouraged or dissuaded; how monetary policies impact access to debt; how personal and corporate taxes impact capitalization of U.S. healthcare; how value-based programs reduce unnecessary costs and improve system effectiveness; how the employer tax exemption fares long-term as employee benefits shrink; how U.S. system innovations are monetized in global markets; how insurers structure premiums and out of pocket payments: et al. The capital domain thinks forward to the costs of capital it deploys and anticipated returns. But inputs in the models are wildly variable and inconsistent across sectors: hospitals/health systems vs. global private equity healthcare investors vs. national insurers’ capital strategies vary widely and each is prone to over-simplification about the others.
The Consumer Domain: how individuals, households and populations perceive and use the system; how they assess the value of their healthcare spending; how they vote on healthcare issues; how and where they get information; how they assess alternatives to the status quo; how household circumstances limit access and compromise outcomes; et al. The original sin of the U.S, health system is its presumption that it serves patients who are incapable/unwilling to participate effectively and actively in their care. Might the system’s effectiveness and value proposition be better and spending less if consumerization became core to its future state?
For organizations operating in the U.S. system, staying abreast of trends in these domains is tough. Lag indicators used to monitor trends in each domain are decreasingly predictive of the future. Most Boards stay focused on their own sector/subsector following the lead of their management and thought leadership from their trade associations. Most are unaware of broader trends and activities outside their sector because they’re busy fixing problems that impact their current year performance. Environmental assessments are too narrow and short-sighted. Planning processes are not designed to prompt outside the box thinking or disciplined scenario planning. Too little effort is invested though so much is at risk.
It’s understandable. U.S. healthcare is a victim of its success; maintaining the status quo is easier than forging a new path, however obvious or morally clear. Blaming others and playing the victim card is easier than corrective actions and forward-thinking planning.
In 10 years, the health system will constitute 20% of the entire U.S. economy and play an outsized role in social stability. It’s path to that future and the greater good it pursues needs charting with open minds, facts and creativity. Society deserves no less.
In January 2023, the Rockefeller Institute published a three-part blog series on trends to watch in healthcare in 2023. The series covered broad issues related to the healthcare workforce, economy, and health policy, and highlighted internal industry changes and trends in service delivery, quality, and equity.
Here, we provide a recap and mid-year update on those trends.
The Public Health Emergency:
In January, we anticipated the COVID-19 federal public health emergency (PHE) would end at some point during the year and its ending would impact the industry by rolling back flexibilities and programs that were temporarily put in place to combat the pandemic. The end of the PHE, while not a “trend” per se, held significant potential to alter the trajectory of trends in healthcare coverage, access, and care delivery that were occurring during the pandemic.
Mid-year Update: As predicted, the PHE was not renewed and ended on May 11, 2023. The most notable impact of the non-renewal of the PHE was the end of continuous Medicaid public health insurance coverage. The Kaiser Family Foundation’s Medicaid Enrollment Tracker shows that, as of July 5, 2023, 1,652,000 Medicaid enrollees were disenrolled by the District of Columbia and 28 states reporting data. For context, this means that 39% of people with a completed renewal were disenrolled in reporting states, though disenrollment rates varied significantly across those states from 16 percent in Virginia to 75 percent in South Carolina. The eligibility redetermination process that can lead to a potential disenrollment is being conducted differently in each state with some states moving quickly to make redeterminations and others doing the process more deliberately over the course of the year with a clear intent to avoid shedding people from the Medicaid program because of an inability to submit administrative paperwork.
The process for eligibility renewals will continue to play out over the course of the next year since states have until mid-2024 to update all Medicaid enrollees’ eligibility status. Also notable are some changes made under the purview of the PHE that persist despite the emergency’s conclusion. For example, access to COVID-19 vaccinations and certain COVID-19 treatments generally have not been affected. Some telehealth flexibilities that were allowed under the PHE are also staying in effect, at least until the end of 2024.
Healthcare Workforce Shortages:
Prior to the pandemic, larger demographic trends in society were already impacting the supply of the healthcare workforce. The number of people aging and needing healthcare services was growing while the number of people available to provide care was not keeping pace thus creating a long-term healthcare workforce shortage.
Mid-year Update:The workforce shortage continues. As outlined in a May 23rd Becker’s Hospital Review article, several sources point to a continued shortage. They include a report that says the US could see a deficit of 200,000 to 450,000 registered nurses by 2025. Within the next five years, another report also projects a shortage of more than 3.2 million lower-wage healthcare workers, such as medical assistants, home health aides, and nursing assistants. As a result, some healthcare providers are becoming more creative in their efforts to counteract the workforce shortage: creating alumni networks from which to recruit or providing other benefits to their workforce, such as housing or educational assistance. Policymakers can help counteract the negative impacts of the workforce shortage through a variety of strategies. With the shortage expected to continue, it will be important to enact additional policies that bolster the workforce.
Price Inflation:
As we noted, price inflation was significant in 2022 but was not unique to the health sector.Inflation was particularly exacerbated by the re-opening of the economy after the pandemic, the continued war in Ukraine, and supply chain challenges.
Mid-year Update: Prices for many consumer goods and services increased faster than usual, with overall inflation reaching a four-decade high in mid-2022. The Bureau of Labor Statistics (BLS) reported inflation rates have slowed, with overall prices growing by 6 percent in February 2023 compared to the previous year. Interestingly, prices for medical care increased only 2.3 percent. Similarly, BLS reported that the average price of health care in the United States increased by 0.7 percent in the 12 months ending May 2023, following a previous increase of 1.1 percent. The slower price growth in healthcare compared to other sectors of the economy is highly unusual,[i] and while inflation is not easily influenced by state-level policymakers’ actions alone, the trend is still worth monitoring to better understand the impacts on healthcare access and quality. As of early July, the latest predictions from PwC are that healthcare costs will rise 7% in 2024.
Declining Margins at Hospitals:
Previous analysis by the consulting firm Kaufman Hall predicted that more than half of all hospitals would have negative margins at the end of 2022. As we noted, this was due to such factors as higher-than-normal expenses for staff, supplies, and pharmaceuticals and lower revenues.
Mid-year Update: The latest report from Kaufman Hall offers data that shows a reversal in this trend for the first part of 2023. May was the third consecutive month in which hospital margins were positive after operating in the red for most of 2022. The return to normal is largely driven by revenues that are more in line with pre-pandemic levels. With revenues returning to more normal levels, expenses will be particularly important to watch for the remainder of 2023. If hospital expenses continue to outweigh revenues, policymakers may need to evaluate the financial health of providers and the potential impact that may have on access to services for patients.
Private Equity in Healthcare:
We predicted that private equity (PE) would continue to grow in healthcare, pointing to a PwC consulting report that indicated that PE companies still had plenty of “dry powder,” or money, to invest in 2023.
Mid-year Update:There has been a slowdown in private equity deals over the last year. But it is notable that there were still 200 private equity deals in healthcare in the first quarter of 2023, according to PitchBook’s healthcare services report released in May 2023. While lower than the year before, this is still considered active when compared to pre-pandemic PE dealmaking. Because of the waning of the pandemic and stability returning to the healthcare sector, it is more likely that PE deals stabilize in 2023. And some industry predictions indicate that dealmaking will bounce back further in the second half of 2023. As noted in our previous blog, it will be important to monitor the proliferation of PE in healthcare and determine its impact on healthcare markets, care delivery, innovation, and quality.
Consolidations:
Like many other industries, consolidations of all sorts have been happening in healthcare. The consolidations are both vertical—combining two or more stages of production normally operated by separate companies into one company, such as when hospitals or insurers employ physicians and/or acquire physician practices or other entities like pharmacies—and horizontal—combining organizations that provide the same or similar services, such as hospitals acquiring hospitals.
Mid-year Update: Consolidations of all sorts of healthcare entities continued in 2023 with some of the biggest potential consolidations yet. Those include the proposed merger of two major bi-coastal health system providers: Geisinger, based in Pennsylvania, and Kaiser, based in California. Although the deal must still go through regulatory approval, if completed, the two systems will create a nonprofit that will look to add five or six more systems nationally over the next five years. Other notable consolidations include the finalization of tech-giant Amazon’s purchase of One Medical, a primary care network. And Optum, one of the largest conglomerates that is a subsidiary of United Health Group, increased its net revenue growth by 25% to $54.1 billion in the first quarter of 2023, primarily due to more patients visiting OptumHealth clinics and growth in OptumRx pharmacy scripts processed. Optum’s growth is likely to continue in 2023 as they expect to add another 10,000 physicians. Case in point, in February of this year, Optum paid an undisclosed sum for Crystal Run Healthcare, a network of nearly 400 providers in New York. A goal of consolidation has been better coordination of patient care for improved outcomes and value. Results have been mixed and it is therefore an important trend for policymakers and researchers to monitor and to ensure the impacts are positive.
Alternate Payment Models:
Alternate payment models (APMs) in healthcare have been expanding especially since enactment of the Patient Protection and Affordable Care Act in 2010. They are primarily being developed by the Center for Medicare and Medicaid Innovation (CMMI) which has driven payment policy (including APMs) in the two big government healthcare programs: Medicaid and Medicare. There have been several iterations of APMs—over 50 models—but the one common theme is that all of them generally seek to reward better care.
Mid-year Update: Since the start of 2023, the most notable expansion of the trend toward more alternate payment models was CMMI’s introduction of a new primary care-focused APM called Making Care Primary. In addition to this model, it is expected that the Centers for Medicaid and Medicare Services (CMS), which oversees the operation of these two large public health insurance programs, will introduce more new payment models in 2023, including one that allows states to manage the total cost of care in a given region. This may take various forms, including something akin to Maryland’s global budget, which is used statewide. Since the total cost of care model has yet to be officially revealed, this trend and the emergence of any new developments is worth watching in the second half of 2023. Policymakers can learn from these various payment models and use them to inform the plans implemented in their own state or region in order to improve healthcare.
Attention to Health Equity:
A notable aspect of the pandemic was the disparate impact it had on people of color and other marginalized groups. In response, policymakers and providers began paying more attention to the underlying cause of these disparities. In 2021, President Joe Biden signed an executive order to focus federal resources and attention on reducing health disparities.
Mid-year Update: Increased attention to health equity in healthcare has continued. Ernst and Young, an international consulting group, released its first-ever report on the state of health equity in the United States, which involved a survey of over 500 providers to begin tracking their methods for, and progress in, addressing health disparities. More recently, in June 2023, The Joint Commission on the Accreditation of Healthcare Organizations (JCAHO) announced that it will be adding a certification program for healthcare organizations specifically targeted towards improving health equity. While attention to equity has grown, what will be interesting to watch in the second half of 2023 is the degree to which such efforts are having an impact on actually reducing disparities. Understanding the impacts of various interventions can help policymakers expand efforts that are effective.
Digital TeleHealth Delivery Expansion:
The use of digital health expanded dramatically from 2020 to 2022 as social distancing practices were adopted and telehealth options became more widely available. As noted in our blog series, digital health “includes mobile health (mHealth), health information technology (IT), wearable devices, telehealth and telemedicine, and personalized medicine.” It also includes, “mobile medical apps and software that support the clinical decisions doctors make every day to do artificial intelligence and machine learning.”
Mid-year Update: At the end of 2022 and the start of 2023, the ability to infuse capital to drive the expansion of digital health seemed tenuous, in part due to the collapse of Silicon Valley Bank (SVB). As noted by the publication Pitchbook and CB Insights, venture capital funding in the digital health space totaled $7.5 billion in 2022, a 57 percent year-over-year drop. Although the fast pace of investment in digital health may have slowed since its explosion during the pandemic, the expansion of digital health continues. Our January blog suggested that areas such as behavioral health, care at home, and maternal health were areas to watch. In 2023, digital access is expanding in other areas, such as in-home urgent primary care to allow for the treatment of complex injuries and illnesses with the goal of reducing emergency department visits. And other important digital health deals are still occurring: health tech startup Florence picked up Zipnosis from Bright Health to expand its virtual care capabilities. And with the launch of consumer-facing tech products, such as Chat GPT and Apple Vision Pro in the first half of 2023, additional opportunities for applying such technologies in healthcare may fuel further expansion of digital health. Policies that are developed in the future may want to support the growth of such innovation, while also being mindful to monitor the potential impacts on care.
Expansion of Non-Traditional Providers:
In January, we noted an emergence of companies in healthcare whose genesis was something other than healthcare. The blog pointed to examples of how companies such as Walgreens, CVS, and Amazon were expanding their offerings in healthcare.
Mid-year Update:Non-traditional entities continue to expand in the healthcare space. Notable examples include the recent acquisitions and expansions made by CVS. One of these expansions is being done through its affiliation with the insurance company, Aetna. Through Aetna, CVS has entered the insurance exchange market in four more states in 2023, in addition to the 12 states in which it already operates. CVS also closed a deal in the first half of 2023 to acquire Oak Street Health for over $10 billion. And, in March 2023, CVS announced it had officially acquired Signify Health, a digital telehealth company that enables more care to occur in-home. As noted earlier, Amazon officially completed its deal to acquire OneMedical and United Health Group is working on expanding its use of value-based care through a partnership with Walmart. Monitoring the impact of these emerging companies in healthcare will be important for policymakers that have historically only focused on more traditional providers, such as hospitals. These non-traditional entrants, in many cases, are large organizations with substantial resources and their impact may be just as significant if not greater than traditional providers.
Conclusion
These trends merit close attention in the second half of 2023. As healthcare takes on new shapes, the implications for those in the sector and all who depend on it will be huge. In addition, there are important implications for state and federal policymakers who will need to consider how these trends impact access, affordability, and quality of health care, so they can determine whether and how government might help to accelerate beneficial innovations, invest in promising trends, prevent or reverse harmful trends, and monitor the impacts on consumers.
The latest CPI was a crowd-pleaser: Inflation has plunged from its peak, helping provide relief for consumers.
Beyond the headline, an underlying measure closely watched by economists and the Fed finally began to cool.
Why it matters:
The worst of the inflation crisis looks to be firmly behind us. Price gains appear to be on a path to returning to normal, but there is huge uncertainty around how long that will take, with plenty of hurdles still ahead.
What they’re saying:
“After a punishing stretch of high inflation that eroded consumer’s purchasing power, the fever is breaking,” Bill Adams, chief economist at Comerica Bank, wrote in a note.
While the Fed appears to be on track to tighten by a quarter percentage point two weeks from today, the promising news lowers the odds of further hikes this year.
Details:
Headline CPI rose 3% (or 2.97%, unrounded) in the 12 months through June, the smallest increase since March 2021. That reflects milder price gains for a slew of goods, including food — and outright deflation for other items consumers buy, like airline fares, which fell 8% in June.
The intrigue:
At the same time last year, headline prices skyrocketed by 9%. Now we’re lapping that period, which makes the comparison much more favorable.
Then, commodity prices soared on disruptions from Russia’s invasion of Ukraine. Those prices are sharply lower now, helping the headline figure cool rapidly. Gasoline, for instance, is down nearly 27%.
Those favorable effects will fade in the year-on-year numbers, so don’t be surprised if the headline CPI figure rebounds some in the coming months.
The most encouraging aspect was the core figure, which strips out volatile food and energy costs and is closely followed by policymakers. That rose by just 0.2% in June, the slowest monthly pace since February 2021.
In the past three months, core inflation has risen at a 4.1% annualized pace — down almost a full percentage point from May.
Under the hood, there was notable disinflation across a key sector of the economy monitored by the Fed: core services, excluding shelter. Prices in that category were flat last month, compared to a 0.2% rise in May.
That cooling is happening alongside a still-healthy labor market and solid wage gains (more on this below), which officials worried could stoke inflation in this category.
The Biden administration is eager to tout the progress. “The economy is defying predictions that inflation would not fall absent significant job destruction,” top White House economic adviser Lael Brainard is expected to say this afternoon at the Economic Club of New York, according to prepared remarks.
“Annual inflation has now declined every month for 12 months in a row,” she will say, “and inflation in the United States is now the lowest among G-7 nations … even as our economic recovery from the pandemic has been the strongest.”
The bottom line:
We have been head-faked before by what appeared to be remarkable progress on inflation, notably in the summer of 2001.
With expected cooling in other areas (including shelter, which makes up a big chunk of the index), there is reason to be hopeful this progress could be here to stay.
Last Thursday, the Senate Finance Committee heard testimony from experts who offered damning testimony about hospital consolidation (excerpts below). Committee Chair Ron Wyden (D-OR) gaveled the session to order with this commentary:
“I’d like to talk about health care costs and quality. Advocates for proposed mergers often say they will bring lower health costs due to increased efficiency. Time after time, it’s simply not proven to be the case. When hospitals merge, prices go up, not down. When insurers merge, premiums go up, not down. And quality of care is not any better with this higher cost. “
Ranking Member Mike Crapo (R-ID) offered a more conciliatory assessment in his opening statement: “In exploring and addressing these problems, we have the opportunity to build on our efforts to improve medication access and affordability by taking a broader look at the health care system through a similarly bipartisan, consensus-based lens…We need to examine the drivers of consolidation, as well as its effects on care quality and costs, both for patients and taxpayers. We also need to develop focused, bipartisan and bicameral solutions that reduce out-of-pocket spending while protecting access to lifesaving services.”
Congress’ concern about consolidation in healthcare is broad-based. Pharmacy benefits managers and health insurers face similar scrutiny. Drug price control referenda have passed in several states and a federal cap was included in the Inflation Reduction Act.
The reality is this: the entire U.S. health system is on trial in the court of public opinion for ‘careless disregard for affordability’. And hospitals are seen as part of the problem justifying consolidation as a defense mechanism.
What followed in this 3-hour hearing was testimony from 3 experts critical of hospital consolidation, a Colorado community hospital CEO who opined to competition with big hospital systems and a Peterson Foundation spokesperson who offered that data access and transparency are necessary to mitigate consolidation’s downside impact.
None of their testimony was surprising. Nor were questions from the 25 members of the committee. It’s a narrative that played out in House Energy and Commerce and Ways and Means Committee hearings last month. It’s likely to continue.
Often, Congressional Hearings on healthcare issues amount to little more than political theatre. In this one, four key themes emerged:
Consolidation among hospitals has adversely impacted quality of care and affordability of healthcare. Prices have gone up without commensurate improvements in quality harming consumers.
Larger organizations use horizontal and vertical integration to strengthen their positions relative to smaller competitors. Physician employment by hospitals is concerning. Rural and safety net hospitals are impaired most.
Anti-trust efforts, price transparency mandates, data sharing and value-based programs have not been as effective as anticipated.
Physicians are victims of consolidation and corporatization in U.S. healthcare. They’re paid less because others are paid more.
While committee members varied widely in the intensity of their animosity toward hospitals, a consensus emerged that the hospital status quo is not working for voters and consumers.
My take:
Consolidation is part of everyday life. Last Tuesday’s bombshell announcement of the merger of the PGA Tour and the Saudi Arabia’s Public Investment Fund caught the golfing world by surprise. Anti-trust issues and monopolistic behaviors are noticed by voters and lawmakers. Hospital consolidation is no exception festering suspicions among lawmakers and voters that the public’s good is ill-served. And studies showing that charity care among not-for-profit hospitals is lower than for-profit confuse and complicate.
As I listened to the hearing, I had questions…
Were all relevant perspectives presented?
Was the information provided by witnesses and cited in Committee member questioning accurate?
Will meaningful action result?
But having testified before Congressional Committees, I find myself dismissive of most hearings which seem heavy on political staging but light on meaningful insight. Many are little more than political theatre. Hospital consolidation seems different. There seems to be growing consensus that it’s harmful to some and costly to all.
Sadly, this hearing is the latest evidence that the good will built by hospital heroics in the pandemic is now forgotten. It’s clear hospital consolidation is an issue that faces strong and increased headwinds with evidence mounting—accurate or not– showing more harm than good.
On Monday, Minnetonka, MN-based UHG’s Optum division made a $3.3B all-cash offer to acquire Baton Rouge, LA-based Amedisys, one of the country’s largest home health companies.
Optum’s bid came several weeks after Bannockburn, IL-based Option Care Health, a home health company specialized in drug and infusion services, offered to purchase Amedisys in an all-stock transaction valued at $3.6B. Amedisys itself acquired hospital-at-home company Contessa Health for $250M in 2021. While its Board of Directors is now evaluating whether UHG has made a “Superior Proposal”, a UHG acquisition of Amedisys would likely be subject to significant regulatory oversight, as the payer recently closed on its purchase of home health company and Amedisys-competitor LHC Group in a deal that was heavily scrutinized by the Federal Trade Commission.
The Gist: UHG, the nation’s largest health insurer, is on a tear to bring the country’s largest home health providers under its Optum umbrella—and it has the deep pockets to outbid nearly anyone else trying to do the same.
While some questioned the value of an Option Care-Amedisys combination, UHG would get to plug another asset into its scaled continuum of home-based care, allowing it to steer beneficiaries away from high-cost post acute care and continue to increase profitable intercompany eliminations.
If UHG’s bid for Amedisys is accepted, it would also gain its first hospital-at-home asset in Contessa, providing it with the opportunity to fully redirect—and reduce—its inpatient care spend.
Correction: An earlier version incorrectly referenced a Texas deal between Houston Methodist and Baylor Scott and White. News about deals is sensitive and unnecessarily disruptive to reputable organizations like these. I sourced this news from a reputable deal advisor: it was inaccurate. My apology!
Congressional Republicans and the White House spared Main Street USA the pain of defaulting on the national debt last week. No surprise.
Also not surprising: another not-for-profit-mega deal was announced:
St. Louis, MO-based BJC HealthCare and Kansas City, MO-based Saint Luke’s Health System announced their plan to form a $9.5B revenue, 28-hospital system with facilities in Missouri, Kansas, and Illinois.
This follows recent announcements by four other NFP systems seeking the benefits of larger scale:
Gundersen Health System & Bellin Health (Nov 2022): 11 hospitals, combined ’22 revenue of $2.425B
Froedtert Health & ThedaCare (Apr 2023 LOI): 18 hospitals, combined ’22 revenues of $4.6B
And all these moves are happening in an increasingly dicey environment for large, not-for-profit hospital system operators:
Increased negative media attention to not-for-profit business practices that, to critics, appear inconsistent with a “NFP” organization’s mission and an inadequate trade for tax exemptions each receives.
Decreased demand for inpatient services—the core business for most NFP hospital operations. Though respected sources (Strata, Kaufman Hall, Deloitte, IBIS et al) disagree somewhat on the magnitude and pace of the decline, all forecast decreased demand for traditional hospital inpatient services even after accounting for an increasingly aging population, a declining birthrate, higher acuity in certain inpatient populations (i.e. behavioral health, ortho-neuro et al) and hospital-at-home services.
Increased hostility between national insurers and hospitals over price transparency and operating costs.
Increased employer, regulator and consumer concern about the inadequacy of hospital responsiveness to affordability in healthcare.
And heightened antitrust scrutiny by the FTC which has targeted hospital consolidation as a root cause of higher health costs and fewer choices for consumers. This view is shared by the majorities of both parties in the House of Representatives.
In response, Boards and management in these organizations assert…
Health Insurers—especially investor-owned national plans—enjoy unfettered access to capital to fund opportunistic encroachment into the delivery of care vis a vis employment of physicians, expansion of outpatient services and more.
Private equity funds enjoy unfettered opportunities to invest for short-term profits for their limited partners while planning exits from local communities in 6 years or less.
The payment system for hospitals is fundamentally flawed: it allows for underpayments by Medicaid and Medicare to be offset by secret deals between health insurers and hospitals. It perpetuates firewalls between social services and care delivery systems, physical and behavioral health and others despite evidence of value otherwise. It requires hospitals to be the social safety net in every community regardless of local, state or federal funding to offset these costs.
These reactions are understandable. But self-reflection is also necessary. To those outside the hospital world, lack of hospital price transparency is an excuse. Every hospital bill is a surprise medical bill. Supporting the community safety net is an insignificant but manageable obligation for those with tax exemption status. Advocacy efforts to protect against 340B cuts and site-neutral payment policies are about grabbing/keeping extra revenue for the hospital. What is means to be a “not-for-profit” anything in healthcare is misleading since moneyball is what all seem to play. And short of government-run hospitals, many think price controls might be the answer.
My take:
The headwinds facing large not-for-profit hospitals systems are strong. They cannot be countered by contrarian messaging alone.
What’s next for most is a new wave of operating cost reductions even as pre-pandemic volumes are restored because the future is not a repeat of the past. Being bigger without operating smarter and differently is a recipe for failure.
What’s necessary is a reset for the entire US health system in which not-for-profit systems play a vital role. That discussion should be led by leaders of the largest NFP systems with the full endorsements of their boards and support of large employers, physicians and public health leaders in their communities.
Everything must be on the table: funding, community benefits, tax exemption, executive compensation, governance, administrative costs, affordability, social services, coverage et al. And mechanisms for inaction and delays disallowed.
It’s a unique opportunity for not-for-profit hospitals. It can’t wait.
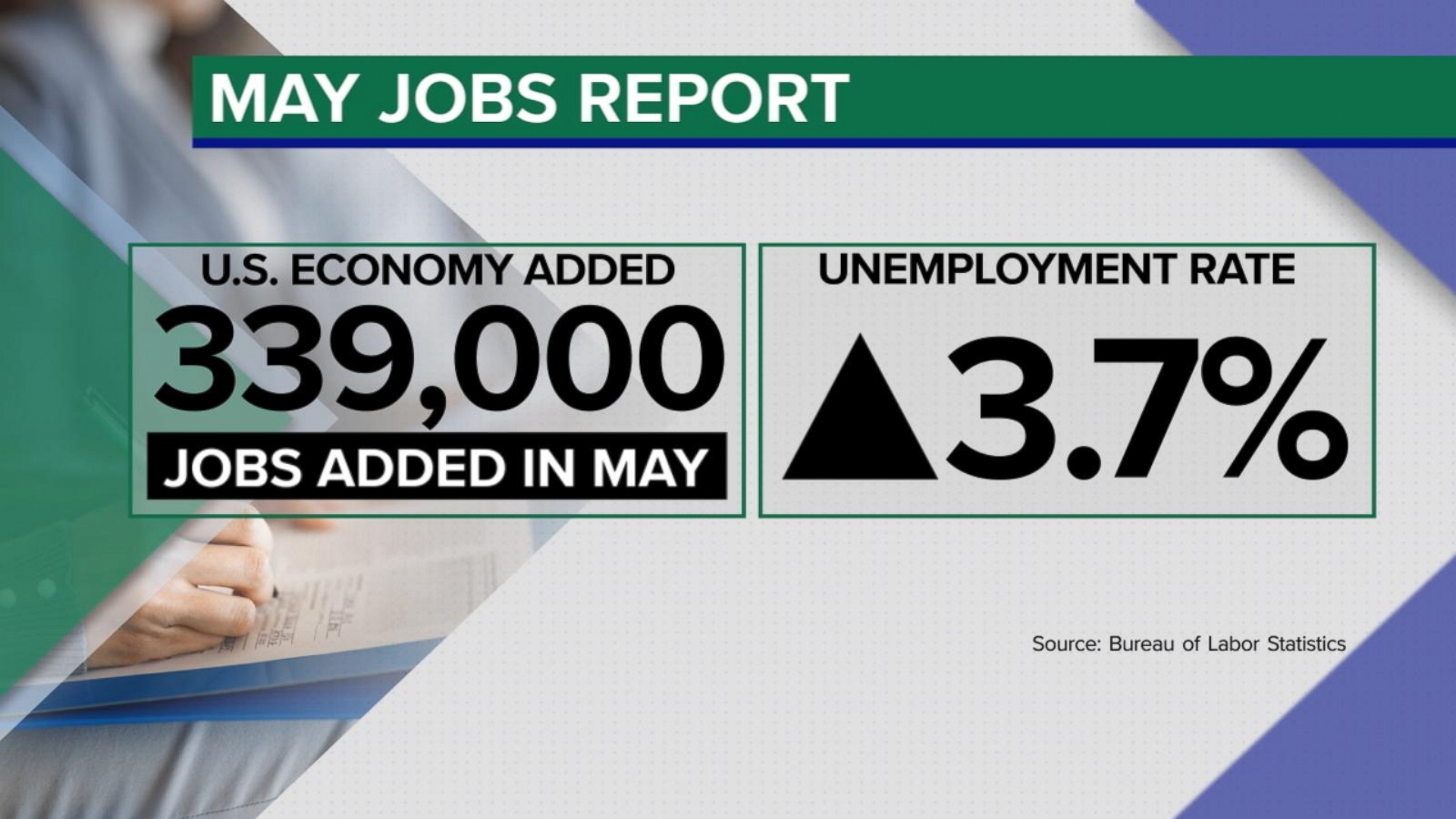
The U.S. economy added 339,000 jobs in May, while the unemployment rate jumped to 3.7% from 3.4%, the Labor Department said Friday.
Why it matters:
Job gains came in well above forecasters’ expectations — the latest sign that the economy is still underpinned by a hot labor market.
Economists expected a gain of 190,000 jobs last month. The May jobs figures are a pickup from the 294,000 added in April, which was revised up by 41,000. Job gains in March were revised up, too.
Details:
Economic policymakers have kept a close eye on other details from the payrolls report — whether more Americans are joining the workforce and how quickly pay is rising.
The labor force participation rate — the share of workers with a job or hunting for one — held at 62.6% in May.
Meanwhile, average hourly earnings, a measure of pay, rose by 0.3% in May. Compared to the same period a year ago, wages are up 4.3%.
What we’re watching:
The May jobs report is among the final data points Federal Reserve officials will consider before deciding whether to continue the interest rate hiking campaign that began more than a year ago.
Inflation remains too high, and there are concerns that rapid price gains are being fueled by the tight labor market and strong consumer demand.
Still, a top Fed official this week signaled the central bank may skip a rate hike at its meeting later this month.
BJC HealthCare of St. Louis and Saint Luke’s Health System of Kansas City are exploring a merger that would yield a 28-hospital, $10 billion, integrated, academic health system, the nonprofits announced Wednesday.
The two have signed a nonbinding letter of intent and “are working toward reaching a definitive agreement in the coming months” with a targeted close before the end of the year, they said. The cross-market deal would be subject to regulatory review and other customary closing conditions.
“Together with Saint Luke’s, we have an exciting opportunity to reinforce our commitment to providing extraordinary care to Missourians and our neighboring communities,” BJC HealthCare President and CEO Richard Liekweg said in the announcement. “Amid the rapidly changing health care landscape, this is the right time to build on our established relationship with Saint Luke’s. With an even stronger financial foundation, we will further invest in our teams, advance the use of technologies and data to support our providers and caregivers and improve the health of our communities.”
Both systems are based in Missouri but “serve distinct geographic markets,” they said.
St. Louis-based BJC Healthcare’s footprint is spread across the greater St. Louis, southern Illinois and southeast Missouri regions. It comprises 14 hospitals including two (Barnes-Jewish and St. Louis Children’s) affiliated with Washington University School of Medicine. It also operates multiple health service organizations providing home health, long-term care, workplace health and other offerings.
Kansas City, Missouri-based Saint Luke’s is a faith-based system with 14 hospitals and more than 100 offices throughout western Missouri and parts of Kansas. It also provides home care and hospice, adult and children’s behavioral care and a senior living community.
Should the deal close, both systems would continue to serve their existing markets and maintain their branding. The joined organization would be run from dual headquarters with BJC’s Liekweg as CEO but an initial board chair hailing from Saint Luke’s.
The organizations said their combination will expand the services available to patients and provide an estimated $1 billion in annual community benefits. The arrangement would also fuel clinical and academic research while supporting greater workforce investment.
“Our integrated health system, with complementary expertise and team of world-class physicians and caregivers, will set a new national standard for medical education and research,” Saint Luke’s President and CEO Melinda Estes, M.D., said in the announcement. “Through our decade-long relationship as a member of the BJC Collaborative, we’ve established mutual trust and respect, so the opportunity to come together as a single integrated system that can accelerate innovation to better serve patients is a logical next step.”
Years of health system consolidation have led to increased scrutiny from regulators and lawmakers, who have worried that mergers can harm competition. To date, however, efforts to block announced deals have been limited to situations where the parties are operating in the same geographic markets.
Larger, cross-market deals like BJC and Saint Luke’s have become more common in the past year, potentially due to the opportunity to distribute operational risks with limited regulatory scrutiny, analysts have noted.
Multiple health policy researchers have warned that these deals are relatively understudied and, according to some prior analyses, very rarely translate to the quality and consumer cost savings often touted by health systems.
Healthcare’s most recent billion-dollar deal took the industry by surprise, leaving medical experts and hospital leaders grappling to comprehend its implications.
In case you missed it, California-based Kaiser Foundation Health Plan and Hospitals, which make up the insurance and facilities half of Kaiser Permanente, announced the acquisition of Geisinger, a Pennsylvania-based health system once acknowledged by President Obama for delivering “high-quality care.”
Upon regulatory approval, Geisinger will become the first organization to join Risant Health, Kaiser Foundation’s newly created $5 billion subsidiary. According to Kaiser, the aim is to build “a portfolio of likeminded, nonprofit, value-oriented, community-based health systems anchored in their respective communities.”
Having spent 18 years as CEO of The Permanente Medical Group, the half of Kaiser Permanente responsible for the delivery of medical care, I took great interest in the announcement. And I wasn’t alone. My phone rang off the hook for weeks with calls from reporters, policy experts and healthcare executives.
After hundreds of conversations, here are the three most common questions I received about the acquisition—and the implications for doctors, insurers, health-system competitors and patients all over the country.
Question 1: Why did Kaiser acquire Geisinger?
Most callers wanted to know about Kaiser’s motivation, figuring there must’ve been more to the acquisition than the press release indicated. Although I don’t have inside information, I believe they were right. Here’s why:
Kaiser Permanente has a long and ongoing reputation for delivering nation-leading care. The organization has consistently earned the highest quality and patient-satisfaction rankings from the National Committee for Quality Assurance (NCQA), Leapfrog Group, JD Power and Medicare.
And yet, despite a 78-year history, dozens of hospitals and 13 million members across eight states, Kaiser Permanente is still considered a coastal—not national—health system. It maintains a huge market share in California and a strong presence in the Mid-Atlantic states, yet the organization has failed repeatedly to replicate that success in other geographies.
With that context, I see two compelling reasons why the Kaiser Foundation Health Plan and Hospitals wish to become a national brand:
Influence. Elected officials and regulatory bodies often turn to healthcare’s biggest players to set legislative agendas and carve out national policy. At that table, there are a limited number of seats. By shedding its reputation as a “local” health system, Kaiser could earn one.
Survival. In recent years, companies like Amazon, CVS and Walmart have been scooping up organizations that provide primary care, telehealth, home health and specialty care services. These “retail giants” are spending up to $13 billion per acquisition. And they’re consuming already-successful healthcare companies like One Medical, Oak Street Health, Signify, Pill Pack and many others. Like an army preparing for war, these corporate behemoths are amassing the components needed to battle the traditional healthcare incumbents and ultimately oust them entirely.
The Geisinger deal expands Kaiser’s footprint, adding 600,000 patients, 10 hospitals and 100 specialty and primary care clinics. These assets lend gravitas, even though Geisinger also comes with a 2022 operating loss of $239 million.
The lesson to draw from this first question is clear: size matters. The days of solo physicians and stand-alone hospitals are over. Nostalgia for medicine’s folksy, home-spun past is understandable but futile. To survive, healthcare players must get bigger quickly or team up with someone who can. That insight leads to the next question and lesson.
Question 2: How much value will Kaiser give Geisinger?
Almost everyone I’ve spoken with understands Kaiser’s desire for greater national influence, but they’re less sure how this deal will affect Geisinger Health.
Geisinger’s Pennsylvania-based hospitals and clinics have been locked in territorial battles for years with surrounding health systems. More recently, the pandemic, combined with staffing shortages and national inflation, have challenged Geisinger’s clinical performance and eroded its bottom line.
Assuming Kaiser plans to invest roughly $1 billion in each of the four to five health systems it’s planning to acquire, that surge in cash inflow will provide Geisinger with temporary financial safety. But the bigger question is how will Kaiser improve Geisinger’s value-proposition enough to grow its market share?
In public comments, Kaiser leaders spoke of the acquisition as an opportunity for Risant to “improve the health of millions of people by increasing access to value-based care and coverage, and raising the bar for value-based approaches that prioritize patient quality outcomes.”
Many of the experts I spoke with understand Kaiser’s value intent. But they question how Kaiser can could deliver on that promise since The Permanente Medical Group (TPMG) wasn’t involved in the deal.
If, hypothetically, Kaiser and Permanente leaders were to strike a deal to collaborate in the future, TPMG’s physician leaders could bring tremendous knowledge, experience and expertise to the table. Otherwise, I agree with those who’ve expressed doubt that Kaiser, alone, will be able to significantly improve Geisinger’s clinical performance.
Health plans and insurance companies play an important role in financing medical care. They possess rich data on performance and can offer incentives that boost access to higher-quality care. But insurers don’t work directly with individual doctors to coordinate medical care or advance clinical solutions on behalf of patients. And without strong physician leadership, the pace of positive change slows to a crawl. As a example, research conducted within The Permanente Medical Group found that it takes only three years to turn a proven clinical advance into standard practice—that’s nearly six times faster than the national average.
For decades, the secret sauce for Kaiser Permanente has been the cohesive success of its three parts: Kaiser Health Plan, Kaiser Foundation Hospitals and The Permanente Medical Group.
And KP’s results speak for themselves:
90% control of hypertension for members (compared to 60% for the rest of the country)
30% fewer deaths from heart attack and stroke (compared to the rest of the country)
20% fewer deaths from colon cancer
The big lesson: insurance, by itself, doesn’t drive major improvements in medicine. It must be a combined effort between forward-looking insurers and innovative, high-performing clinicians.
But there’s another takeaway here for doctors everywhere: now is the time to join forces with other clinicians in your community. Together, you can collaborate to improve clinical quality. You can augment access and make care more affordable for patients. Simultaneously, this is the time for the insurers and the retail giants to figure out which medical groups can deliver the best care and make the best partners. Neither side will flourish alone. And this leads to a third question and lesson.
Question 3: Will the deal work?
Almost all of my conversations ended with this query. I say it’s too early to tell. But as I look years down the road, one part of the deal, in particular, gives me doubt.
Today, Geisinger uses a hybrid reimbursement model—blending both “value-based” care payments with traditional “fee-for-service” insurance plans. In addition to offering its own coverage, it contracts with a variety of other insurance companies. Rarely have I seen this scattered approach succeed.
Most healthcare observers understand the inherent flaw in the “fee for service” (FFS) model is also its greatest appeal to providers: the more you do the more you earn. FFS is how nearly all financial transactions take place in America (i.e., provide a service, earn a fee). In medicine, however, this financial model results in frequent over-testing and over-treatment with minimal if any improvement in clinical outcomes, according to researchers.
The “value-based” alternative to FFS involves prepaying for care—a model often referred to as “capitation.” In short, capitation involves a single fee, paid upfront for all the medical care provided to a defined population of patients for one year based on their age and health status. The better an organization at preventing disease and avoiding complications from chronic illness, the greater its success in both clinical quality and affordability.
Within the small world of capitated healthcare payments, there’s an important element that often gets overlooked. It makes a big difference who receives that lump-sum payment.
In the case of Kaiser Permanente, capitated payments are made directly to the medical group and the physicians who are responsible for providing care. In almost every other health system, an insurance company collects capitated payments but then pays the medical providers on a fee-for-service basis. Even though the arrangement is referred to as capitated, the incentives are overwhelmingly tied to the volume of care (not the value of that care).
In a mixed-payment model, doctors and hospitals invariably prioritize the higher paying FFS patients over the capitated ones. When I think about these conflicting incentives, I’m reminded of a prominent medical group in California. It had a main entrance for its fee-for-service patients and a second, smaller one off to the side for capitated patients.
I doubt the time spent with the patient—or the overall care provided—was equal for both groups. When income is based on quantity of care, not quality, clinicians focus more on treating the complications of chronic disease and medical errors rather than preventing them in the first place. Geisinger has walked this tightrope in the past, but as economic pressures mount, I fear doctors will find the two sets of incentives conflicting and difficult to navigate.
The big lesson: as financial pressures mount, the most effective approaches of the past will likely fail in the future. All healthcare organizations will need to make a decision: keep trying to drive volume and prices up through FFS or shift to capitation. Getting caught in the middle is a prescription for failure.
Examining the healthcare acquisitions made by Amazon and CVS, it’s clear these giants have decided to move aggressively toward a model more like Kaiser Permanente’s—one that brings insurance, pharmacy, physicians and sophisticated IT systems under one roof. These companies, along with Walmart, are aggressively marching down a path toward capitation, focusing on Medicare Advantage (the value-based option for Americans 65+) as an entry point.
So far, Geisinger has hedged its bets by maintaining a hybrid revenue stream. I doubt they can do so successfully in the future. That brings us to a final question.
The biggest question remaining
Over the next decade, hospital systems, insurers and retailers will battle for healthcare supremacy. The most recent Kaiser-Geisinger deal reflects an industry that’s undergoing massive change as health systems face intensifying pressure to remain relevant.
The most important issue to resolve is whether these shifts will ultimately help or harm patients. I’m optimistic for a positive outcome.
Whether or not the retail giants displace the incumbents, they will redefine what it takes to win. For all their faults, companies like Amazon and Walmart care a lot about meeting the needs of customers—a mindset rarely found in today’s healthcare world. As these companies grow ever larger, they’ll place consumer-oriented demands on doctors and hospitals. This will require care providers to deliver higher quality care at more affordable prices.
The retailers will only do deals with the best of the best. And they’ll kick the underachievers to the curb. They’ll use their sophisticated IT systems to better coordinate and innovate medical care. Insurers, hospitals and doctors who fail to keep up will be left behind.
Over time, patients will find themselves with far more choices and control than they have today. And I’m optimistic that will be good for the health of our nation.