HCA is looking for qualified nurses in the event of a job action against its facilities in Los Angeles, such as a strike, according to a job posting from May 29. The giant hospital chain did not respond to multiple requests for comment.
The country’s largest nurses union, National Nurses United, has recently disputed with the system over other pandemic-related labor issues. Nurses at 15 HCA hospitals protested in late May over contractually bargained wage increases the hospital says it can’t deliver due to financial strains, asking nurses to give up the increases or face layoffs.
Another dispute involves a last-minute change mandating in-person voting for nurses deciding whether to form a union at HCA’s Mission Hospital in Asheville, North Carolina, according to an NNU release.
Dive Insight:
Nashville-based HCA Healthcare, the largest among for-profit hospital operators, has received the most among for-profits in Coronavirus Aid, Relief and Economic Security Act funding so far, about $1 billion. The amount is about 2% of HCA’s total 2019 revenue.
The 184-hospital system said it has not had to furlough any employees like other systems have, though some employees have been redeployed or seen their hours and pay decrease. HCA implemented a program providing seven weeks paid time off at 70% of base pay that was scheduled to expire May 16, but extended through June 27.
An NNU spokesperson told Healthcare Dive the program isn’t technically a furlough because some HCA nurses participating said they must remain on call or work rotating shifts.
The union spokesperson also confirmed that an email was sent to HCA nurses referring them to the strike-nurse job posting, which would offer more pay than their current roles.
“This really is a threat to nurses, and particularly insulting when you already have layoffs or cuts, if you don’t accept further concessions,” a union spokesperson told Healthcare Dive.
Nurses in California joined those in five other states at the end of May to protest HCA’s proposal to cut wage increases or impose layoffs.
At HCA’s Regional Medical Center in San Jose, California, NNU filed a suit to block the closure of the maternal-child care center, which it said is in violation of laws to protect the health and safety of the community. The closure proceeded anyway on May 30, followed by an announcement from Santa Clara County that the move may be jeopardizing the facility’s Level II Trauma designation agreement.
Across the country, frontline caregivers continue noting a lack of adequate personal protective equipment. The union’s executive director, Bonnie Castillo, will testify before Congress on Wednesday on protecting nurses during the pandemic and the dire need for optimal PPE.
Pennsylvania’s state health secretary issued an order June 9 requiring all hospitals to better protect staff from COVID-19.
“I have heard from nurses and staff, and this order responds directly to many of their safety concerns,” said Secretary of Health Rachel Levine, MD.
The order requires hospitals to develop, implement and adhere to the following measures by June 15:
Notify staff who have been in close contact with a confirmed or probable COVID-19 case within 24 hours of the known contact; provide instruction for quarantine and work exclusion
Provide testing for symptomatic and asymptomatic hospital staff members who have received notice of a close contact with a confirmed or probable COVID-19 case upon request
Equip staff with nationally approved respirators when staff determine the mask is soiled, damaged or otherwise ineffective
Require universal masking for all individuals entering the hospital facility, except for people for whom wearing a mask would create a further health risk, or individuals under age 2
In addition to medical staff, the measures apply to staff members in therapeutic services, social services, housekeeping services, dietary services and maintenance.
Seven million people have been infected worldwide, and new cases hit a high globally on Sunday, according to the W.H.O. Central banks are seeking new tools to offset the downturn.
RIGHT NOW
New Jersey’s governor said on Tuesday that he was lifting the stay-at-home order that he issued in March. “With more and more of our businesses reopening, we’re no longer requiring you to stay at home,” he said.
The W.H.O. walked back an earlier assertion that asymptomatic transmission is ‘very rare.’
A top expert at the World Health Organization on Tuesday walked back her earlier assertion that transmission of the coronavirus by people who do not have symptoms is “very rare.”
Dr. Maria Van Kerkhove, who made the original comment at a W.H.O. briefing on Monday, said that it was based on just two or three studies and that it was a “misunderstanding” to say asymptomatic transmission is rare globally.
“I was just responding to a question, I wasn’t stating a policy of W.H.O. or anything like that,” she said.
Dr. Van Kerkhove said that the estimates of transmission from people without symptoms come primarily from models, which may not provide an accurate representation. “That’s a big open question, and that remains an open question,” she said.
Scientists had sharply criticized the W.H.O. for creating confusion on the issue, given the far-ranging public policy implications. Governments around the world have recommended face masks and social distancing measures because of the risk of asymptomatic transmission.
A range of scientists said Dr. Van Kerkhove’s comments did not reflect the current scientific research.
“All of the best evidence suggests that people without symptoms can and do readily spread SARS-CoV-2, the virus that causes Covid-19,” scientists at the Harvard Global Health Institute said in a statement on Tuesday.
“Communicating preliminary data about key aspects of the coronavirus without much context can have tremendous negative impact on how the public and policymakers respond to the pandemic.”
A widely cited paper published in April suggested that people are most infectious about two days before the onset of symptoms, and estimated that 44 percent of new infections are a result of transmission from people who were not yet showing symptoms.
Dr. Van Kerkhove and other W.H.O. experts reiterated the importance of physical distancing, personal hygiene, testing, tracing, quarantine and isolation in controlling the pandemic.
The debate over transmission erupted a day after the W.H.O. said that cases had reached a new single-day global high — 136,000 on Sunday, with three-quarters in just 10 countries, mostly in the Americas and South Asia. The coronavirus has already sickened more than seven million people worldwide and killed at least 405,400, according to a New York Times database.
The Pan American Health Organization said on Tuesday that 3.3 million people in South and Central America have been infected with the coronavirus. Dr. Carissa F. Etienne, the agency’s director, said that many areas are experiencing exponential growth in infections and death.
Rajnish Sinha, the owner of an event management company in Delhi, struggled to find a hospital bed for his 75-year-old father-in-law, who tested positive for the virus on Tuesday.
“This is just the beginning of the coming disaster,” Mr. Sinha said. “Only God can save us.”
Dozens of top recipients of government aid have laid off, furloughed or cut the pay of tens of thousands of employees.
HCA Healthcare is one of the world’s wealthiest hospital chains. It earned more than $7 billion in profits over the past two years. It is worth $36 billion. It paid its chief executive $26 million in 2019.
But as the coronavirus swept the country, employees at HCA repeatedly complained that the company was not providing adequate protective gear to nurses, medical technicians and cleaning staff. Last month, HCA executives warned that they would lay off thousands of nurses if they didn’t agree to wage freezes and other concessions.
A few weeks earlier, HCA had received about $1 billion in bailout funds from the federal government, part of an effort to stabilize hospitals during the pandemic.
HCA is among a long list of deep-pocketed health care companies that have received billions of dollars in taxpayer funds but are laying off or cutting the pay of tens of thousands of doctors, nurses and lower-paid workers. Many have continued to pay their top executives millions, although some executives have taken modest pay cuts.
The New York Times analyzed tax and securities filings by 60 of the country’s largest hospital chains, which have received a total of more than $15 billion in emergency funds through the economic stimulus package in the federal CARES Act.
The hospitals — including publicly traded juggernauts like HCA and Tenet Healthcare, elite nonprofits like the Mayo Clinic, and regional chains with thousands of beds and billions in cash — are collectively sitting on tens of billions of dollars of cash reserves that are supposed to help them weather an unanticipated storm. And together, they awarded the five highest-paid officials at each chain about $874 million in the most recent year for which they have disclosed their finances.
At least 36 of those hospital chains have laid off, furloughed or reduced the pay of employees as they try to save money during the pandemic.
Industry officials argue that furloughs and pay reductions allow hospitals to keep providing essential services at a time when the pandemic has gutted their revenue.
But more than a dozen workers at the wealthy hospitals said in interviews that their employers had put the heaviest financial burdens on front-line staff, includinglow-paid cafeteria workers, janitors and nursing assistants. They said pay cuts and furloughs made it even harder for members of the medical staff to do their jobs, forcing them to treat more patients in less time.
Even before the coronavirus swept America, forcing hospitals to stop providing lucrative nonessential surgery and other services, many smaller hospitals were on the financial brink. In March, lawmakers sought to address that with a vast federal economic stimulus package that included $175 billion for the Department of Health and Human Services to hand out in grants to hospitals.
But the formulas to determine how much money hospitals receive were based largely on their revenue, not their financial needs. As a result, hospitals serving wealthier patients have received far more funding than those that treat low-income patients, according to a study by the Kaiser Family Foundation.
One of the bailout’s goals was to avoid job losses in health care, said Zack Cooper, an associate professor of health policy and economics at Yale University who is a critic of the formulas used to determine the payouts. “However, when you see hospitals laying off or furloughing staff, it’s pretty good evidence the way they designed the policy is not optimal,” he added.
The Mayo Clinic, with more than eight months of cash in reserve, received about $170 million in bailout funds, according to data compiled by Good Jobs First, which researches government subsidies of companies. The Mayo Clinic is furloughing or reducing the working hours of about 23,000 employees, according to a spokeswoman, who was among those who went on furlough. A second spokeswoman said that Mayo Clinic executives have had their pay cut.
Seven chains that together received more than $1.5 billion in bailout funds — Trinity Health, Beaumont Health and the Henry Ford Health System in Michigan; SSM Health and Mercy in St. Louis; Fairview Health in Minneapolis; and Prisma Health in South Carolina — have furloughed or laid off more than 30,000 workers, according to company officials and local news reports.
The bailout money, which hospitals received from the Health and Human Services Department without having to apply for it, came with few strings attached.
Katherine McKeogh, a department spokeswoman, said it “encourages providers to use these funds to maintain delivery capacity by paying and protecting doctors, nurses and other health care workers.” The legislation restricts hospitals’ ability to use the bailout funds to pay top executives, although it doesn’t stop recipients from continuing to award large bonuses.
The hospitals generally declined to comment on how much they are paying their top executives this year, although they have reported previous years’ compensation in public filings. But some hospitals furloughing front-line staff or cutting their salaries have trumpeted their top executives’ decisions to take voluntary pay cuts or to contribute portions of their salary to help their employees.
The for-profit hospital giant Tenet Healthcare, which has received $345 million in taxpayer assistance since April, has furloughed roughly 11,000 workers, citing the financial pressures from the pandemic. The company’s chief executive, Ron Rittenmeyer, told analysts in May that he would donate half of his salary for six months to a fund set up to assist those furloughed workers.
But Mr. Rittenmeyer’s salary last year was a small fraction of his $24 million pay package, which consists largely of stock options and bonuses, securities filings show. In total, he will wind up donating roughly $375,000 to the fund — equivalent to about 1.5 percent of his total pay last year.
A Tenet spokeswoman declined to comment on the precise figures.
The chief executive at HCA, Samuel Hazen, has donated two months of his salary to a fund to help HCA’s workers. Based on his pay last year, that donation would amount to about $237,000 — or less than 1 percent — of his $26 million compensation.
“The leadership cadre of these organizations are going to need to make sacrifices that are commensurate with the sacrifices of their work force, not token sacrifices,” said Jeff Goldsmith, the president of Health Futures, an industry consulting firm.
Many large nonprofit hospital chains also pay their senior executives well into the millions of dollars a year.
Dr. Rod Hochman, the chief executive of the Providence Health System, for instance, was paid more than $10 million in 2018, the most recent year for which records are available. Providence received at least $509 million in federal bailout funds.
A spokeswoman, Melissa Tizon, said Dr. Hochman would take a voluntary pay cut of 50 percent for the rest of 2020. But that applies only to his base salary, which in 2018 was less than 20 percent of his total compensation.
Some of Providence’s physicians and nurses have been told to prepare for pay cuts of at least 10 percent beginning in July. That includes employees treating coronavirus patients.
Stanford University’s health system collected more than $100 million in federal bailout grants, adding to its pile of $2.4 billion of cash that it can use for any purpose.
Stanford is temporarily cutting the hours of nursing staff, nursing assistants, janitorial workers and others at its two hospitals. Julie Greicius, a spokeswoman for Stanford, said the reduction in hours was intended “to keep everyone employed and our staff at full wages with benefits intact.”
Ms. Greicius said David Entwistle, the chief executive of Stanford’s health system, had the choice of reducing his pay by 20 percent or taking time off, and chose to reduce his working hours but “is maintaining his earning level by using paid time off.” In 2018, the latest year for which Stanford has disclosed his compensation, Mr. Entwistle earned about $2.8 million. Ms. Greicius said the majority of employees made the same choice as Mr. Entwistle.
HCA’s $1 billion in federal grants appears to make it the largest beneficiary of health care bailout funds. But its medical workers have a long list of complaints about what they see as penny-pinching practices.
Since the pandemic began, medical workers at 19 HCA hospitals have filed complaints with the Occupational Safety and Health Administration about the lack of respirator masks and being forced to reuse medical gowns, according to copies of the complaints reviewed by The Times.
Ed Fishbough, an HCA spokesman, said that despite a global shortage of masks and other protective gear, the company had “provided appropriate P.P.E., including a universal masking policy implemented in March requiring all staff in all areas to wear masks, including N95s, in line with C.D.C. guidance.”
Celia Yap-Banago, a nurse at an HCA hospital in Kansas City, Mo., died from the virus in April, a month after her colleagues complained to OSHA that she had to treat a patient without wearing protective gear. The next month, Rosa Luna, who cleaned patient rooms at HCA’s hospital in Riverside, Calif., also died of the virus; her colleagues had warned executives in emails that workers, especially those cleaning hospital rooms, weren’t provided proper masks.
Around the time of Ms. Luna’s death, HCA executives delivered a warning to officials at the Service Employees International Union and National Nurses United, which represent many HCA employees. The company would lay off up to 10 percent of their members, unless the unionized workers amended their contracts to incorporate wage freezes and the elimination of company contributions to workers’ retirement plans, among other concessions.
Nurses responded by staging protests in front of more than a dozen HCA hospitals.
“We don’t work in a jelly bean factory, where it’s OK if we make a blue jelly bean instead of a red one,” said Kathy Montanino, a nurse treating Covid-19 patients at HCA’s Riverside hospital. “We are dealing with people’s lives, and this company puts their profits over patients and their staff.”
Mr. Fishbough, the spokesman, said HCA “has not laid off or furloughed a single caregiver due to the pandemic.” He said the company had been paying medical workers 70 percent of their base pay, even if they were not working. Mr. Fishbough said that executives had taken pay cuts, but that the unions had refused to take similar steps.
“While we hope to continue to avoid layoffs, the unions’ decisions have made that more difficultfor our facilities that are unionized,” he said. The dispute continues.
Apparently anticipating a strike, a unit of HCA recently created “a new line of business focused on staffing strike-related labor shortages,” according to an email that an HCA recruiter sent to nurses.
The email, reviewed by The Times, said nurses who joined the venture would earn more than they did in their current jobs: up to $980 per shift, plus a $150 “Show Up” bonus and a continental breakfast.
Banner Health warned of a major spike of COVID-19 cases over the past few weeks in Arizona as the state opened back up and eased social distancing guidelines.
Arizona’s COVID-19 hospitalizations are rapidly increasing and raising potential capacity concerns, the system said.
“As of June 4, there were 1,234 hospitalized COVID-19 patients,” the system said in a statement. “About 50% of those patients are hospitalized in Banner Health facilities.”
Banner officials said its ICUs have gotten very busy, and the system has been transferring patients and resources to avoid putting stress on one particular hospital. Banner Health operates 28 hospitals across six states, including several hospitals in Arizona. The health system’s update comes as other hospital systems are eyeing a potential resurgence of COVID-19 cases as states reopen their economies after months of stay-at-home orders.
“If these trends continue, Banner will soon need to exercise surge planning and flex up to 125% bed capacity,” the system warned.
The number of Banner Health patients in Arizona on a ventilator has also increased over the past few weeks, from 41 on May 22 to nearly 120 on June 3.
The system also attributed the increase in COVID-19 cases to a relaxation of the state’s stay-at-home order, which expired May 15.
The cases started to spike two weeks after the end of the order, which is the likely incubation period for the virus.
Banner emphasized that the public needs to continue certain behaviors like wearing a mask in public and social distancing in order to ensure capacity isn’t overwhelmed.
Hospitals not only have to worry about the prospects of a second surge of the virus in the fall but also a wave of pent-up demand for healthcare services put off due to the pandemic.
Banner Health, like all health systems, canceled or postponed elective procedures at the onset of the pandemic back in March. But health systems are taking small steps to resume elective procedures.
Banner Health has also taken steps to preserve its personal protective equipment (PPE), which has been in short supply across the healthcare industry throughout the pandemic. Banner was one of 15 healthcare systems to buy a minority stake in PPE domestic manufacturer Prestige Ameritech in the hopes of shoring up a supply chain that is traditionally reliant on overseas manufacturers.
Shutdown orders prevented about 60 million novel coronavirus infections in the United States and 285 million in China, according to a research study published Monday that examined how stay-at-home orders and other restrictions limited the spread of the contagion.
A separate study from epidemiologists at Imperial College London estimated the shutdowns saved about 3.1 million lives in 11 European countries, including 500,000 in the United Kingdom, and dropped infection rates by an average of 82 percent, sufficient to drive the contagion well below epidemic levels.
The two reports, published simultaneously Monday in the journal Nature, used completely different methods to reach similar conclusions. They suggest that the aggressive and unprecedented shutdowns, which caused massive economic disruptions and job losses, were effective at halting the exponential spread of the novel coronavirus.
“Without these policies employed, we would have lived through a very different April and May,” said Solomon Hsiang, director of the Global Policy Laboratory at the University of California at Berkeley, and the leader of the research team that surveyed how six countries — China, the United States, France, Italy, Iran and South Korea — responded to the pandemic.
He called the global response to covid-19, the disease caused by the virus, “an extraordinary moment in human history when the world had to come together,” and said the shutdowns and other mitigation measures resulted in “saving more lives in a shorter period of time than ever before.”
The two reports on the effectiveness of the shutdowns come with a clear warning that the pandemic, even if in retreat in some of the places hardest hit, is far from over. The overwhelming majority of people remain susceptible to the virus. Only about 3 percent to 4 percent of people in the countries being studied have been infected to date, said Samir Bhatt, senior author of the Imperial College London study.
“This is just the beginning of the epidemic: we’re very far from herd immunity,” Bhatt said Monday in an email. “The risk of a second wave happening if all interventions and precautions are abandoned is very real.”
In a teleconference with reporters later, Bhatt said economic activity could return to some degree so long as some interventions to limit viral spread remain in place: “We’re not saying the country needs to stay locked down forever.”
The Berkeley study used an “econometric” model to estimate how 1,717 interventions, such as stay-at-home orders, business closings and travel bans, altered the spread of the virus. The researchers looked at infection rates before and after the interventions were imposed. Some of these interventions were local, and some regional or national. The researchers concluded that the six countries collectively managed to avert 62 million test-confirmed infections.
Because most people who are infected never get tested, the actual number of infections that were averted is much higher — about 530 million in the six countries, the Berkeley researchers estimated.
Timing is crucial, the Berkeley study found. Small delays in implementing shutdowns can lead to “dramatically different health outcomes.” The report, while reviewing what worked and what made little difference, is clearly aimed at the many countries still early in their battle against the coronavirus.
“Societies around the world are weighing whether the health benefits of anti-contagion policies are worth their social and economic costs,” the Berkeley team wrote. The economic costs of shutdowns are highly visible — closed stores, huge job losses, empty streets, food lines. The health benefits of the shutdowns, however, are invisible, because they involve “infections that never occurred and deaths that did not happen,” Hsiang said.
That spurred the researchers to come up with their estimates of infections prevented. The Berkeley team did not produce an estimate of lives saved.
One striking finding: School closures did not show a significant effect, although the authors cautioned that their research on this was not conclusive and the effectiveness of school closures requires further study. Banning large gatherings had more of an effect in Iran and Italy than in the other countries.
In discussing their findings Monday with reporters in the teleconference, leaders of the two research teams said challenges exist in crafting their models and thus there are uncertainties in the final estimates.
Bhatt, for example, said the model used by his team is highly sensitive to assumptions about the infection fatality rate, estimates for which have varied among researchers and from one country to another. He said his team was heartened to see that its estimates for the number of people infected so far is generally consistent with antibody surveys that attempt to calculate the attack rate of the virus.
Ian Bolliger, one of the Berkeley researchers, acknowledged the difficulty in obtaining reliable numbers for coronavirus infections given the haphazard pattern of testing for the virus. Both research teams said the peer review process had made their findings more robust.
After months of lock down, hospitals are eager to get patients back for routine care and elective procedures.
An executive at a Palm Beach hospital stands between a box of surgical masks and a Purell dispenser.
“We understand you haven’t been inside our hospitals for some time,” she says to the camera. The executive is delivering her line for a promotional video intended to get people back to hospitals after almost three months of avoiding the place at all costs.
Moments later, the film crew records her chatting with a vascular surgeon in an idled operating room, who soothingly reassures that a hospital is the cleanest place to be outside your home. “The hospital is safer than the grocery store,” the doctor says.
The video published on YouTube in mid-May is part of a marketing campaign by Tenet Healthcare, which operates 65 hospitals and about 250 ambulatory surgery centers. It’s one attempt to solve a problem the entire health-care industry faces: Most patients vanished when Covid-19 swept the country.
Billions in Losses
Much of routine health care came to a halt in March as hospitals cleared space for an expected wave of Covid-19 patients and authorities ordered a halt to surgeries and other procedures that could be postponed. The decline in volume has clobbered hospital finances, with the industry estimating it is losing $50 billion a month.
Emergency visits dropped by 42% in four weeks in April compared to the same period last year, the Centers for Disease Control reported June 3. The number of U.S. patients getting hospital care dropped by more than half in late March and early April compared to 2019, according to data from Strata Decision Technology, which provides software to hospitals.
Some of that rebounded modestly in May as distancing rules eased, but hospital volume is nowhere near pre-Covid levels. With the pandemic ongoing and many states still confirming hundreds of new cases daily, patients are hesitating to rush back to hospitals.
“The main thing that really is a gating factor at this point is patient comfort,” Tenet President and Chief Operating Officer Saumya Sutaria said at a recent virtual conference with investors. Tenet declined interview requests.
Free Masks
To counter the public’s fears, hospitals publicize what they’re doing to keep patients safe. They’re handing out masks at the door and spacing out chairs in waiting rooms. They’re steering Covid-19 patients to dedicated sites and testing staff regularly.
Hospitals need to show patients that their facilities are safe. At Catholic hospital chain Trinity Health, that includes moving patients through “Covid-free” zones with separate doors, elevators and waiting areas.
“We can put all of the outreach and marketing in place, but it’s only as effective as the people who execute those strategies,” said Julie Spencer Washington, Trinity’s chief marketing and communications officer.
The question for the entire industry is how quickly patients come back. The answer will depend on a constellation of related variables, including how reluctant people are to resume care, and the course of the pandemic. Future surges could force hospitals to shut down regular care again — and spook patients further.
Hospitals and doctors are going to have to do as much as they can as fast as they can until they can’t anymore,” said Lisa Bielamowicz, co-founder of consultancy Gist Healthcare.
Many patients, on the other hand, are in no rush. “They’re waiting and watching rather than pulling the trigger and going to see the doctor like they would have in the past,” Bielamowicz said.
The calculation for the health-care industry is different than for many other service businesses resuming operations. A hospital procedure or even a check-up is more intimate than a meal out.
For procedures that require in-patient rehab stints for recovery, the havoc Covid-19 has brought to nursing homes adds another layer of concern. “Those places seem like deathtraps now, so it’s much harder to bring back those patients because you need to find an alternative way for them to rehab,” Bielamowicz said.
And the biggest consumers of health care are the elderly and the chronically ill, the very people Covid-19 most threatens. “From personal discussions with my patients, the older and more co-morbidities that any individual has, the more nervous they are about returning,” said Shauna Gulley, chief clinical officer at Centura Health, which has hospitals in Colorado and Kansas.
Patients with serious ongoing needs like cancer treatment or emergencies like heart attacks and strokes have continued to get care. And many medical problems resolve on their own. The decline in those visits – for a migraine headache, for example – reduces providers’ revenue but may not harm patients in the long-term.
While people often go to the emergency room for needs better treated in other settings, now the concern is the opposite: That true medical emergencies will be neglected.
Ascension, the nation’s largest Catholic hospital chain, has purchased billboards that say “Don’t delay ER care.” On hospital websites and social media posts, Tenet facilities reminded patients that “Emergencies Can’t wait. We’re Open & Safe.”
Deferred Care
Doctors fear that some patients will defer needed care too long, allowing progressive conditions to deteriorate. Clinicians at Maimonides Medical Center in Brooklyn, New York, have seen patients arrive sicker because they didn’t come earlier, said Ken Gibbs, the hospital’s CEO.
“There are unmet needs, I think that’s clear,” he said. “And I think the data on that will emerge, but it will take time.”
Maimonides treated 471 Covid patients at the peak on April 9, Gibbs said, and still had about 100 in late May. The hospital has applied for a waiver from New York State to resume elective surgeries, which are still on hold in New York City.
Some hospitals are preparing for a lasting dent in their revenue. For years, health economists have pointed to waste in the health-care system, with the estimated cost of unnecessary treatments in the hundreds of billions of dollars. Covid-19 may demonstrate that patients are willing to forego some of that care or opt for more conservative treatment.
People who had delayed back surgeries, for example, may now decide that doing physical therapy at home is good enough, said Marvin O’Quinn, president and chief operating officer at CommonSpirit Health, a large Catholic hospital system.
“We’ve all talked about too much intervention in health care in the past,” he said. “I think we’ll see a new normal in terms of what patients want to do and what doctors want to do, and we will have to adjust to that.”
Factors such as how many patients would need ICU treatment, average length of stay and fatality risk are straining hospital resources.
When it became evident that the COVID-19 pandemic would spread across the U.S., lawmakers, scientists and healthcare leaders sought to predict what the financial and operational impact on hospitals would be. In those early days, policymakers relied on data from China, where the pandemic originated.
Now, with the benefit of time, the early predictions seriously underestimated the coronavirus’ impacts. University of California Berkeley and Kaiser Permanente researchers have determined that certain factors — such as how many patients would need treatment in intensive care units, average length of stay and fatality risk — are much worse than previously anticipated, and put a much greater strain on hospital resources.
WHAT’S THE IMPACT
Looking primarily at California and Washington, data showed the incidents of COVID-19-related hospital ICU admissions totaled between 15.6 and 23.3 patients per 100,000 in northern and southern California, respectively, and 14.7 per 100,000 in Washington. This incidence increased with age, hitting 74 per 100,000 people in northern California, 90.4 per 100,000 in southern California, and 46.7 per 100,000 in Washington for those ages 80 and older. These numbers peaked in late March and early April.
Those numbers are greater than the initial forecast, especially when factoring in the virus itself. Modeling estimates based on Chinese data suggested that about 30% of coronavirus patients would require ICU care, but in the U.S., the probability of ICU admissions was 40.7%. Male patients are more likely to be admitted to the ICU than females, and also are more likely to die.
Length of stay was also higher than had been predicted. By April 9, the median length of stay was 9.3 days for survivors and 12.7 days for non-survivors. Among patients receiving intensive care, the median stay was 10.5 days, although some patients stayed in the ICU for roughly a month.
Long durations of hospital stay, in particular among non-survivors, indicates the potential for substantial healthcare burden associated with the management of patients with severe COVID-19 — including the need for ventilators, personal protective equipment including N95 masks, more ICU beds and the cancellation of elective surgeries.
The considerable length of stay among COVID patients suggests that unmitigated transmission of the virus could threaten hospital capacity as it has in hotspots such as New York and Italy. Social distancing measures have acted as a stop-gap in reducing transmission and protecting health systems, but the authors said hospitals would do well to ensure capacity in the coming months in a manner that’s responsive to changes in social distancing measures.
THE LARGER TREND
These challenges have placed a financial burden on hospitals that can’t be overstated. In fact, a Kaufman Hall report looking at April hospital financial performance showed that steep volume and revenue declines drove margin performance so low that it broke records.
Despite $50 billion in funding allocated through the CARES Act, operating EBITDA margins fell to -19%. They fell 174%, or 2,791 basis points, compared to the same period last year, and 118% compared to March. This shows a steady and dramatic decline, as EBITDA margins were as high as 6.5% in April.
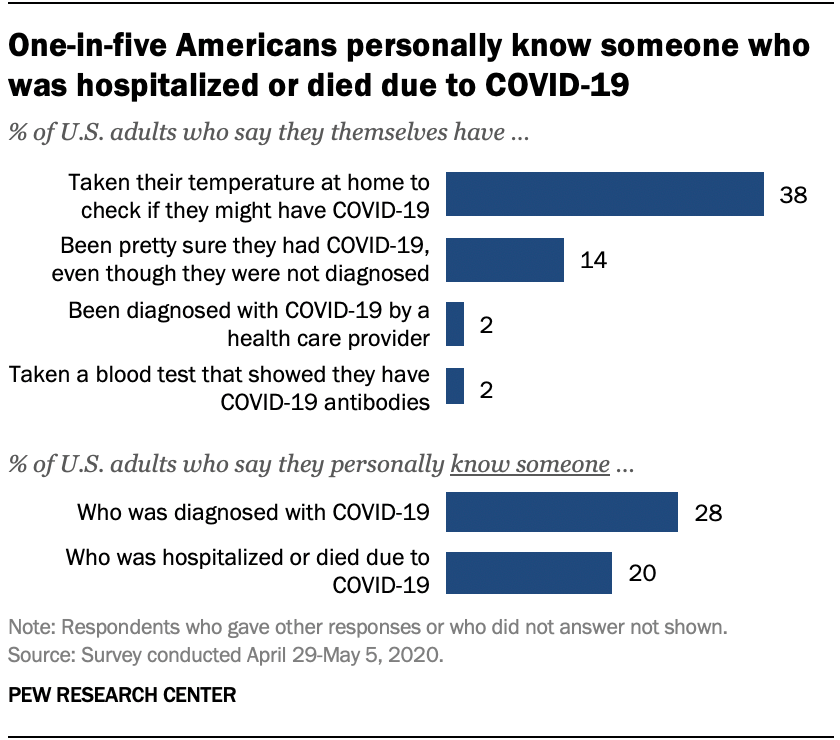
Relatively few Americans say they have been diagnosed with COVID-19 or tested positive for coronavirus antibodies, but many more believe they may have been infected or say they personally know someone who has been diagnosed.
Only 2% of U.S. adults say they have been officially diagnosed with COVID-19 by a health care provider, according to a new Pew Research Center survey. And 2% say they have taken a blood test that showed they have COVID-19 antibodies, an indication that they previously had the coronavirus. But many more Americans (14%) say they are “pretty sure” they had COVID-19, despite not getting an official diagnosis. And nearly four-in-ten (38%) say they’ve taken their temperature to check if they might have the disease.
Although few Americans have been diagnosed with COVID-19 themselves, many more say they know someone with a positive diagnosis. More than one-in-four U.S. adults (28%) say they personally know someone who has been diagnosed by a health care provider as having COVID-19. A smaller share of Americans (20%) say they know someone who has been hospitalized or who has died as a result of having the coronavirus.
Some groups are more likely than others to report personal experiences with COVID-19. For instance, black adults are the most likely to personally know someone who has been hospitalized or died as a result of the disease. One-third of black Americans (34%) know someone who has been hospitalized or died, compared with 19% of Hispanics and 18% of white adults. Black Americans (32%) are also slightly more likely than Hispanic adults (26%) to know someone diagnosed with COVID-19. Public health studies have found black Americans are disproportionately dying or requiring hospitalization as a result of the coronavirus.
Areas in the northeastern United States have recorded some of the highest rates of coronavirus cases and fatalities, and this is reflected in the Center’s survey. About four-in-ten adults living in the Northeast (42%) say they personally know someone diagnosed with COVID-19, significantly more than among adults living in any other region. People living in the Northeast (31%) are also the most likely to know someone who has been hospitalized or died as a result of the disease.
One aspect of personal risk for exposure to the coronavirus is whether someone is employed in a setting where they must have frequent contact with other people, such as at a grocery store, hospital or construction site. Given the potential for the spread of the coronavirus within households, risk to individuals is also higher if other members of the household are employed in similar settings. Among people who are currently employed full-time, 35% are working in a job with frequent public contact. Among those working part-time, almost half work (48%) in such a setting. For those living in a household with other adults, 35% report that at least one of those individuals is working in a job that requires frequent contact with other people.
Taken together, nearly four-in-ten Americans (38%) have this type of exposure – either currently working in a job that requires contact with others, living in a household with others whose jobs require contact, or both.
Hispanics (at 48%) are more likely than either blacks (38%) or whites (35%) to have this type of personal or household exposure. An earlier Center analysis of government data found Hispanic adults were slightly more likely to work in service-sector jobs that require customer interaction, and that are at higher risk of layoffs as a result of the virus. In fact, the current Center survey found Hispanics were among the most likely to have experienced pay cuts or job losses due to the coronavirus outbreak.
Interpersonal exposure in the workplace is also more widespread among younger adults. And there is a 10 percentage point difference between upper- and lower-income Americans in exposure, with lower-income adults more likely to work in situations where they have to interact with the public, or to live with people who do.
Health experts warn that COVID-19 is particularly dangerous to people who have underlying medical conditions. In the survey, one-third of adults say they have such a condition. Among this group, nearly six-in-ten (58%) say that the coronavirus outbreak is a major threat to their personal health. Among those who do not report having an underlying medical condition, just 28% see the outbreak as a major threat to their health. Americans who have an underlying health condition are also more likely than those who do not to say they’ve taken their temperature to check if they might have COVID-19 (47% vs. 33% of those without a health condition).
Self-reports of an underlying health condition vary greatly by age. Among those ages 18 to 29, just 16% say they have a condition; this rises steadily with age to 56% among those 65 and older. Whites are a little more likely than blacks and Hispanics to report having a health condition, but both blacks (at 54%) and Hispanics (52%) are far more likely than whites (32%) to say that the coronavirus outbreak is “a major threat” to their health.
Months into the pandemic, the U.S. faces an ongoing shortage of PPE and some of it is still subject to tariffs.
Gojo Industries, which makes Purell, builds automated hand sanitizer dispensers in the U.S. The devices rely on an electronic input made in China. But in early March, the U.S. Trade Representative (USTR) turned down Gojo’s tariff exemption request for the specific part needed for its dispensers, just before President Donald Trump declared a national emergency due to COVID-19.
The government later reversed its decision and waived the tariff after a senator from Ohio, where Gojo Industries is based, pressured the USTR because of the product’s importance to public health.
But several months into the COVID-19 pandemic, many consumers still struggle to find public-health-related products, from hand sanitizer to wipes. There’s also a shortage of personal protective equiptment (PPE) in the United States, and some of it is still subject to tariffs, throwing a wrench into pandemic preparedness and response.
Health supply chain experts sound the warning bell
The healthcare industry warned the Trump administration long before COVID-19 that imposing tariffs on Chinese-produced essential healthcare products put the nation’s public health preparedness at risk.
In August 2018, Matt Rowan, president of the Health Industry Distributors Association (HIDA) told the U.S. Trade Representative (USTR) 301 Committee that products on the proposed list were widely used in healthcare settings and “are a critical component of our nation’s response to public health emergencies, such as Ebola.”
Tariffs on items like masks, medical gloves, isolation gowns and wet wipes would not only increase U.S. healthcare costs, but impact government and commercial suppliers supporting patients and providers during a medical crisis, the industry warned.
“We did not make up for the lack of imports from China by more imports from the rest of the world.”
Jennifer Hillman
Senior fellow for trade and international political economy, Council on Foreign Relations
Disrupting this supply chain would erode the industry’s ability to deliver quality outcomes, and “placing tariffs on these products would lead to product shortages and further exacerbate public health challenges during times of crisis. It would significantly limit the ability of all levels of government, as well as the commercial healthcare supply chain, to adequately support response efforts during emergency events,” Rowan said.
In spite of healthcare industry testimony, the U.S. slapped 15% to 25% tariffs on many of these essential healthcare items. That included 25% Section 301 tariffs on items like disposable medical headwear, hand sanitizers and pulse oximeters. It included 15% Section 301 tariffs on medical protective clothing, protective goggles, and Nitrile and sterile gloves.
In 2018, the American Action Forum estimated if import numbers remained consistent, medical supply costs would rise by $400 million.
“A good portion of the reason why we are in such a difficult position is imports of those products went way down once those tariffs were imposed on China,” Jennifer Hillman, senior fellow for trade and international political economy at the Council on Foreign Relations, told reporters on a press call. “Our traditional stockpiles, the amount that we had just in storage, by FEMA, by Veterans Affairs, by HHS, and by a lot of state and local hospitals, they decreased the amount of their imports and decreased their stockpiles because of the tariffs.”
Shefali Kapadia / Supply Chain Dive, data from World Trade Organization
In placing the tariffs, one Trump administration goal was for buyers to procure items from other countries or manufacture in the U.S. instead. And that happened, but not to the extent necessary to maintain the stockpiles.
“We did not make up for the lack of imports from China by more imports from the rest of the world,” Hillman said. China was the largest exporter of medical face masks globally, accounting for 25% of the world’s supply in 2019, according to the World Trade Organization (WTO).
The U.S. was the largest medical products importer during the last three years, with 19% of total world imports of these products in 2019, according to the WTO. Personal protective products (including face masks, hand sanitizer and protective eyewear) made up 10% of U.S. medical imports. Worldwide trade of products labeled “critical” and in severe shortage during the pandemic, included 1.7% of the total world trade for 2019, totaling $597 billion. The U.S. imported $5.2 billion in medical equipment in 2019.
The time-consuming exemption process
Trump refused a blanket exemption for medical products when COVID-19 hit, but did grant some exemptions retroactively to Sept. 1, 2019, through Sept. 1, 2020, on supplies like sterile drapes, disposable gowns, some face masks and disposable shoe covers. The government granted exemptions in executive orders on March 10, March 16 and March 17.
“They issued over 200 exclusions from the tariffs, with more than a hundred of these items are the ones that were needed for medical devices and to fight COVID,” said Hillman.
Still, $1.1 billion worth of healthcare imports that could be used for treating COVID-19 remain subject to the 25% tariffs, according to a report by Chad P. Brown, senior fellow at the Peterson Institute for International Economics. Tariffs from another $3.3 billion of critical healthcare product imports were lowered from 15% to 7.5%.
General Motors (GM), partnering with Ventec to produce ventilators under the Defense Production Act, needed to source more than 700 components for the new machines. While GM could obtain most from North America, it sourced components from a handful of categories from China, which fell under a 25% tariff. They included grommets, filter parts, compressor silencers and a power cord set. GM requested exclusions from the USTR for individual parts.
GM is producing ventilators in response to the pandemic. The company needed to source more than 700 component parts for the ventilators, many of which come from China and face 25% tariffs.
AJ Mast for General Motors
These types of requests are time-consuming, especially when efforts might be better spent on other priorities during this crisis, according to legislators. Senators on both sides of the aisle pointed this out in an April letter to U.S. Trade Representative Robert Lighthizer, saying “[companies] should not be subjected to the lengthy process of submitting tariff exemption requests for each individual input required to make products essential for addressing the ongoing pandemic.”
Tethered to China
Procuring from outside of China can alleviate the risk of single sourcing and increased costs from tariffs, but it’s not always possible due to availability of raw materials, FDA clearance or production capabilities,
In June 2019, Lara Simmons, Group President of Medline Industries, explained to the USTR why a manufacturer wasn’t easily able to source many of its healthcare products, like gloves, outside of China. She said 97% of vinyl gloves come from China.
“These products are not made in the United States and some of these products are effectively available only from China. Starting production in the U.S. or any third country would be a time-consuming expensive process due to the FDA regulatory procedure that is required for these products,” she said.
The process for FDA regulated Class I and Class II medical devices can take more than two years, she said, and includes development and installation of environmental controls, facility upgrades, equipment purchase, installation, process validation and multiple rounds of audits to ensure regulatory compliance and verification of the quality system effectiveness.
Personal protective products include face masks, hand soap, sanitizer and protective spectacles.
Shefali Kapadia / Supply Chain Dive, data from World Trade Organization
Even gloves used for hospital cleaning and industrial food prep are in short supply, sending buyers back to China in spite of high tariffs.
Minnesota-based Global Glove & Safety Manufacturing applied for a tariff exemption for unsupported gloves (rubber gloves without a fabric lining), which are subject to a 25% tariff. The company’s clients that traditionally use disposable supported gloves can’t keep those in stock and are now using unsupported gloves.
“Once stability is achieved in the marketplace, we won’t buy from China for unsupported gloves, especially because of the tariffs.”
Tanner Brehmer
Product development manager, Global Glove & Safety Manufacturing
Global Glove typically buys from producers in countries including Malaysia, Sri Lanka and Thailand, but due to lockdowns and limited production in those countries, it’s trying to source some from China. “It’s tough because nothing is really shipping and lead times are pushed out so far. We don’t know when we’ll get it from other countries,” Tanner Brehmer, the company’s product development manager, told Supply Chain Dive.
The 25% tariff on the gloves produced in China greatly increases the cost, yet China is one of the only countries producing these products at full speed, he said. So in spite of tariffs, his company may move some procurement back to China. “Once stability is achieved in the marketplace, we won’t buy from China for unsupported gloves, especially because of the tariffs,” Brehmer said.
A diversified future?
Lighthizer and the Trump administration has a long-term vision for the tariffs. “Indeed, if there is one lesson to be drawn from this crisis, it is that dependence on other countries as the source of key medical products has created a strategic vulnerability for the U.S. By encouraging diversification of supply chains and—better yet—more manufacturing in the U.S., President Trump’s economic and trade policies are helping to overcome that vulnerability,” Lighthizer wrote in the The Wall Street Journal.
As healthcare systems sourced PPE and other supplies to treat COVID-19, they often paid the tariffs if needed, even if that meant paying more for the products. Healthcare systems and the government also purchased from manufacturing companies converting their domestic factories to produce needed items for COVID-19 treatment.
“We need a more resilient supply chain, which means we need to have multiple sources of supply.”
Jennifer Hillman
Senior fellow for trade and international political economy, Council on Foreign Relations
Which of these production lines will continue when the acute need for PPE is over, is hard to know. However, healthcare systems are now more aware of the risk in relying on foreign sources for their supplies.
“We need a more resilient supply chain, which means we need to have multiple sources of supply rather than sole sources of supply, and we need to do a better job of creating stockpiles,” said Hillman. “Part of the reason why we’re in such a world of hurt is because of our stockpiles were allowed to be depleted, again, in response to these tariffs.”