The healthcare industry is still licking its wounds from $1 trillion in federal funding cuts included in the One Big Beautiful Bill Act (OBBBA) signed into law July 4.
Adding insult to injury, the Center for Medicare and Medicaid services issued a 913-page proposed rule last Tuesday that includes unwelcome changes especially troublesome for hospitals i.e. adoption of site neutral payments, expansion of hospital price transparency requirements, reduction of inpatient-only services, acceleration of hospital 340B discount repayment obligations and more.
The combination of the two is bad news for healthcare overall and hospitals especially: the timing is precarious:
Economic uncertainty: Economists believe a recession is less likely but uncertainty about tariffs, fear about rising inflation, labor market volatility a housing market slowdown and speculation about interest rates have capital markets anxious. Healthcare is capital intense: the impact of the two in tandem with economic uncertainty is unsettling.
Consumer spending fragility: Consumer spending is holding steady for the time being but housing equity values are dropping, rents are increasing, student loan obligations suspended during Covid are now re-activated, prices for hospital and physicians are increasing faster than other necessities and inflation ticked up slightly last month. Consumer out-of-pocket spending for healthcare products and services is directly impacted by purchases in every category.
Heightened payer pressures: Insurers and employers are expecting double-digit increases for premiums and health benefits next year blaming their higher costs on hospitals and drugs, OBBBA-induced insurance coverage lapses and systemic lack of cost-accountability. For insurers, already reeling from 2023-2024 financial reversals, forecasts are dire. Payers will heighten pressure on healthcare providers—especially hospitals and specialists—as a result.
Why healthcare appears to have borne the brunt of the funding cuts in the OBBBA is speculative:
Might a case have been made for cuts in other departments? Might healthcare programs other than Medicaid have been ripe for “waste, fraud and abuse” driven cuts? Might technology-driven administrative costs reductions across the expanse of federal and state government been more effective than DOGE- blunt experimentation?
Healthcare is 18% of the GDP and 28% of total federal spending: that leaves room for cuts in other industries.
Why hospitals, along with nursing homes and public health programs, are likely to bear the lion’s share of OBBBA’ cut fallout and CMS’ proposed rule disruptions is equally vexing. Might the high-profile successes of some not-for-profit hospital operators have drawn attention? Might Congress have been attentive to IRS Form 990 filings for NFP operators and quarterly earnings of investor-owned systems and assume hospital finances are OK? Might advocacy efforts to maintain the status quo with facility fees, 340B drug discounts, executive compensation et al been overshadowed by concerns about consolidation-induced cost increases and disregard for affordability? Hospital emergency rooms in rural and urban communities, nursing homes, public health programs and many physicians will be adversely impacted by the OBBBA cuts: the impact will vary by state. What’s not clear is how much.
My take:
Having read both the OBBBA and CMS proposed rules and observed reactions from industry, two things are clear to me:
The antipathy toward the healthcare industry among the public and in Congress played a key role in passage of the OBBBA and regulatory changes likely to follow.
Polls show three-fourths of likely voters want to see transformational change to healthcare and two-thirds think the industry is more concerned with its profit over their care: these views lend to hostile regulatory changes. The public and the majority of elected officials think the industry prioritizes protection of the status quo over obligations to serve communities and the greater good.
The result: winners and losers in each sector, lack of continuity and interoperability, runaway costs and poor outcomes.
No sector in healthcare stands as the surrogate for the health and wellbeing of the population. There are well-intended players in each sector who seek the moral high ground for healthcare, but their boards and leaders put short-term sustainability above long-term systemness and purpose. That void needs to be filled.
The timing of these changes is predictably political.
Most of the lower-cost initiatives in both the OBBBA changes and CMS proposals carry obligations to commence in 2026—in time for the November 2026 mid-term campaigns. Most of the results, including costs and savings, will not be known before 2028 or after. They’re geared toward voters inclined to think healthcare is systemically fraudulent, wasteful and self-serving.
And they’re just the start: officials across the Departments of Health and Human Services, Justice, Commerce, Labor and Veterans Affairs will add to the lists.
Hi, everybody. I’m Elizabeth Wilkins, president and CEO of the Roosevelt Institute, and I am delighted to be here today with some big news and a very special guest. I am thrilled to announce that Nobel Prize–winning economist Paul Krugman will be joining the Roosevelt Institute as a senior fellow. Paul is one of the world’s most cited economists and widely read commentators, and for good reason. His longtime New YorkTimes column and his Substack now prove that he is not just a bold thinker, he is one of the clearest and most dynamic communicators in the field—skills that come in handy when you want to break through the noise of this moment and get people thinking about what the future of our economy and democracy might look like. And, of course, this is what Roosevelt is all about: understanding where we are in the moment and where we need to go.
So, Paul, I’m so excited to talk with you today. I started at Roosevelt in February, so we’re both new kids on the block here, and I will start with a question that I am getting a lot recently: Why your interest in affiliating with Roosevelt, and why now?
Paul Krugman:
Well, now I think because partly having retired from the New York Times, I’m free to pursue other affiliations. The Times is kind of a jealous organization. But now that I’m no longer there, I can do this. Roosevelt has been a tremendous reservoir of progressive thinking and progressive economics. I was heavily reliant on Roosevelt research particularly during the aftermath of the 2008 financial crisis—I’ve been around for a while here. [There’s] still novel stuff going on, and this seemed like a good affiliation to have in these times, to join the ranks of people with Roosevelt affiliations who have been providing really urgent commentary.
Elizabeth:
Thank you for the kind words. We appreciate it. One of the things that made your Times column such a hit for decades was the unique voice that you bring to economics: your ability to break down orthodoxy and cut to the core of what’s happening in plain terms. It almost goes without saying that there is a lot to cut through right now. We’ve seen attacks on government programs and on whole government agencies. And as you have noted and I have noted, the fate of Social Security and our social compact hangs in the balance right now. So, can you talk—with a little bit of your perspective on economic history—about what you think makes this moment unique? And through all this noise, what people should be paying attention to, and why?
Paul:
We are in a moment where we’ve lived, really since the New Deal in—whatever you want to call it—the Keynesian consensus. We’ve lived in a world where, we by no means went to socialism, but we had capitalism with some of the rough edges sanded off. Not as many of the rough edges that I would like, but we have Social Security, we’ve had Medicare since the 60s. We have Medicaid. We have the Affordable Care Act. We have a whole bunch of social insurance programs. We have government efforts to at least somewhat regulate the excesses and harms of markets. And now we are at a moment where there’s a real possibility that we may really lose that. We’re talking about possible retrogression, and the possibility of moving forward after this current moment has passed. But we really are at a point where the certainties of the underlying continuity of a fairly decent social compact is at risk. And so this is really new.
Elizabeth:
I really like that phrase, this “capitalism with the rough edges sanded off.” And what I’m hearing you say is basically the idea of the social compact is that, yes, we have capitalism, but we also have a commitment to providing a measure of security for people, and that’s the deal we have struck. You write a ton about the New Deal and FDR [Franklin D. Roosevelt]. Can you just expand a little bit about how to think about that trade-off, how long that consensus has held, and if there are any other moments in our economic history where there have been similar threats to that compact that we can learn from?
Paul:
I like to think about—it’s 1933, and the world economy has collapsed. There are a lot of reasonable people [who] have concluded that capitalism is irredeemable and can’t be saved, and that on the other hand, you have a lot of forces of repression out there. And along comes several countries—with the US in some ways leading the New Deal order, which says, no, we’re not actually going to go socialist. We’re not going to seize the commanding heights of production, but we are going to try to make sure that extreme hardship is vanished, as far as we can manage. We’re going to try to make sure that workers feel that they are a part of, and that they have rights and claims to, the system. There was very much this moment when we reached a kind of—I don’t know if it’s a compromise or a synthesis—but the idea of a basic standard of decency, the Four Freedoms. While at the same time saying that it’s not evil to make profits. It’s not evil to be personally ambitious. But we are going to try to make it so that everyone shares in the gains from economic activity.
And that really held. I mean, there was the moment when the Reagan administration came in, which represented, in many ways, a turn away from that New Deal consensus. But not to the extent that we have now. In moments of economic stress, people tend to say, well, maybe this thing doesn’t work anymore. The 1970s with stagflation, the aftermath of the 2008 financial crisis. That has basically been the case during attempts to turn away from the basic structure (which in the US context have always been a turn to the right, but in principle, you could imagine a turn to the left, but that hasn’t ever really happened in this country). And until right now, it has always seemed that the public wouldn’t stand for it. When push came to shove, when George W. Bush tried to privatize Social Security, it was a sort of resounding, “no, you don’t. We love Social Security.” But the possibility that we will have either explicitly or de facto undermining of those institutions seems much higher right now just because we live in such—well, we’re not gonna talk about the politics particularly, but there’s a possibility that we’ll lose it, that it will go away. And the one thing that I would say is that there’s this political action by itself, but there’s also the importance of getting the facts clear, getting the way the world works clear. No, there are not 10 million dead people receiving Social Security benefits. No, tax cuts and deregulation are not the only way to achieve economic growth. These are really critical things. Facts matter, analysis matters.
Elizabeth:
I’m just gonna pick up on that last thing you said about facts matter, analysis matters, and maybe go a little bit toward your true economist side. It’s not just Social Security we’re talking about. As you know and just mentioned, we’re in the middle of a tax and budget fight where we are very much looking at a situation where tax cuts for the wealthy might be traded for cuts to the programs that are specifically for our most vulnerable, like Medicaid and SNAP. This obviously has both political economy and democratic implications. It also has economic implications. Can you talk a little bit about this idea of what it means—this kind of wealth transfer, frankly, from the poorest to the richest, both in terms of hard facts, economics, and growth? And in terms of the social compacts that we’ve been talking about.
Paul:
It’s become increasingly clear that taking care of the most vulnerable members of society—it’s something you should do. It’s a moral obligation. But it’s also good economics, especially by the way of children. If you ask, a dollar spent on ensuring adequate health care and nutrition for children clearly pays off with multiple dollars of economic performance, because those children grow up to be more productive adults.
One way to say this is that conservative economic doctrine is all about punishing, it’s all about incentives: Poverty should be painful and wealth should be glorious. And what that all misses is the importance of just plain resources. That if low-income families cannot devote the resources to their children that you need to make those children fully productive adults—some will manage despite that, but just plain making sure that everybody in the country has the resources to make the most of themselves and their children is an enormously practical thing. It’s not just soft-hearted liberal talk, though I am a soft-hearted liberal, but it’s also just what you need to do if you want to make the most of your country’s potential.
Elizabeth:
I’m going to take another policy area, one actually that you know a lot about. It’s the area of focus that won you your Nobel Prize. You, in recent months, have been saying that one of the biggest risks of the Trump administration’s economic agenda is their chaotic tariff policy. We are currently recording the day after Liberation Day. And last year you predicted that the cronyism of those tariffs might be the biggest story in the long run, in addition to the chaos. So can you walk us through those risks, the chaos and the cronyism, and to what degree you’re seeing that play out for American workers and consumers? And, you know, why—I mean, there’s a lot of reasons why—but why are these tariffs different than the years that we’ve seen them in the past?
Paul:
There’s a standard economics case against tariffs, which is that it basically leads your economy to turn away from the things it’s really good at and start doing the things that it’s not especially good at. So for example, in New York, there’s lots of memories of the garment industry, but we really don’t wanna bring the garment industry back. Those were pretty bad jobs, and it happens to be stuff that can be done—where they can do it reasonably well—in Bangladesh, which desperately needs that industry, and we should be doing the things that we’re really good at instead. So that’s the classic case. What we’re discovering is that the rise of this hostility toward trade has additional costs. And the most immediate one is just plain that we don’t know what it’s gonna be.
As you said, we’re recording this the day after Liberation Day, which—nobody knows. I have to say that the actual tariff announcement shocked a lot of people, because it was both much bigger and much more arbitrary than people expected. I wouldn’t have been really shocked if there was a 15 percent across-the-board tariff, because that had been foreshadowed. But instead, there’s different tariffs for every country and this wasn’t really on anybody’s playbook. And nobody knows whether it [will] persist.
Think of yourself as being a business person trying to make decisions. You’re going to make an investment in your business—or are you? I mean, should you be spending money and making commitments on the basis that, okay, we’re gonna have 20 percent tariffs on all goods from Europe, or should you make it on the proposition that, “look, that’s crazy, those won’t last”? And both of those are defensible propositions. Anything you do, if you invest on the assumption that the tariffs are here to stay, then you’ll have made a terrible decision if they don’t. And so there’s a lot of paralysis that comes from the chaos. I’ve always been skeptical of people who invoke uncertainty as a reason that policy is holding the economy back, but because it’s often used as an argument against progressive policies: Oh, you know, your universal health care goals, that creates uncertainty. But in this case, this really is a major harmful issue.
We have not yet seen the cronyism, but it’s clearly potential. The whole root of—the reason why trade is where the dramatic stuff is happening [is because] US law creates a lot of discretion for the executive branch in tariff setting. Tariffs were only supposed to be applied as remedies for specific kinds of shocks or specific kinds of threats, but the decision about whether those conditions apply lies with the executive branch. So a president who wants to can do whatever they want on trade. And in the past, that’s always been held back by concern about: How will other countries react? What about the system? We built this global trading system. So it’s always been assumed that the president would have a wider view.
But if you take that away, then it’s not just arbitrary in terms of what are the overall levels of tariffs, it’s who gets a tariff break. And in fact, every time we do impose tariffs, there tend to be some exemptions. There are good reasons why sometimes you might want to exempt somebody from a tariff. But if it’s all arbitrary, the exemption might come because you go golfing with the president. And so that creates a lot of problematic incentives. We actually saw that in 2017, 2018, when the US was putting on tariffs—which looked trivial compared to what’s now on the plate—but it was very clear that industries and companies that were politically tied to the administration in power were much more likely to get exemptions than those that weren’t. So we actually saw this. We live in amazing times, and I mean that in the worst way. But everything that happened in the first go-around of what we called the trade war, it was really nothing—it was a skirmish compared with what’s happening now. But now, the possibilities are huge.
There’s a whole field of economic research on what the field calls rent-seeking. Economies where the way to succeed in business is not to be good at business, but to be good at cultivating political connections. And much of that actually was about tariffs and import quotas, but typically in developing countries. So there was a large concern that in places like Brazil or India, they were actually sacrificing a lot of potential gainful economic activity because businesses were focused instead on currying political favor. Well, could that happen here? Yes, it could. Very much down the road. I mean, I have to say that the speed and scale of the stuff that’s going on makes me think that we may have a global trade war and massive disruption before we even get around to the cronyism. But it’s down there, it’s in there. It’s in the mix.
Elizabeth:
We have seen, before yesterday, a real stop-start, put-on put-off, someone complains and we delay for a month. So I think we’ll really have to see, post-yesterday, where this goes. And this is a helpful roadmap for what to look for.
Paul:
And we should bear in mind also that the rest of the world has agency too. And part of the issue here is that the chaotic nature of the rollout is—again, the rest of the world has agency. And if you want to avoid getting into a lot of tit-for-tat, you probably want to at least explain what you’re doing and not be offending other countries unnecessarily. But, of course, we are doing that. I mean, to make Canada turn anti-American really takes—I didn’t think that—that wasn’t on my dance card for my career.
Elizabeth:
Roosevelt has argued for a long time for the strategic and targeted use of tariffs alongside industrial policy. And also, of course, alongside a strong sense of what rules and regulations you have to use to control unproductive uses of corporate and market power in that context, to make sure that the incentive structure that you’re creating actually targets the gains that you’re trying to make. But we’ve also argued for a way to transition into those things that takes account of some of the concerns that you’ve raised in terms of creating a stable business environment for investment, creating predictability, explaining things to mitigate the risk of fallout. And we’ve heard members of the administration say, “hey, yes.” [They] admit that this is going to be a little bit painful for a while, but it’ll be beneficial in the end.
You started to say this, but can you just pick apart for us when we hear someone say, “there might be a little bit of turmoil for a while,” what are the real costs of what that kind of turmoil might be for businesses, workers, consumers?
Paul:
I actually don’t buy—I mean, yes, there’s short-term pain, but it’s not short-term pain in exchange for a long-run gain, by any economic model I can think of applying. It’s actually short-term pain in return for probably even bigger long-term pain. The story about how this gets better is really not there.
I’m not a purist free trader. I’m not a laissez-faire guy. I mean, there’s a kind of idealized version of the post–New Deal consensus, which is, leave economic activity up to the markets, and then we’ll have a social safety net. But that has never been enough. We always need some additional stuff. We always need some industrial policy. And I think we need it more than we have actually had. But the reality is that you still want to have a lot of [trade]. International trade has, for the most part, been a plus for the US economy. There were distributional issues, but even there, it’s probably been a net-plus for the great majority of workers. And you’d want to mitigate the parts that aren’t. So the idea that shutting it down is going to produce a better outcome 5, 10 years down the pike, there’s really no clear argument to that effect. What is true is that we have this additional overlay, which is that nobody knows what the world is gonna look like next year. And so this is a tremendous inhibiting force.
Normally, when people say that, well, protectionism causes recessions, my answer has been no. There are lots of reasons not to like protectionism, but there’s no story about how it causes recessions. But protectionism where nobody knows what it’s gonna be, where nobody knows what the tariff rates are gonna be next year, that could cause a recession. So we may have the first real tariff-induced recession that I’m aware of in history, like, now.
Elizabeth:
That will give us something to keep an eye on over the next year and more.
I’m gonna change topics a little bit. We started, a little bit, to talk about power in the economy. Who has it? Who doesn’t? It’s something that you’ve explored. In your book Conscience of a Liberal, you wrote something that I really like: “The New Deal did more than create a middle-class society. It also brought America closer to its democratic ideals by giving working Americans real political power and ending the dominant position of the wealthy elite.”
Particularly in the environment we’re in today, what do you think policymakers should be thinking about in terms of what we can do to bring that New Deal power lens both to this moment and to a moment where we would have the ability to set the rules to put our country on a better course?
Paul:
There are two ends to that. One is just giving ordinary working- or middle-class people effective vehicles to exert political influence. And of course, we have the vote. (There may be that there’s no “of course” about that, but in principle, at least we have votes.) But I don’t think we really realized how much a strong union movement contributed toward making democracy work better. You can say, well, why isn’t the individual right to vote enough? And the answer is, look, there’s collective action problems. Politics is completely pervasive of things that would be good if everybody did them, but maybe [there’s] no individual incentives. So organizing politically is always hard, and unions are a big force in that—or were. And to some extent, still are, but much less than they used to be. And that’s really important. We are a less democratic country in practice because we don’t have workers organized. That’s one end of it, and there may be other ways, although I have to admit that I’m not all that creative. I think the success of unions in really making America more American in the postwar generation is something that we have never managed to find other routes to do.
Then on the other hand, there’s the question of the influence of malefactors of great wealth. The influence of vast wealth. And you don’t have to get too much into current events to say, well, we can really see that. I have to say, going back now, it looks like the plutocrats of the Gilded Age, by contemporary standards, were remarkable in their restraint and discretion. They didn’t try to buy influence as openly as the plutocrats today do. So now there are things you can do. It’s funny that our great grandfathers were much more open than we are in saying that one of the purposes of progressive taxation is to actually limit extreme wealth. And not simply because it’s more money to serve the common people, but because extreme wealth distorts democracy. Woodrow Wilson was much more willing to say things that would be regarded as extremely radical leftism now.
So really to reclaim who we are as a nation, [who we] are supposed to be, we need to work on both those ends. We need to try to empower basically working Americans, ordinary workers to have a role. And maybe there are other things besides unions, but that’s the obvious route.
And then you also need to try both with rules about money and politics, but also perhaps, if we can eventually, [through] constraining policy that limits the accumulation of enormous fortunes. That also limits that distortion because we really are in a situation now where it’s—all of the warnings about, as FDR would have said, the powers of organized money seem far more acute now than they ever did in the past.
Elizabeth:
You mentioned ideas that once were acceptable to say in polite company that seem more radical now. This is sort of the business of Roosevelt, to think big about how we can solve these questions of the maldistribution of power in the economy and do them at a structural level. And how to make ideas about that part of the common sense. You’ve talked about how that is part of what happened with the New Deal—that New Deal institutions that were at first considered novel and radical, by the Eisenhower presidency had become [a] normal part of American life. How did that happen in your view, that change in the common sense? And what made them so enduring and what lessons can we find for today about how to reorient what seems impossible and what seems a normal part of life?
Paul:
One of the things that strikes me when I look at history, both of economic institutions and of economic ideas, is that lots of things seem radical and scary until people have had a chance to experience them. So there’s the famous Nancy Pelosi quote—often out of context—where she said that for people to really understand the Affordable Care Act, we have to pass it. And it wasn’t like we were going to pull one over on people. It was that, as long as it was merely a theoretical thing, as long as it was something in prospect, it was possible to tell scare stories about death panels and just say, what will this do? But then after a few years, it becomes part of the fabric of life. And then, by the time we actually came fairly close to losing it, people were outraged because even imperfect as it is, Obamacare is a terrifically important safety net for many people.
You see that on a much larger scale [with] the New Deal changes. So if you go back to when FDR did his really stem-winding address in 1936 about the “I welcome their hatred” thing. The thing that was really the flash point—[that] was widely portrayed on one side of the political spectrum as an outrageous step that would destroy the market economy—was actually not Social Security, but unemployment insurance. It was like, “oh my god. You’re gonna actually pay people when they don’t have jobs.” And it turned out that hey, that’s okay. In fact—unemployment insurance was the most important thing that got us through COVID with minimal hardship. And now there are people, there’s always people who want to do away with these safety net programs. But things that can be made to sound ominous and radical when no one has actually experienced them can, after a few years, become part of the landscape.
The New Deal first got us through the Great Depression, then got us through the war. And by the time the war was over, we had become a very different country—and I would say a much better country—in which people accepted that, yeah, we have a kind of public responsibility to limit extreme inequality, to limit extreme hardship.
Elizabeth:
I want to close this out with a note that you struck in your final New York Timescolumn last December. It was a tough one. You wrote, “optimism has been replaced by anger and resentment,” and that “the public no longer has faith that the people running things know what they’re doing, or that we can assume that they’re being honest.”
I think that applies to government. It also applies to a lot of institutions across the board. So here is my question for you: What do you think it will take to rebuild trust in public institutions? And also, on a more personal level, how do you find the hope that we can make it there from here?
Paul:
Well, there’s nothing like actually doing good to build trust. If we can find our way past the current turmoil, I think that there’s an underlying reservoir of optimism still in America. And if we can get our way past this, all of these things that led us to this rather scary moment, then a few years of good governance can actually do wonders. I mean, I’m older than you are, and certainly older than a lot of the people I deal with, but I remember the 1990s. And although there are many imperfections and lots of things, it’s hard to remember just how positive people were feeling about America by the end of that decade. And that was thrown away through a variety of bad decisions. But still, it’s not that distant. It’s not that inconceivable.
And so I would think that the way forward is to get people in power who really do try to use it for good, get good programs, get good policy, get decent people. And there’s a lot of strengths in America. And this atmosphere of distrust and feeling that everyone is out to get you is self-serving. That will go away fairly quickly if it’s demonstrably not true.
Now personally, I’m terrified. I’m not giving up, but you can see a lot of the things that we read about in the history books about how societies go wrong are no longer abstract. We can see those emotions, we can see those forces out there. But the truth is that a better environment is actually—people become more generous, more positive when things are going okay. And we really don’t want to have a situation where [this] zero-sum, “I’ve got mine, I don’t want anybody else to get it” thinking is validated by experience. So, try to make things work is how we go from here.
Elizabeth:
I can tell you one of the things that gives me hope, Paul, is that in a moment where we are watching some institutions capitulate and fold in a way that is really disheartening, we also have some voices that are getting louder, not softer, and I think one of them is yours. So I wanna say how appreciative I know I am personally and how excited I know the [Roosevelt] Institute is generally to have you on as a senior fellow, in part because I really do think you are a voice out there that’s making sense of what’s happening. That’s helping us put into a context that we can understand the flood of news that we are experiencing. And, again, to demonstrate what it looks like to be a consistent voice with good analysis and moral clarity about what’s happening now, and also who we have been in the past and who we could be again. So we really appreciate your work, and we really appreciate you taking the time to chat today.
The Trump administration is moving into its second 100 days facing conditions more problematic than its first 100. For healthcare, this period will define the industry’s near-term future as changes in three domains unfold:
The Economy: The economy is volatile and consumer confidence is waning. The impact of tariffs on U.S. prices remains an unknown and escalating tension between the Ukraine and Russia, Israel and Palestine, Pakistan and India are worrisome. Household debt is mounting as student loans, medical debt and housing costs imperil financial security for more than half of U.S. households. The 3 major stock indices remain in the red YTD, prospects for a recession are high and investors are increasingly cautious. Net impact on healthcare organizations and public programs: negative, especially those without strong balance sheets and access to affordable private capital.
The Courts: Recent opinions by the Supreme Court and District Courts suggest a willingness to challenge the administration’s Executive Orders on immigrant deportation and due process, threats and funding cuts aimed at law firms and universities considered “woke” and layoffs initiated by DOGE and more. Court challenges will slow the administration’s agenda and create uncertainty in workplaces. Net impact: negative. Uncertainty paralyses planning and operations in every public and private healthcare organization.
The Public Mood: The afterglow of the election has dissipated and the public’s mood has shifted from guarded optimism to anxiety and despair. The public’s uncertain about tariffs and worried about household expenses. Net impact: negative. Healthcare affordability and prices are major concerns to consumers: the majority (76%) think the system is more concerned about profitability than patient care (Jarrard).
Current events in these areas portend headwinds for most public and private healthcare organizations where attention in the next 100 days will be focused in these areas:
Oversight: New rules, programmatic priorities, key personnel appointments and re-organization in HHS, CMS, the FDA and VA: RFKJ’s MAHA plans and Commission appointees, Oz’ affinity for Medicare Advantage predisposition toward value-based care and Makary’s overhaul of the FDA’s drug oversight process will be “on the table” in the next 100 days.
Funding: Healthcare funding in the FY 2026 federal budget. The GOP-controlled House and Senate can pass a budget with minimal support from Dem’s that reflects a serious effort to reduce the federal debt ($37 trillion/123% of GDP– up from $20 trillion in 2017). Healthcare cuts expected to be significant though rumored massive cuts to Medicaid unlikely.
States: State healthcare referenda and executive actions: states are evaluating price controls on drugs and hospitals, reparations from insurers for delays and prior-authorizations, scope of practice restrictions and more. Topping the watchlist in most states is Medicaid funding and potential fallout from discontinued ACA marketplace subsidies factored into the FY 2026 budget being finalized by the GOP-led Congress in DC.
SCOTUS: Supreme Court decisions will be handed down or before June 30 when SCOTUS’ 2024 term ends including Braidwood Management v. Becerra which will determine whether the Affordable Care Act’s requirement that private insurers cover preventive services without cost-sharing will continue. The court will also opine to the authority of the HHS secretary to appoint members of the U.S. Preventive Services Task Force. The potential impact of these decisions on coverage, insurance premiums and access to preventive health services is pervasive.
Financial markets: Capital markets are in a watchful waiting mode as US trade policy unfolds, inflation fluctuates, the fed’s interest rate determination is disclosed and consumer spending reacts. Private investing in healthcare remains opportunistic though deal flow is shifting and risk thresholds tightening.
Polls: Polls draw the attention of media and elected officials. They influence how organizations prioritize advocacy strategies, address consumer complaints and concerns and manage reputations. As reflected in numerous national polls, trust in the system and its key players—insurers, hospitals, drug companies—is at a historic low.
Each sector in U.S. healthcare will be impacted differently: Three face the strongest headwinds:
Hospitals: Hospitals face enormous financial challenges, especially not-for-profits, safety net, rural and veteran’s hospitals. Last week’s unfavorable SCOTUS decision against hospitals alleging DSH under-payments will cost $1 billion per year. Congressional adoption of site neutral payment policy could cost $15 billion/year. Drug prices, labor costs, insurer payment cuts and red-tape will negate operating margins and lower investment income knee-capping growth and innovation plans. Complicating matters, employed physicians will demand higher pay and more control. And Congressional budget-creators believe the sector’s 31% share of total healthcare spending makes it ripe for cuts attributable to “waste, fraud and abuse”.
Insurers: Medicare Advantage (which enjoys support by key administrators including CMS’ Mehmet Oz) has become a lightening rod of insurer criticism alongside prior authorization policies that restrict care. Coverage remains key to household financial security but insurers are seen as barriers to rather than facilitators of evidence-based cost-effective care. And the concentration of power in corporate titans (United, Humana, Cigna, CVS, Centene and others) is viewed with skepticism.
Public Health: Public health is not a priority in the U.S. health system despite recognition that social determinants account for 70% of the system’s $5 trillion spending. Most programs are funded by state and local governments with federal support limited. Public health is not seen as an investment and, in some settings treated with disdain as welfare or waste. As Mayors and Governors develop plans for the rest of 2025 and through 2026, public health cuts will be likely as federal co-funding becomes scarce.
The next 100 days will define the national agenda for the mid-term election in November 2026, reflect the solidarity of the MAGA movement and show the impact of tariffs on inflation, consumer prices and the public’s mood.
Healthcare leaders will be watching closely. All will be impacted.
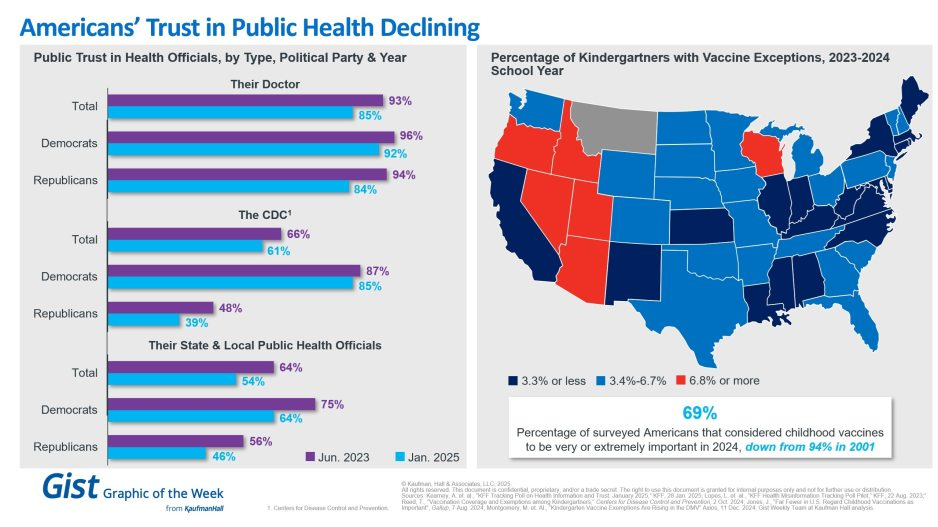
In light of the recent confirmation of Secretary Kennedy to lead HHS and new survey data on trust in public health, this graphic highlights Americans’ declining positive perception of public health officials. Among respondents’ personal doctors, the CDC and their state and local public health officials, trust in all three, regardless of political identification, has decreased from June 2023 to January 2025.
Respondents trusted their doctors more than public health officials, and there is less difference by political identification. In 2025, only 61% of surveyed Americans reported that they trusted the CDC. That prevalence drops to 39% among Republicans and increases to 85% among Democrats.
Another important public health indicator, the percentage of kindergarteners with vaccine exemptions, also illustrates the challenging place in which public health officials find themselves. During the 2023-2024 school year, about 3.3% of kindergartners received an exemption, an increase from 2022-2023 that still does not provide a complete picture. Exemption rates vary widely by state, with 6 states having exemption rates more than double the median. These differences are a reflection of how easy it is to receive an exemption in some states rather than a clear trend.
The shift also underscores how easily an outbreak could occur in some states. Alarmingly, the perceived importance of vaccines has dramatically decreased, from 94% in 2001 to 69% in 2024.
We will have to wait and see what Kennedy, long considered a vaccine skeptic, does regarding vaccines, but amid immense distrust in the healthcare system, providers’ role of giving thorough, honest information to their patients is more important than ever.
I never met Brian Thompson. His senseless death is first and foremost a human tragedy.
Second, it’s a business story that continues to unfold. Speculation about the shooter’s motive and whereabouts runs rampant.
But media attention has seized on a larger theme: the business of health insurance and its role in U.S. healthcare.
Headlines like these illustrate the storyline that has evolved in response to the killing: health insurance is part of a complicated industry where business practices are often geared to corporate profit.
Some on Social Media See Suspect in C.E.O. Killing as a Folk Hero New York Times
In this coverage and social media postings, health insurer denials are the focal point: journalists and commentators have seized on the use of Artificial intelligence-based tools used by plans like United, Cigna, Aetna and most others to approve/deny claims and Thompson’s role as CEO of UHG’s profitable insurance division.
The bullet-casing etchings “Deny. Defend. Depose” is now a T-shirt whistle to convey a wearer’s contempt for corporate insurers and the profit-seeking apparatus in U.S. healthcare.
Laid bare in the coverage of Brian’s death is this core belief: the majority of Americans think the U.S. health system is big business and fundamentally flawed.
As noted in last week’s Gallup Poll, and in previous polling by Pew, Harris, Kaiser Family Foundation and Keckley, only one in three Americans believe the health system performs well. Accessibility, costs, price transparency and affordability are dominant complaints. They believe the majority of health insurers, hospitals and prescription drug companies put their financial interests above the public’s health and wellbeing. They accept that the health system is complex and expensive but feel helpless to fix it.
This belief is widely held: its pervasiveness and intensity lend to misinformation and disinformation about the system and its business practices.
Data about underlying costs and their relationship to prices are opaque and hard to get. Clinical innovation and quality of care are understood in the abstract: self-funded campaigns touting Top 100 recognition, Net Promoter Scores are easier. The business of healthcare financing and delivery is not taught: personal experiences with insurers, hospitals, physicians and drugs are the basis for assessing the system’s effectiveness…and those experiences vary widely based on individual/household income, education, ethnicity and health status.
The majority accept that operators in every sector of healthcare apply business practices intended to optimize their organization’s finances. Best practices for every insurer, hospital, drug/device manufacturer and medical practice include processes and procedures to maximize revenues, minimize costs and secure capital for growth/innovation.
But in healthcare, the notion of profit remains problematic: how much is too much? and how an organization compensates its leaders for results beyond short-term revenue/margin improvement are questions of growing concern to a large and growing majority of consumers.
In every sector, key functions like these are especially prone to misinformation, disinformation and public criticism:
Among insurers, provider credentialing, coverage allowance and denial management, complaint management and member services, premium pricing and out-of-pocket risks for enrollees, provider reimbursement, prior authorization, provider directory accuracy, the use of AI in plan administration and others.
Among hospitals, price setting, employed physician compensation, 340B compliance, price and cost transparency, revenue-cycle management and patient debt collection, workforce performance composition, evaluation and compensation, integration of AI in clinical and administrative decision-making, participation in gainsharing/alternative payment programs, clinical portfolio and others.
And across every sector, executive compensation and CEO pay, Board effectiveness, and long-term strategies that balance shareholder interests with broader concern for the greater good.
The bottom line:
The public is paying attention to business practices in healthcare. The death of Brian Thompson opened the floodgate for criticism of health insurers and the U.S. healthcare industry overall. It cannot be ignored. The public thinks industry folks are shrewd operators and they’re inclined to conclude they’re screwed as a result.
This is National Hospital week. It comes at a critical time for hospitals:
The U.S. economy is strong but growing numbers in the population face financial insecurity and economic despair. Increased out-of-pocket costs for food, fuel and housing (especially rent) have squeezed household budgets and contributed to increased medical debt—a problem in 41% of U.S. households today. Hospital bills are a factor.
The capital market for hospitals is tightening: interest rates for debt are increasing, private investments in healthcare services have slowed and valuations for key sectors—hospitals, home care, physician practices, et al—have dropped. It’s a buyer’s market for investors who hold record assets under management (AUM) but concerns about the harsh regulatory and competitive environment facing hospitals persist. Betting capital on hospitals is a tough call when other sectors appear less risky.
Utilization levels for hospital services have recovered from pandemic disruption and operating margins are above breakeven for more than half but medical inflation, insurer reimbursement, wage increases and Medicare payment cuts guarantee operating deficits for all. Complicating matters, regulators are keen to limit consolidation and force not-for-profits to justify their tax exemptions. Not a pretty picture.
And, despite all this, the public’s view of hospitals remains positive though tarnished by headlines like these about Steward Health’s bankruptcy filing last Monday:
The public is inclined to hold hospitals in high regard, at least for the time being. When asked how much trust and confidence they have in key institutions to “to develop a plan for the U.S. health system that maximizes what it has done well and corrects its major flaws,” consumers prefer for solutions physicians and hospitals over others but over half still have reservations:
A Great Deal
Some
Not Much/None
Health Insurers
18%
43%
39%
Hospitals
27%
52%
21%
Physicians
32%
53%
15%
Federal Government
14%
42%
44%
Retail Health Org’s
21%
51%
28%
The American Hospital Association (AHA) is rightfully concerned that hospitals get fair treatment from regulators, adequate reimbursement from Medicare and Medicaid and protection against competitors that cherry-pick profits from the health system.
It can rightfully assert that declining operating margins in hospitals are symptoms of larger problems in the health system: flawed incentives, inadequate funding for preventive and primary care, the growing intensity of chronic diseases, medical inflation for wages, drugs, supplies and technologies, the dominance of ‘Big Insurance’ whose revenues have grown 12.1% annually since the pandemic and more. And it can correctly prove that annual hospital spending has slowed since the pandemic from 6.2% (2019) to 2.2% (2022) in stark contrast to prescription drugs (up from 4% to 8.4% and insurance costs (from -5.4% to +8.5%). Nonetheless, hospital costs, prices and spending are concerns to economists, regulators and elected officials.
National health spending data illustrate the conundrum for hospitals: relative to the overall CPI, healthcare prices and spending—especially outpatient hospital services– are increasing faster than prices and spending in other sectors and it’s getting attention: that’s problematic for hospitals at a time when 5 committees in Congress and 3 Cabinet level departments have their sights set on regulatory changes that are unwelcome to most hospitals.
My take:
The U.S. market for healthcare spending is growing—exceeding 5% per year through the next decade. With annual inflation targeted to 2.0% by the Fed and the GDP expected to grow 3.5-4.0% annually in the same period, something’s gotta’ give. Hospitals represent 30.4% of overall spending today (virtually unchanged for the past 5 years) and above 50% of total spending when their employed physicians and outside activities are included, so it’s obvious they’ll draw attention.
Today, however, most are consumed by near-term concerns– reimbursement issues with insurers, workforce adequacy and discontent, government mandates– and few have the luxury to look 10-20 years ahead.
I believe hospitals should play a vital role in orchestrating the health system’s future and the role they’ll play in it. Some will be specialty hubs. Some will operate without beds. Some will be regional. Some will close. And all will face increased demands from regulators, community leaders and consumers for affordable, convenient and effective whole-person care.
For most hospitals, a decision to invest and behave as if the future is a repeat of the past is a calculated risk. Others with less stake in community health and wellbeing and greater access to capital will seize this opportunity and, in the process, disable hospitals might play in the process.
Near-term reactive navigation vs. long-term proactive orchestration–that’s the crossroad in front of hospitals today. Hopefully, during National Hospital Week, it will get the attention it needs in every hospital board room and C suite.
PS: Last week, I wrote about the inclination of the 18 million college kids to protest against the healthcare status quo (“Is the Health System the Next Target for Campus Unrest?” The Keckley Report May 6, 2024 www.paulkeckley.com). This new survey caught my attention:
According to the Generation Lab’s survey of 1250 college students released last week, healthcare reform is a concern. When asked to choose 3 “issues most important to you” from its list of 13 issues, healthcare reform topped the list. The top 5:
Health Reform (40%)
Education Funding and access (38%)
Economic fairness and opportunity (37%)
Social justice and civil rights (36%)
Climate change (35%)
If college kids today are tomorrow’s healthcare workforce and influencers to their peers, addressing the future of health system with their input seems shortsighted. Most hospital boards are comprised of older adults—community leaders, physicians, et al.
And most of the mechanisms hospitals use to assess their long-term sustainability is tethered to assumptions about an aging population and Medicare.
College kids today are sending powerful messages about the society in which they aspire to be a part. They’re tech savvy, independent politically and increasingly spiritual but not religious. And the health system is on their radar.
At the Annual Meeting of the American Hospital Association in DC last week, its all-out attack on “corporate insurance” was a prominent theme. In the meeting recap, AHA CEO Rick Pollack made the influential organization’s case:
“This year, there was special focus on educating policymakers that our health care system is suffering from multiple chronic conditions.These include continued government underpayment, cyberattacks, workforce shortages, broken supply chains, access to behavioral health, and irresponsible behavior by corporate commercial health insurance companies, among others — that put access to services in serious jeopardy.”
The AHA’s declaration of war came on the heels of last week’s Congressional investigation of Change Healthcare’ (UnitedHealth Group subsidiary) cybersecurity breech and the widely-noticed earnings release by Elevance (aka Anthem) that featured prominently its plans to build a $4 billion business unit focused on primary care and chronic care management. Per company CEO Gail Boudreaux:
“This will help us continue through having a focus on advanced primary care; it’s still very much focused on our chronic patients and complex patients. We are still building specialty care enablement, which is another very important component of what we’re trying to prime through… In time, Elevance Health will have full ownership of what we expect will be a leading platform for value-based care delivery and physician enablement at scale.”
To industry watchers, the war is no surprise.
It’s been simmering for years but most recently inflamed as operating margins for most hospitals eroded while profits among corporate insurers led by Big 6 (UnitedHealth, Humana, CVS-Aetna, Elevance, Cigna, Centene) swelled at double-digit rates.
To outsiders, it’s not quite so clear.
Big names (Brands) are prominent in both. Corporatization seems embedded in the business models for both. And both appear complicit in well-documented beliefs that the health system is failing as unnecessary higher costs make it less accessible, affordable and effective.
As the War intensifies, each combatant is inclined to make their cases aggressively contrasting “us” against “them.” Here’s where things stand today:
Consideration
Hospitals
Corporate Insurers
Advantage
Public Standing
Hospitals enjoy relatively strong public support but growing discontent about their costs, prices and household affordability. Hospitals blame insurers & drug companies for increasing health costs.Increased attention to affordability, value and low prices is a threat.
Insurers enjoy reasonably high support among middle & high-income consumers who think it necessary to their financial security. Insurers blame drug companies, hospitals and unhealthy consumer behaviors for increased health costs.
It’s a tossup. Though polls show trust in hospitals is higher than insurers, both are declining especially among younger, urban and low-middle income consumers
Regulatory positioning
Scrutiny of business practices & the impact of consolidation on consumer prices, workforce wage compression, competition et al is significant and increasing in 5 Congressional Committees and 3 Federal agencies. Hospitals also face state and local regulatory challenges around pricing, community benefits, et al.
Compliance with plan transparency rules, prior authorization requirements, Medicare Advantage marketing & coverage, and antitrust are targets. Levels of Congressional attention to business practices are relatively low. Insurers are primarily overseen by states, so the regulatory landscape varies widely except.
Insurers enjoy regulatory advantages today not withstanding current attention to UnitedHealth Group. Hospitals are “soft targets” for state legislatures, Congress and investigators in state and federal agencies.
Confidence of capital markets in their core businesses: Hospitals: inpatient, outpatient careInsurers: group & individual coverage, claims data commercialization
The acute sector, especially rural & systems operating in low-growth markets, face insurmountable headwinds due to reimbursement cuts, value-based purchasing initiatives by Medicare and private insurers and clinical innovations that drive demand away from inpatient care. Hospital Outpatient services are profitable for the near term despite growing competition from privately investors.
The consolidation of power, financial strength & influence among the corporate insurers is assuring to lenders & investors who value their performance and support their vertical integration expansion role.
Lenders and investors favor “corporate insurers” over others. The potential (likelihood) that hospitals will lose on high profile revenue-enhancer issues (facility fees, site neutral payments, et al) and restrict tax exemptions for NFP hospital operators is concerning to the capital markets.
Relationships with Physicians
Hospitals employ 58% of physicians directly & relate to all. Regulations (i.e. Stark Laws, et al), capital deployment for hospital programs and administrative overhead are factors of high importance to physicians seeking clinical autonomy & financial security. Hospitals are a viable option to physicians seeking income security though not without concern.
Insurers employment of physicians plus contractual relationships with network physicians are transactional. Physicians inclined toward business relationships with “corporate insurers” believe their role in healthcare’s future is more stable than that of hospitals based on the belief hospitals are wasteful and non-responsive to physician input.
Hospitals enjoy a relationship advantage with most physicians. Corporate insurers enjoy a transactional relationship with physicians that’s premised on shared views about the future of the system vs. hospitals that focus on protecting the past. Hospitals enjoy a near-term advantage but the long-term is uncertain.
Unity of voice
Relatively strong around “chronic ailments” of the system but unclear about long-term destination and limited to universal hospital concerns (i.e. 340B) vs. cohort issues (tax exemptions for not for profits). The delineations between not-for-profit, investor-owned and public/government restricts the strength of hospital voice overall as each seeks unique recognition and regulatory protections.
Corporate insurers have corporate boards, broader membership, stronger balance sheets and scale. Their messaging is customized to their key customers and influencers and aligned with but not controlled by their trade groups. And they direct considerable resources to their proprietary messaging strategies.
Corporate insurers have fewer constraints in their messaging and enjoy an advantage in opining to issues that resonate with consumers (prices, quality, value).
Long-term Vision for the U.S. Health System
A private connected system of health in which hospitals coordinate and provide services for patients across the continuum of their care: preventive, chronic, acute and long-term.
A private system of comprehensive, customized products and services that operates efficiently, effectively and in the interests of all consumers.
The public and Congress aren’t sure which is better positioned to develop a “new” system of health.
This war has been simmering. It’s now a blaze. The outcome is uncertain despite the considerable resources both will spend to win.
Stay tuned.
Paul
P.S. Last week, I participated in Scottsdale Institute’s Annual Leadership Summit in Arizona. It’s 62 institutional members and corporate partners include most of the major not-for-profit health systems and the biggest names in healthcare information technology solutions.
I left with two strong impressions I’ll share:
1-How GenAI and HCIT influence the future of healthcare services delivery is very much speculative but no-less certain. It’s a work in process for everyone.
2- To navigate its evolution, knowledge sharing (and mistake sharing) among those in the trenches is essential. SI afforded a great venue for both, and also a platform for those of us who are easily overwhelmed by all this to ask honest questions and get candid answers.
Of late, private equity investors in healthcare services have faced intense criticism that their business practices have compromised patient safety and raised costs for consumers. March 5, the FTC, DOJ and HHS announced the launch of an investigation into the inner workings of PE in healthcare. It comes on the heels of U.S. Senate investigations in their Finance, HELP and Budget Committees to explore legislative levers they might pull to address their growing concerns about affordability, competition and accountability in the industry.
PE funds don’t welcome the spotlight.
Their business model lends to misinformation and disinformation: company takeovers by new owners are rarely treated as good news unless the circumstance under prior ownership was dire. Even then, attention shifts quickly to the fairness of the PE business model playbook: acquire the asset on favorable terms, replace management, reduce operating costs, grow and the sell in 5-7 years at a profit using debt to finance the deal along the way. In exchange, the PE fund’s General Partner gets an annual management fee of 2% plus 20% of the value they create when they sell the company or take it public, and favorable tax treatment (carried interest) on their gain.
Concern about PE in healthcare services comes at a particularly delicate time: hospitals. nursing homes, outpatient care, medical practices, clinics et al) are still feeling the after-effects of the pandemic, proposed reimbursement bumps by Medicare for hospitals and physicians do not offset medical inflation and the Change Healthcare cybersecurity breach February 21 has created cash flow issues for all.
Concern about PE ownership was high already.
Innovations funded through PE-backed organizations have been drowned out by the steady drip of peer reviewed and industry-sponsored studies a causal relationship between PE ownership decreased quality and patient safety and increased prices and worker discontent. Nonetheless, PE-owns 4% of hospitals (among 36% that are investor-owned, 13% of medical practices and 6% of nursing homes today and they’re increasing in all cohorts of health services.
Here are the facts:
Private equity enjoys significant influence in public policy including healthcare. Direct lobbying activity by PE funds in Congress and state legislatures is well-funded and effective, especially by the It is increasingly 20 global fund sponsors that control 46% of assets under management. Cash on hand and fund-raising by PE are strong and healthcare remains an important but non-exclusive target of PE investing.
2023 was a down year for PE, 2024 will be strong: the IPO market and sponsor- to sponsor transactions dipped, and deal values shrank. Even with interest rates remaining high, returns exceeded overall growth in the stock market for deals consummated. At the same time, PE raised $1.2 trillion last year and has $2.6 trillion of dry powder to invest. Healthcare services will be a target as PE deal activity increases in 2024.
In U.S. healthcare, PE investments are significant and increasing. Technology-enabled services that lower unit costs and AI-based solutions that enable standardization and workforce efficiency will garner higher valuations and greater PE interest than traditional services. Valuations will recover from record 2023 lows and dry powder will be deployed for roll-ups despite antitrust concerns and government investigations. Congress will investigate the impact on PE on patient safety, prices and competition and, in tandem with FTC and DOJ issue guidance: compliance will be mandated and financial penalties added. But displacement of PE in health services is unlikely.
Some notable data:
Private equity funds have $2.49 trillion of cash on hand to invest—up 7% from 2022. They raised $1.2 trillion globally in 2023. 26% of its global dry powder is more than 4 years old—undeployed.
Private equity groups globally are sitting on a record 28,000 unsold companies worth more than $3tn. 40% of the companies waiting to be sold are at least four years old. Last year, the combined value of companies that the industry sold privately or on public markets fell 44% and the value of companies sold to other buyout groups fell 47%.
Private equity investments in almost every sector in healthcare are significant, and until lately, increasing. Last year, deals were down 16.2% (from 940 to 788) cutting across every sector. In some sectors, like physician services, PE deals were tuck-in’s to their previous platform investments increasing from 75 deals in 2012 to 484 deals in 2021.
PE investments in US healthcare exceeded $1 trillion in the last 10 years. Investments in healthcare services i.e. acute, long-term, ambulatory and physician services– have been less profitable to investors than PE investments in technology, devices and therapeutics (based on the ratio of Enterprise Value to EBITDA) but exceed equity-market returns overall.
Peer reviewed studies have shown causal relationships between private equity ownership of hospitals, nursing homes and medical practices with lower operating costs, higher staff turnover, high prices and higher profits.
My take:
Like it or not, private equity investment in healthcare is here to stay. The likelihood of higher taxes paid by employers and individuals to fund the health system is nil. The majority (69%) of the public think it wasteful and inefficient (See Polling below). The majority believe it puts its profits above all else. The majority think it needs major change. That’s not new, but it’s felt more intensely and more widely than ever.
That means accommodation for private capital, including private equity, is not a major concern to voters: the prices they pay matters more than who owns the organization.
Tighter regulation of private equity, including more rights given to the Limited Partners who invest in the PE funds and limitations on public officials who become fund advisors, are likely. Bad actors will be vilified by regulators and elected officials. Media scrutiny of specific PE funds and their GPs will intensify as PE public reporting regulations commence. And investments made by not-for-profit multi-hospital systems and independent hospitals will be critical elements in upcoming Congressional and regulatory policy setting about their community benefit accountability and tax exemptions.
The public’s major concern about its healthcare industry is affordability. To the extent PE-backed solutions offer lower-cost, higher-value alternatives on a playing field that’s level with respect to equitable access and demand-management, they will be at the table.
To the extent PE-backed solutions cherry-pick the system’s low-hanging fruit at the expense of patient safety and affordability sans any regulatory restriction, they’ll breed public discontent from those they choose to ignore.
So, the reality is this: PE’s focus is generating profits for its GP and their LPs. Doing business in a socially responsible way is a fund’s prerogative. Some do it better than others.
PE is part of healthcare’s solution to its poorly structured, perpetually inadequate and mal-distributed funding. But creating a level playing field through meaningful regulatory reform is necessary first.
PS Among the stickier issues facing hospitals is site-neutral payments. Hospitals oppose the proposal reasoning the overhead structure for their outpatient services (HOPD) include indirect & direct costs for services provided those unable to pay i.e. emergency services. Proponents of the change argue that what’s done is the key, not where it’s done, and uniform pricing is common sense. Leavitt Partners has advanced a compromise: a Unified Ambulatory Payment System for HOPDs, ASCs and physician clinics that would be applied to 66 services starting
In the last 2 weeks, the Affordable Care Act (ACA) has been inserted itself in Campaign 2024 by Republican aspirants for the White House:
On Truth Social November 28, former President Trump promised to replace it with something better:“Getting much better Healthcare than Obamacare for the American people will be a priority of the Trump Administration. It is not a matter of cost; it is a matter of HEALTH. America will have one of the best Healthcare Plans anywhere in the world. Right now, it has one of the WORST! I don’t want to terminate Obamacare, I want to REPLACE IT with MUCH BETTER HEALTHCARE. Obamacare Sucks!!!!”
Then, on NBC’s Meet the Press December 3, Florida Governor Ron DeSantis offered “We need to have a healthcare plan that works,” Obamacare hasn’t worked. We are going to replace and supersede with a better plan….a totally different healthcare plan… big institutions that are causing prices to be high: big pharma, big insurance and big government.”
It’s no surprise. Health costs and affordability rank behind the economy as top issues for Republican voters per the latest Kaiser Tracking Poll. And distaste with the status quo is widespread and bipartisan: per the Keckley Poll (October 2023), 70% of Americans including majorities in both parties and age-cohorts under 65 think “the system is fundamentally flawed and needs major change.” To GOP voters, the ACA is to blame.
Background:
The Affordable Care Act (aka Obamacare aka the Patient Protection and Affordable Care Act) was passed into law March 23, 2013. It is the most sweeping and controversial health industry legislation passed by Congress since Lyndon Johnson’s Medicare and Medicaid Act (1965). Opinions about the law haven’t changed much in almost 14 years: when passed in 2010, 46% were favorable toward the law vs. 40% who were opposed. Today, those favorable has increased to 59% while opposition has stayed at 40% (Kaiser Tracking Poll).
Few elected officials and even fewer voters have actually read the law. It’s understandable: 955 pages, 10 major sections (Titles) and a plethora of administrative actions, executive orders, amendments and legal challenges that have followed. It continues to be under-reported in media and misrepresented in campaign rhetoric by both sides. Campaign 2024 seems likely to be more of the same.
In 2009, I facilitated discussions about health reform between the White House Office of Health Reform and the leading private sector players in the system (the American Medical Association, the American Hospital Association, America’s Health Insurance Plans, AdvaMed, PhRMA, and BIO). The impetus for these deliberations was the Obama administration’s directive that systemic reform was necessary with three-aims: reduce cost, increase access via insurance coverage and improve the quality of care provided by a private system. In parallel, key Committees in the House and Senate held hearings ultimately resulting in passage of separate House and Senate versions with the Senate’s becoming the substance of the final legislation. Think tanks on the left (I.e. the Center for American Progress et al.) and on the right (i.e. the Heritage Foundation) weighed in with members of Congress and DC influencers as the legislation morphed. And new ‘coalitions, centers and institutes’ formed to advocate for and against certain ACA provisions on behalf of their members while maintaining a degree of anonymity.
So, as the ACA resurfaces in political discourse in coming months, it’s important it be framed objectively. To that end, 3 major considerations are necessary to have a ‘fair and balanced’ view of the ACA:
1-The ACA was intended as a comprehensive health reform legislative platform. It was designed to be implemented between 2010 and 2019 in a private system prompted by new federal and state policies to address cost, access and quality. It allowed states latitude in implementing certain elements (like Medicaid expansion, healthcare marketplaces) but few exceptions in other areas (i.e.individual and employer mandates to purchase insurance, minimum requirements for qualified health plans, et al). The CBO estimated it would add $1.1 trillion to overall healthcare spending over the decade but pay for itself by reducing demand, administrative red-tape and leveraging better data for decision-making. The law included provisions to…
To improve quality by modernizing of the workforce, creating an Annual Quality Report obligation by HHS, creating the Patient Centered Outcome Research Institute and expanding the the National Quality Forum, adding requirements that approved preventive care be accessible at no cost, expanding community health centers, increasing residency programs in primary care and general surgery, implementing comparative effectiveness assessments to enable clinical transparency and more.
To increase access to health insurance by subsidizing coverage for small businesses and low income individuals (up to 400% of the Federal poverty level), funding 90% of the added costs in states choosing to expand their Medicaid enrollments for households earning up to 138% of the poverty level, extending household coverage so ‘young invincibles’ under 26 years of age could stay on their parent’s insurance plan, requiring insurers to provide “essential benefits” in their offerings, imposing medical loss ratio (MLR) mandates (80% individual, 85% group) and more.
To lower costs by creating the CMS Center for Medicare and Medicaid Innovation to construct 5-year demonstration pilots and value-based purchasing programs that shift provider incentives from volume to value, imposing price and quality reporting and transparency requirements and more.
The ACA was ambitious: it was modeled after Romneycare in MA and premised on the presumption that meaningful results could be achieved in a decade. But Romneycare (2006) was about near-universal insurance coverage for all in the Commonwealth, not the triple aim, and the resistance calcified quickly among special interests threatened by its potential.
2-The ACA passed at a time of economic insecurity and hyper-partisan rancor and before many of the industry’s most significant innovations had taken hold. The ACA was the second major legislation passed in the first term of the Obama administration (2009-2012); the first was the $831 billion American Recovery and Reconstruction Act (ARRA) stimulus package that targeted “shovel ready jobs” as a means of economic recovery from the 2008-2010 Great Recession. But notably, it included $138 billion for healthcare including requirements for hospitals and physicians to computerize their medical records, extension of medical insurance to laid off workers and additional funding for states to offset their Medicaid program expenses. The Obama-Biden team came to power with populist momentum behind their promises to lower health costs while keeping the doctors and insurance plans they had. Its rollout was plagued by miscues and the administration’s most popular assurances (‘keep your doctor and hospitals’) were not kept. The Republican Majority in the 111th Congress’ (247-193)) seized on the administration’s miss fueling anti-ACA rhetoric among critics and misinformation.
3-Support for the ACA has grown but its results are mixed. It has survived 7 Supreme Court challenges and more than 70 failed repeal votes in Congress. It enjoys vigorous support in the Biden administration and among the industry’s major trade groups but remains problematic to outsiders who believe it harmful to their interests. For example, under the framework of the ACA, the administration is pushing for larger provider networks in the 18 states and DC that run their own marketplaces, expanded dental and mental health coverage, extended open enrollment for Marketplace coverage and restoration of restrictions on “junk insurance’ but its results to date are mixed: access to insurance coverage has increased. Improvements in quality have been significant as a result of innovations in care coordination and technology-enabled diagnostic accuracy. But costs have soared: between 2010 and 2021, total health spending increased 64% while the U.S. population increased only 7%.
So, as the ACA takes center stage in Campaign 2024, here are 4 things to watch:
1-Media attention to elements of the ACA other than health insurance coverage. My bet: attention from critics will be its unanticipated costs in addition to its federal abortion protections now in the hands of states. The ACA’s embrace of price and quality transparency is of particular interest to media and speculation that industry consolidation was an unintended negative result of the law will energize calls for its replacement. Thus, the law will get more attention. Misinformation and disinformation by special interests about its original intent as a “government takeover of the health system” will be low hanging fruit for antagonists.
2- Changes to the law necessary intended to correct/mitigate its unintended consequences, modernize it to industry best practice standards and responses to court challenges will lend to the law’s complex compliance challenges for each player in the system. New ways of prompting Medicaid expansion, integration of mental health and social determinants with traditional care, the impact of tools like ChatGPT, quantum computing, generative AI not imagined as the law was built, the consequences of private equity investments on prices and spending, and much more.
3-Public confusion. The ACA is a massive law in a massive industry. Cliff’s Notes are accessible but opinions about it are rarely based on a studied view of its intent and structure. It lends itself to soundbites intended to obscure, generalize or misdirect the public’s attention.
4-The ACA price tag. In 2010, the CBO estimated its added cost to health spending at $1.1 trillion (2010-2019) but its latest estimate is at least $3 trillion for its added insurance subsidies alone. The fact is no one knows for sure what its costs are nor the value of the changes it has induced into the health system. The ranks of those with insurance coverage has been cut in half. Hospitals, physicians, post-acute providers, drug manufacturers and insurers are implementing value-based care strategies and price transparency (though reluctantly) but annual health cost increases have consistently exceeded 4% annually as the cumulative impact of medical inflation, utilization, consolidation and price increases are felt.
Final thought:
I have studied the ACA, and the enabling laws, executive orders, administrative and regulatory actions, court rulings and state referenda that have followed its passage. Despite promises to ‘repeal and replace’ by some, it is more likely foundational to bipartisan “fix and repair’ regulatory reforms that focus more attention to systemness, technology-enabled self-care, health and wellbeing and more.
It will be interesting to see how the ACA plays in Campaign 2024 and how moderators for the CNN-hosted debates January 10 in Des Moines and January 21 in New Hampshire address it. In the 2-hour Tuscaloosa debate last Wednesday, it was referenced in response to a question directed to Gov. DeSantis about ‘reforming the system’ 101 minutes into the News Nation broadcast. It’s certain to get more attention going forward and it’s certain to play a more prominent role in the future of the system.
The ACA is back on the radar in U.S. healthcare. Stay tuned.
PS The resignations under pressure of Penn President Elizabeth Magill and Board Chair Scott Bok over inappropriate characterization of Hamas’ genocidal actions toward Jews are not surprising. Her response to Congressional questioning was unfortunate. The eventuality turned in 4 days, sparked by student outrage and adverse media attention that tarnished the reputations of otherwise venerable institutions like Penn, MIT and Harvard.
The lessons for every organization, including the big names in healthcare, are not to be dismissed: Beyond the issues of genocide, our industry is home to a widening number of incendiary issues like Hamas.
They’re increasingly exposed to public smell tests that often lead to more: Workforce strikes. CEO compensation. Fraud and abuse. Tax exemptions and community benefits. Prior authorization and coverage denial. Corporate profit. Patient collection and benevolent use policies. Board independence and competence and many more are ripe for detractors and activist seeking attention.
Public opinion matters. Reputations matter. Boards of Directors are directly accountable for both.