JPMorgan Chase on May 20 unveiled its new healthcare company, dubbed Morgan Health, which its top executive told Becker’s Hospital Review can be viewed as a continuation of Haven, an ambitious healthcare venture that recently disbanded.
“We learned a lot from the Haven experience,” Dan Mendelson, CEO of Morgan Health, said. “The Haven experience focused us on primary care, digital medicine and specific populations. … You can see this as a continuation of the work that was started at Haven.”
However, Mr. Mendelson said there are several key differences between Morgan Health and Haven, the healthcare venture launched by Amazon, Berkshire Hathaway and JPMorgan Chase in 2018. For one, it has a much more simplified business structure, as it is a unit of JPMorgan Chase. Second, it has a philosophy of striking partnerships to meet its goals rather than working from the ground up.
“We don’t want to create things from scratch,” Mr. Mendelson said. “We are going to be collaborating with outstanding healthcare organizations nationally to accomplish our objectives. That’s another piece that differentiates this effort from the prior one.”
Morgan Health said its new business is focused on improving employer-sponsored healthcare in the U.S. and bringing meaningful innovation into the industry by targeting insurance and keeping populations healthy.Success for the company will be measured by whether it improves the Triple Aim: quality of care, access to care and cost to deliver care, Mr. Mendelson said. Morgan Health initially will focus its efforts on improving care for JPMorgan Chase employees, but its long-term goals are to become a leader at improving healthcare in the U.S. and to create a successful model other employers can adopt.
“We come at this with the benefit of having 285,000 employees and dependents,” Mr. Mendelson said. “We have a very strong interest in driving quality improvements for them and also creating models that are reproducible across organizations. We are looking to take a leadership role to improve care in the United States.”
Morgan Health said it has three core focus areas at its launch: improving healthcare by investing $250 million into organizations that are improving employer-sponsored healthcare; piloting new benefits for employees; and promoting healthcare equity for its employees and the broader community.
One employee benefit Morgan Health will be piloting is advanced primary care, Mr. Mendelson said. Morgan Health said it is working to create improved primary care capacity to enable employees to better navigate the healthcare system. One example of this is instead of having employees see just a primary care physician, they would be directed to a clinic that leverages more healthcare talent, such as pharmacists and nurses, to improve health outcomes.
Morgan Health said it will work with a range of partners, including provider groups, health plans and other employers. One such organization is CVS Health/Aetna, which is one of JPMorgan Chase’s insurance carriers, Mr. Mendelson said.
“CVS Health has a lot of innovation within the organization that we are not currently tapping into,” Mr. Mendelson said. “It’s a great example of a great American company that is ripe for further partnership and innovation in this effort.”
Morgan Health initially will have 20 dedicated employees, but Mr. Mendelson said the healthcare unit is tapping talent from other existing departments at JPMorgan Chase, including its legal, communications and benefits departments.
“This is a company that is very passionate about leading; there’s a very deep reservoir of support from the organization to accomplish the objectives,” Mr. Mendelson said. “These are objectives that are hard — it will take us time to accomplish and to show meaningful improvement. But there’s a sense that this is so important that there’s going to be a sustained effort in this regard and that we will achieve our objectives together.”
Prior to joining Morgan Health, Mr. Mendelson served as an operating partner at private equity firm Welsh, Carson, Anderson & Stowe. He also is the founder and former CEO of healthcare advisory firm Avalere Health and worked in the White House Office of Management and Budget during the Clinton administration.
Mr. Mendelson said his passion for establishing collaborative partnerships in healthcare will help him succeed in his new role.
CommonSpirit Health and Essentia Health have called off a deal for Essentia to acquire 14 CommonSpirit facilities in North Dakota and Minnesota, the two Catholic systems announced Tuesday.
The deal, nixed just four months after being announced, would have doubled the size of Duluth, Minn.-based Essentia’s hospital network. One of the facilities up for grabs, CHI St. Alexius Medical Center, is a tertiary hospital and the other 13 are critical access hospitals. The deal would also have included associated clinics and living communities.
The systems did not provide details as to why they scrapped the deal in their release, and an Essentia representative did not respond to a request for comment by time of publication.
Dive Insight:
CommonSpirit and Essentia signed a letter of intent in January to explore the sale, but talks have now fizzled following months of deliberation.
“While we share a similar mission, vision, values and strong commitment to sustainable rural healthcare, CommonSpirit and Essentia were unable to come to an agreement that would serve the best interests of both organizations, the people we employ and the patients we serve,” a joint statement from the two systems said.
Earlier this month, more than 700 nurses and medical workers filed a petition noting their concern over the deal. In the petition, the Minnesota Nurses Association and employees at Essentia and CommonSpirit said they feared layoffs and restricted access to patient care resulting from the acquisition.
Nurses cited Essentia’s partnership with Mercy Hospital in Moose Lake, Minn., last summer, which they claimed hurt the quality of patient care.
“Ever since the takeover, we’ve lost numerous staff, causing shortages in how we care for patients,” a nurse wrote in a news release about the petition May 4. “We don’t want CHI’s hospitals and clinics to lay off workers, cut the services they offer or close entirely.”
Essentia did not respond to a request for comment about whether workers’ concerns affected the decision to call off the deal.
Hospitals maintain consolidation betters the patient experience and improves care quality, but numerous studies have suggested that’s not the case. One from early last year published in the New England Journal of Medicine found acquired hospitals actually saw moderately worse patient experience, along with no change in 30-day mortality or readmission rates, while another from 2019 found mergers and acquisitions drive up prices for consumers.
Despite that, provider mergers and acquisitions have continued at a rapid clip even during COVID-19, as hospitals look to divest underperforming assets and bulk up market share in more lucrative geographies. The letter of intent CommonSpirit signed with Essentia suggests the roughly 140-hospital system is taking stock of its smaller rural facilities.
Chicago-based CommonSpirit was formed in 2019 by the merger of nonprofit giants Catholic Health Initiatives and Dignity Health. The nonprofit giant was hit hard by the pandemic, losing $550 million in the 2020 fiscal year.
Throughout the COVID-19 pandemic, experts have been warning of the dangers of postponed health care services. In January, the American Cancer Society, the National Comprehensive Cancer Network, and 73 other organizations, including many major health care systems, issued a statement stressing the urgency of preventive care. “We urge people across the country to talk with their health care provider to resume regular primary care checkups, recommended cancer screening, and evidence-based cancer treatment (PDF) to lessen the negative impact the pandemic is having on identifying and treating people with cancer,” the groups said.
That was sound advice not everyone could follow, as ProPublica’s Duaa Eldeib reported last week in a tragic story about Teresa Ruvalcaba. The 48-year-old single mother of three worked for 22 years at a candy factory on Chicago’s West Side. During the pandemic, disaster struck. “For more than six months, the 48-year-old factory worker had tried to ignore the pain and inflammation in her chest. She was afraid of visiting a doctor during the pandemic, afraid of missing work, afraid of losing her job, her home, her ability to take care of her three children,” Eldeib reported.
“Even though her chest felt as if it was on fire, she kept working. She didn’t want to get COVID-19 at a doctor’s office or the emergency room, and she was so busy she didn’t have much time to think about her symptoms,” Eldeib wrote.
Ruvalcaba’s pandemic fears were typical of patients across the nation, surveys revealed. A 2020 CHCF poll of 2,249 California adults revealed that even when people wanted to see a doctor for an urgent health problem, one-third did not receive care. Nearly half of those surveyed didn’t receive care for their nonurgent health problems.
Nationally, more than one in three people delayed or skipped care because they were worried about exposure to Covid-19, or because their doctor limited services, according to an Urban Institute analysis of a September 2020 survey.
The toll of this disruption in care — the forgone cancer screening, the chest pain that isn’t reported — will devastate some patients and families. Ruvalcaba had to face a diagnosis with a terrible prognosis, inflammatory breast cancer. “If she would have come six months earlier, it could have been just surgery, chemo and done,” Ruvalcaba’s doctor told Eldeib. “Now she’s incurable.”
“Unfortunately, we know we’re going to see some tragedies related to the delays,” Wiley Fowler, an oncologist at Dignity Health in Sacramento, told Ibarra.
Consequences of Delayed Care
Public health messages early in the pandemic urged people to avoid public places, including doctor’s offices. In April, as Hayley Smith noted in a Los Angeles Times story, the US Centers for Disease Control and Prevention (CDC) and the Centers for Medicare & Medicaid Services “both published guidelines recommending the postponement of elective and nonurgent procedures, including ‘low-risk cancer’ screenings, amid the first wave of the pandemic.”
Patients and doctors listened. Appointments were canceled. “Nonurgent” procedures encompassing a wide array of treatments and operations, including cancer surgeries, were delayed.
Preventive cancer screenings dropped 94% over the first four months of 2020, Eldeib reported. The National Cancer Institute expects to see 10,000 preventable deaths over the next decade because of pandemic-related delays in diagnosis and treatment of breast and colorectal cancer. Screenings for these cancers, which account for about one in six cancer deaths, are routine features of preventive care.
I know I should get another check soon, but the anxiety of COVID feels like more of a priority than the anxiety of cervical cancer.
—Molly Codner, a Southern Californian who received an abnormal Pap smear last summer
In California, cancer deaths have remained roughly the same as prepandemic rates, but that stability is not expected to last. Based on the National Cancer Institute data, Ibarra calculates that an additional 1,200 Californians will die from breast and colon cancer. The National Cancer Institute estimate is conservative “because it only accounts for a six-month delay in care, and people are postponing care longer than that,” Ibarra reported.
Nationally, death rates from cancer are expected to increase in a year or two. Slow-growing cancers will remain treatable despite a delayed diagnosis, Norman Sharpless, MD, director of the National Cancer Institute, told Eldeib. Yet for conditions like Ruvalcaba’s inflammatory breast cancer, delayed care can be disastrous.
Women, People of Color Disproportionately Affected
For women across Southern California, appointments have been delayed, exams canceled, and screenings postponed during the pandemic, Smith reported in the Los Angeles Times. “Some are voluntarily opting out for fear of encountering the virus,” Smith wrote, “while others have had their appointments canceled by health care providers rerouting resources to COVID-19 patients.”
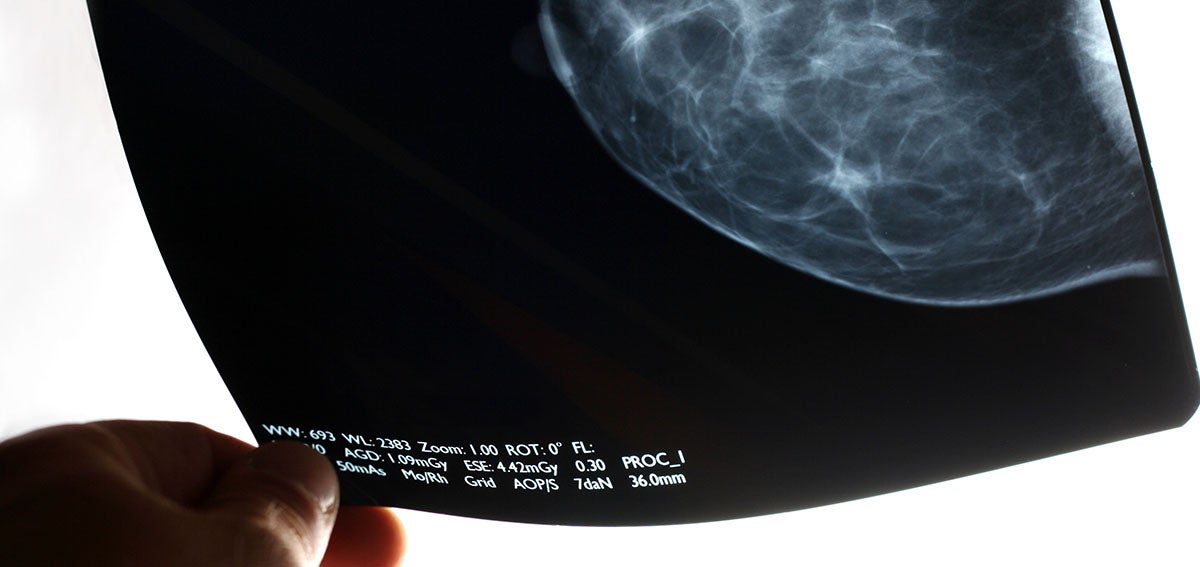
Before Pap smears became part of routine American health care, cervical cancer was one of the deadliest cancers for women. Today, as many as 93% of cervical cancer cases are preventable, according to the CDC, and screenings are a crucial component of preventive care. Yet during the first phase of California’s stay-at-home orders, cervical cancer screenings dropped 80% among the 1.5 million women in Kaiser Permanente’s regional network, Smith wrote.
The effects of the pandemic shutdown extended beyond delayed Pap smears. Women who spoke to Smith said that “mammograms, fertility treatments and even pain prevention procedures have been waylaid by the pandemic.”
Sometimes, obstacles other than the pandemic are continuing to interfere with access to care. One woman had an appointment delayed and then lost her job and her health insurance, Smith reported.
“Molly Codner, 30, has needed a checkup ever since she received an abnormal Pap smear last summer,” Smith wrote, “but like many Southern Californians, the trauma of the last year still weighs heavily on her mind: Nearly a dozen people she knows have had COVID-19.” Codner told Smith that “I know I should get another check soon, but the anxiety of COVID feels like more of a priority than the anxiety of cervical cancer.”
People who face disparities in treatment and care are most likely to be hard hit by pandemic delays. That includes Black people, who were already more likely to die from cancer than any other racial group. Cancer also is the leading cause of death among Latinx people. Breast cancer is the most common cancer diagnosis for Latinx women. Overall, more Americans die of heart disease.
Black adults are more likely than White or Latinx adults to delay or forgo care, according to researchers from the Urban Institute.
Telehealth Solved Access Issues for Some, Not All
Telehealth was a boon for patients during the pandemic year. Yet, as Ibarra notes, “there’s only so much that doctors and nurses can do through a screen.” Dental visits, mammograms, and annual wellness checks were also put on hold by the pandemic.
Unequal access is another challenge for telehealth. The benefits of the telehealth boom were not shared equally, according to a statewide survey conducted last month by the University of Southern California and the California Emerging Technology Fund.
Latinx, Asian, and Black respondents did not use telehealth as often as White respondents. USC researchers attribute these differences to “disparities in income, education and access to any kind of health care.”
Researchers at the Urban Institute report similar findings: “Black and Latinx adults were more likely than White adults to report having wanted a telehealth visit but not receiving one since the pandemic began, and that difficulties getting a telehealth visit were also more common among adults who were in poorer health or had chronic health conditions.”
After controlling for socioeconomic factors and health status, patients with limited English were half as likely to use telehealth compared to fluent English-speaking patients, the Urban Institute said. “Much work remains to ensure all patients have equitable access to remote care during and after the pandemic,” the researchers wrote.
Whether telehealth is conducted by video or phone may be crucial to ensuring access to care. A study of telehealth use at Federally Qualified Health Centers in California in 2020 found that “more primary care visits among health centers in the study occurred via audio-only visits (49%) than in-person (48%) or via video (3%). Audio-only visits comprised more than 90% of all telemedicine visits.”
“For many Californians with low incomes, the ability to connect with a doctor or their care team by phone or video is much more than a convenience,” Chris Perrone, director of CHCF’s Improving Access team, explained on The CHCF Blog. “It’s really the difference between canceling a visit because the barriers are too great or getting the timely care that they or their child needs.”
Pandemic Health Effects Will Outlast COVID-19
Public health efforts might need to focus on two goals at the same time as the US recovers from the pandemic: increasing vaccine uptake to keep COVID-19 in check and proactively managing the fallout from delayed care.
“As we focus on recovery, we have to ensure that we get vaccinated,” Efrain Talamantes, a primary care physician in East Los Angeles, told Ibarra. “But also that we have a concerted effort to manage the chronic diseases that haven’t received the attention required to avoid complications.”
The pandemic won’t end for anyone until it ends for everyone. That sentiment has been repeated so many times, by so many people, it’s easy to forget it’s not just a cliche—particularly if you live in one of the wealthy countries, like the U.S. and Israel, that has made significant moves toward what feels like an end to the COVID-19 era.
Israel, for example, has fully vaccinated more than half of its population and about 90% of its adults 50 and older are now immune to the virus—enough that the country is “busting loose” and “partying like it’s 2019,” as the Washington Post put it last week. The U.S. is a bit further behind, with nearly 30% of its population fully vaccinated, but the possibility of a post-pandemic reality is already coming into focus. While daily case counts remain high, they are far lower than they were even a few months ago—about 32,000 diagnoses were reported on April 25, compared to daily tallies well above 250,000 in January. Deaths have also trended downward for most of 2021. The U.S. Centers for Disease Control and Prevention has relaxed its guidance on travel and indoor gatherings, and some states have repealed mask mandates and other disease precautions.
But while people in certain affluent countries celebrate a return to vacations and parties, COVID-19 remains a dire threat in many nations around the world—nowhere more so than India. For five days in a row, the country has set and reset the global record for new cases in a single day, tallying about 353,000 on April 26.
By official counts, about 2,000 people in India are dying from COVID-19 every day as hospitals grow overtaxed and oxygen supplies run short. Experts say the true toll is likely even higher than that. People are dying as they desperately seek treatment, and crematoriums nationwide are overwhelmed.
It can be difficult to grapple with that devastating reality when people in countries like the U.S. are reuniting with loved ones and cautiously emerging from lockdown. How can both scenarios be happening at once? The answer, as it often has during the pandemic, lies in disparity. As of April 26, 83% of vaccinations worldwide had been given in high- and upper-middle-income countries, according to a New York Times data analysis. In the developing world, many countries are preparing for the reality that it could take until 2022 or even 2023 to reach vaccination levels already achieved by richer countries today. Even in India, one of the world’s leading vaccine manufacturers, fewer than 10% of people have gotten a vaccine—a cruel irony, as people in India die in the streets while those thousands of miles away celebrate receiving their second doses.
To truly defeat COVID-19, we must reckon with that cognitive dissonance, says Dr. Rahel Nardos, who is originally from Ethiopia and now works in the University of Minnesota’s Center for Global Health and Social Responsibility. As an immigrant and global health physician who lives in the U.S., Nardos says she inhabits two worlds: one in which the U.S. may feasibly vaccinate at least 70% of its population this year, and another in which many countries struggle to inoculate even 20% of their residents in the same time frame.
“It’s a huge disparity,” Nardos says. “We need to get out of our silos and start talking to each other and hearing each other.”
That’s imperative, first and foremost because it could save lives. More than 13,000 people around the world died from COVID-19 on April 24. Remaining vigilant about disease prevention and monitoring, and working to distribute vaccines in countries that desperately need them to fight back COVID-19 surges, could help prevent more deaths in the future. That’s especially critical for developing countries, many of which are so overwhelmed by COVID-19 that nearly all other aspects of health care have suffered. “We may be looking at five, 10 years before they can get back to their baseline, which wasn’t that great to begin with,” Nardos says.
There’s also a global health argument for distributing vaccines more equitably.Infectious diseases do not respect borders. If even one country remains vulnerable to COVID-19, that could allow the virus to keep spreading and mutating, potentially evolving to such a point that it could infect people who are vaccinated against original strains of the disease. Already, vaccine makers are exploring the possibility of booster shots to add extra protection against the more transmissible variants currently circulating in various parts of the world.
We aren’t at that point yet; currently authorized vaccines appear to hold up well against these variants. But if the virus keeps spreading for years in some areas, there’s no telling what will happen, says Jonna Mazet, an epidemiologist and emerging infectious disease expert at the University of California, Davis.
“Evolution of those new strains could go into multiple directions. They may evolve to cause more severe or less severe disease. Some of the variants [could be] more concerning for young people,” Mazet says. “The whole dynamics of the disease change.”
And if the virus is mutating somewhere, chances are good it will eventually keep spreading in multiple areas, Mazet says. “Unless or until we have a major shift, we are still going to have large parts of every country that have a susceptible population,” she says. “The virus is going to find a way.”
The only way to stop a virus from mutating is to stop giving it new hosts, and vaccines help provide that protection. COVAX—a joint initiative of the World Health Organization; Gavi, the Vaccine Alliance; the Coalition for Epidemic Preparedness Innovations; and UNICEF—was meant to ensure that people in low-income countries could get vaccinated at the same time as people in wealthier ones. COVAX is providing free vaccines to middle- and low-income countries, using funds gained through purchase agreements and donations from richer countries. But supply and funding shortages have made it difficult for the initiative to distribute vaccines as quickly as it intended to. Many of the doses it planned to disseminate were supposed to have come from the Serum Institute of India, which delayed exporting doses in March and April as India focused on domestic vaccine rollout to combat its COVID-19 surge at home.
In the meanwhile, many poorer countries have been unable to vaccinate anywhere close to as many people as would be required to reach herd immunity. That will almost surely improve as new vaccines are authorized for use by regulators around the world, and as manufacturers scale up production, but those moves may be months away.
COVAX is also developing a mechanism through which developed countries could donate vaccine doses they don’t need. Some wealthy countries, including the U.S. and Canada, have contracts to purchase more than enough doses to vaccinate their entire populations, and have signaled their intent to eventually donate unneeded supplies—but timing is everything. That is, these countries will likely only donate once they are sure their own populations have been vaccinated at a level that ensures herd immunity.
On April 25, the Biden Administration said the U.S. would provide India with raw supplies for making AstraZeneca’s vaccine, as well as COVID-19 tests and treatments, ventilators, personal protective equipment, and funding. That’s a significant shift, since the export of raw vaccine materials was previously banned, but it still doesn’t provide India with ready-to-go vaccines. That step may be next, though. The U.S. will export as many as 60 million doses of AstraZeneca’s vaccine once the shot clears federal safety reviews, the Associated Press reports.
Gian Gandhi, UNICEF’s COVAX coordinator for supply, says he fears many wealthy countries’ vaccine donations may not come until late in 2021, just when global supply is expected to ramp up. That may cause a bottleneck effect: all doses may come in at once, rather than at a slow-but-steady pace that allows countries with smaller health care networks to distribute them. “We need doses now, when we’re not able to access them via other means,” Gandhi says.
The global situation is also critical now. Worldwide, more than 5.2 million cases and 83,000 deaths were reported during the week leading up to April 18. Indian hospitals are so overrun, crowds have formed outside their doors and desperate families are trying to source their own oxygen. Hospitals in Brazil are reportedly running out of sedatives. Iran last week broke daily case count records three days in a row. Countries across Europe remain under various forms of lockdown. Vaccines won’t change those realities immediately—but without them, the global community stands little chance of containing COVID-19 worldwide.
Given regulatory barriers and structural differences in practice, private equity firms have been slow to acquire and roll up physician practices and other care assets in other countries in the same way they’ve done here in the US. But according a fascinating piece in the Financial Times,investors have targeted a different healthcare segment, one ripe for the “efficiencies” that roll-ups can bring—small veterinary practices in the UK and Ireland.
British investment firm IVC bought up hundreds of small vet practices across the UK, only to be acquired itself by Swedish firm Evidensia, which is now the largest owner of veterinary care sites, with more than 1,500 across Europe. Vets describe the deals as too good to refuse: one who sold his practice to IVC said “he ‘almost fell off his chair’ on hearing how much it was offering. The vet, who requested anonymity, says IVC mistook his shock for hesitation—and increased its offer.” (Physician executives in the US, take note.) IVC claims that its model provides more flexible options, especially for female veterinarians seeking more work-life balance than offered by the typical “cottage” veterinary practice.
But consumers have complained of decreased access to care as some local clinics have been shuttered as a result of roll-ups. Meanwhile prices, particularly for pet medications like painkillers or feline insulin, have risen as much as 40 percent—and vets aren’t given leeway to offer the discounts they previously extended to low-income customers. And with IVC attaining significant market share in some communities (for instance, owning 17 of 32 vet practices in Birmingham), questions have arisen about diminished competition and even price fixing.
The playbook for private equity is consistent across human and animal healthcare: increase leverage, raise prices for care, and slash practice costs, all with little obvious value for consumers. It remains to be seen whether and how consumers will push back—either on behalf of their beloved pets, or for the sake of their own health.
A new study out this week revived an old argument about whether telehealth visits spur more downstream care utilization compared to in-person visits, potentially raising the total cost of care. Researchers evaluated three years of claims data from Blue Cross Blue Shield of Michigan to compare patients treated for an acute upper respiratory infection via telemedicine versus an in-person visit, finding that patients who used telemedicine were almost twice as likely to have a related downstream visit (10.3 percent vs. 5.9 percent, respectively).
They concluded that these increased rates of follow-up likely negate any cost savings from replacing an in-person encounter with a less costly telemedicine visit.
Our take: so what?The study failed to address the question of whether a telemedicine visit was easier to access, or more timely than an in-person visit. Further, it evaluated data from 2016-2019, so the results should be caveated as pertaining to the “pre-COVID era”, before last year’s explosion in virtual care. Moreover, it’s unsurprising that patients who have a telemedicine visit may need more follow-up care (or that providers who deliver care virtually may be more aggressive about suggesting follow-up if symptoms change).
This focus on increased downstream care as a prima facie failure also ignores the fact that telemedicine services likely tap into pent-up, unmet demand for access to care. More access is a good thing for patients—and policymakers should consider that limiting reimbursement for virtual access to primary care (which accounts for less than 6 percent of total health spending) is unlikely to deliver the system-wide reduction in healthcare spending we need.
Now that we’ve entered a new phase of the vaccine rollout, with supply beginning to outstrip demand and all adults eligible to get vaccinated, we’re hearing from a number of health systems that their strategy is shifting from a centralized, scheduled approach to a more distributed, access-driven model. They’re recognizing that, in order to get the vaccine to harder-to-reach populations, and to convince reticent individuals to get vaccinated, they’ll need to lean more heavily on walk-in clinics, community settings, and yes—primary care physicians.
For some time, the primary care community has been complaining they’ve been overlooked in the national vaccination strategy, with health systems, pharmacy chains, and mass vaccination sites getting the lion’s share of doses. But now that we’re moving beyond the “if you build it, they will come” phase, and into the “please come get a shot” phase, we’ll need to lean much more heavily on primary care doctors, and the trusted relationships they have with their patients.
As one chief clinical officer told us this week, that means not just solving the logistical challenges of distributing vaccines to physician offices (which would be greatly aided by single-dose vials of vaccine, among other things), but planning for patient outreach. Simply advertising vaccine availability won’t suffice—now the playbook will have to include reaching out to patients to encourage them to sign up.
There will be workflow challenges as well, particularly while we await those single-dose shots—primary care clinics will likely need to schedule blocks of appointments, setting aside specific times of day or days of the week for vaccinations. The more distributed the vaccine rollout, the more operationally complex it will become. Health systems won’t be able to “get out of the vaccine business”, as one health system executive told us, because many have spent the past decade or more buying up primary care practices and rolling out urgent care locations. Now those assets must be enlisted in the service of vaccination rollout.
Health systems will have to orchestrate a “pull” strategy for vaccines, rather than the vaccination “push” they’ve been conducting for the past several months. To put it in military terms,the vaccination “air war” is over—now it’s time for what’s likely to be a protracted and difficult “ground campaign”.
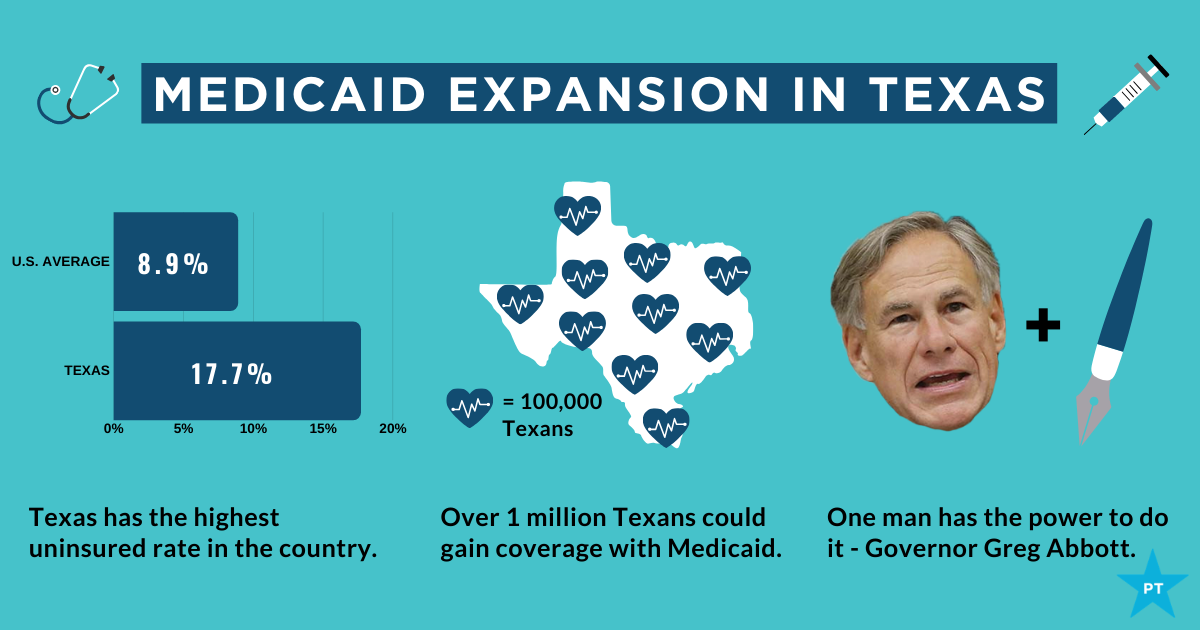
The showdown between the Biden administration and the state of Texas over Medicaid expansion continued to escalate this week. Sen. John Cornyn (R-TX) said he planned to place a hold on the confirmation of Chiquita Brooks-LaSure to become Administrator of the Centers for Medicare & Medicaid Services (CMS), until his concerns over the agency’s move last week to rescind a waiver extension previously granted by the Trump administration were addressed.
The so-called “1115 waiver”—worth more than $11B annually—would have extended by a decade Texas’ ability to use Medicaid funds to cover hospital costs for uninsured residents, rather than expanding Medicaid coverage under the Affordable Care Act (ACA). In rescinding the waiver extension, the Biden administration cited the lack of a public notice process before the waiver was granted, and said that the state’s existing waiver would instead expire next year, as previously scheduled.
Sources inside the administration told the Washington Post last week thatthe move was intended to force Texas’ hand on Medicaid expansion; the state is one of 12 that have not expanded Medicaid, leaving it with the largest share of uninsured residents of any state, with eligibility currently limited to pregnant women, children, people with disabilities, and families with monthly incomes under $300 per month, or 13.6 percent of the federal poverty level.
Enticing the dozen remaining holdout states to expand Medicaid is an important policy priority for the new administration.A key component of the recently passed American Rescue Plan Act is a package of enhanced incentives for those states to expand eligibility, offering an extended 90 percent federal match, in addition to increased funding for existing Medicaid populations.
Although none of the non-expansion states have budged yet, there has been renewed focus among state lawmakers on Medicaid expansion, including in Texas, where the idea had garnered bipartisan support. However, on Thursday, the Texas legislature voted down a proposal aimed at pushing the state toward expanding coverage for the uninsured, by an 80-68 margin. Meanwhile, the rescission of Texas’ waiver has angered the state’s Republican leadership, along with the Texas Hospital Association, whose members have benefited from the waiver’s use of funds to reimburse them for delivering uncompensated care.
While Cornyn’s hold will not ultimately stop the confirmation of the new CMS leader, the escalation on both sides over the past several days surely makes finding a compromise solution less likely. The Biden health policy team is said to be developing a new proposal, as part of an upcoming legislative package, to use the ACA marketplace to offer coverage to people in non-expansion states who might otherwise be eligible for Medicaid—yet another attempt to address one of the longest-standing points of contention stemming from the 2010 health reform law.
For some time, we’ve been focused on the efforts of Walmart to launch and grow a care delivery business, especially as it has piloted an expanded primary care clinic offering in a handful of states. We’ve long thought that access to basic care at the scale that Walmart brings could be transformative, given that more than half of Americans visit a Walmart store every week. Along those same lines, we’ve always wondered why Dollar General and Dollar Tree—each with around four times as many retail locations as Walmart—haven’t gotten into the retail clinic or pharmacy businesses.
(Part of the answer is ultra-lean staffing—this piece gives a good sense of the basic, and troubling, economics of dollar stores.) Now, as the federal government ramps up its efforts to widely distribute the COVID vaccines, it turns out that the CDC is actively discussing a partnership with Dollar General to administer the shots.
A fascinating new paper (still in preprint) from researchers at Yale shows why this could be a true gamechanger. The Biden administration, through its partnership with national and independent pharmacy providers, aims to have a vaccination site within five miles of 90 percent of the US population by next week. Compared to those pharmacy partners, researchers found,Dollar General stores are disproportionately located in areas of high “social vulnerability”, with lower income residents and high concentrations of disadvantaged groups. Particularly in the Southeast, a partnership with Dollar General would vastly increase access for low-income Black and Latino residents, allowing vaccine access within one mile for many, many more people. And the partnership could form the basis for future expansions of basic healthcare services to vulnerable and rural communities, particularly if some of the $7.5B in funding for COVID vaccine distribution went to helping dollar store locations bolster staffing and equipment to deliver basic health services. We’ll be watching with interest to see if the potential Dollar General partnership comes to fruition.