Hospitals across the country are reaching their breaking point on ICU and bed capacity as COVID surges, forcing many health systems to begin diverting patients from emergency rooms and ration care, Axios’ Orion Rummler reports.
What’s happening:
Pennsylvania: “Most hospitals in Montgomery County are at or near capacity,” county commissioners’ chair Valerie Arkoosh said in Norristown, Pennsylvania, last Wednesday.
Georgia: Major hospitals, including Grady Memorial and Emory University, have had to turn away patients brought in ambulances, the Atlanta-Journal Constitution reports.
South Dakota: The Monument Health Rapid City Hospital and Sanford USD Medical Center — some of the biggest in the state — say they have no more ICU beds, the Mitchell Republic reports.
Colorado: More than a third of hospitals across the state said in a survey they expect staffing shortages this week, Colorado Public Radio reports.
Context:White House coronavirus task force coordinator Deborah Birx noted on Sunday’s “Meet the Press” that U.S. hospitals are usually anywhere from 80 to 90% full in the fall and winter — and “when you add 10, 15, 20% COVID-19 patients on top of that, that’s what puts them at the breaking point.”
That brings the total number of enrollees to 2.9 million, a slight jump over last year but with more days to sign up over 2019.
During the fourth week of the 2020 open enrollment period, from November 22-28, 523,020 people selected plans using the HealthCare.gov platform.
That brings the total number of enrollees to 2,903,547 after the first four weeks of open enrollment. That’s an increase of 523,020 people from last year, which saw 2,380,527 consumers sign up for plans after the first four weeks.
It’s important to note, however, that in 2020 there were more days in this four-week period than last year, since the Centers for Medicare and Medicaid Services measures enrollment Sunday through Saturday. Nov. 1 was on a Sunday this year and on a Friday in 2019, so the first week of 2019 had only three days, while the first week this year measured a full seven.
The numbers are a dip from the third week of open enrollment, during which 758,421 signed up for coverage.
The HealthCare.gov platform is used by the federally facilitated exchange and some state-based exchanges. Notably, New Jersey and Pennsylvania transitioned to their own platforms for 2021, and due to this they’re absent from HealthCare.gov for 2021 coverage. Those two states accounted for 578,251 plan selections last year, 7% of all plan selections. These enrollees’ selections will not appear in CMS’ figures until it announces the state-based marketplace plan selections.
Open enrollment lasts six weeks and ends on December 14. Those who sign up within that time frame will see their coverage begin January 1, 2021.
WHAT’S THE IMPACT
This is the fourth snapshot of open enrollment figures by CMS during this sign-up period.
Of those selecting plans, 138,183 were new consumers, while 384,837 were renewing coverage. This brings the total number of new consumers to 659,455 since the beginning of open enrollment, while the tally for those renewing coverage now stands at 2,244,092. More than 4,386,530 consumers have been on the applications submitted to date.
A consumer is considered to be a new consumer if they did not have 2020 exchange coverage through Dec. 31 of this year and had a 2021 plan selection. They’re considered a renewing consumer if they have 2020 exchange coverage through Dec. 31 and actively select either the same plan or a new plan for 2021.
The numbers represent those who have submitted an application and selected a plan, net of any cancellations from a consumer, or cancellations from an insurer. The weekly metric represents the net change in the number of uncanceled plan sections over a given period.
Plan selections will not include those consumers who are automatically re-enrolled into a plan. To have their coverage effectuated, consumers generally need to pay their first month’s health plan premium. CMS did not report the number of effectuated enrollments.
In all, there were 1,749,555 HealthCare.gov users recorded during the fourth week, and 57,502 of the Spanish-speaking equivalent, CuidadoDeSalud.gov, bringing the four-week totals to 9,582,790 and 317,487, respectively.
To date, Florida tops in the number of plan selections over the first four weeks with 871,361 sign-ups, followed by Texas (471,849) and Georgia (198,090).
THE LARGER TREND
President-elect Joe Biden has said he is favorable to strengthening and expanding the Affordable Care Act, and favors a government-run public option to run parallel with private offerings.
But prior to Biden’s inauguration on Jan. 20, 2021, CMS may release a final rule based on a proposed rule it released late on Thanksgiving Eve to allow states to implement Section 1332 waivers to waive certain ACA requirements. This allows states to decentralize enrollment through insurers and web brokers. Opponents have said this will expose consumers to junk plans.
Georgia has already been approved for such a waiver.
According to a recent report from the Kaiser Family Foundation, insurer participation in the ACA marketplace in 2021 is seeing a third straight year of growth as several insurers are entering the market or expanding their service area.
For 2021, 30 insurers are entering the individual market, and an additional 61 are expanding their service area within states.
Despite taking a huge volume hit in Q2, most hospitals have managed to maintain positive operating margins—largely thanks to a $100B cash infusion from the federal government via the Coronavirus Aid, Relief and Economic Security (CARES) Act.
According to Kaufman Hall’s most recent National Hospital Flash Report, based on data from over 900 hospitals of all sizes nationwide, hospitals would have been operating at a significant loss without federal aid. As the graphic above shows, the average hospital operating margin without CARES Act relief funds would have been negative eight percent in April—and would still be in the red as of October, despite much of the cancelled elective business returning across the summer and early fall.
However, with the aid, hospitals operating margins only turned negative in April and May. When compared to the same time period last year, year-to-date (YTD) gross revenue is down almost five percent, though net patient service revenue per discharge is up—the result of longer lengths of stay, the 20 percent Medicare reimbursement bump for COVID-19 patients, and suspension of the two percent sequestration adjustment on Medicare fee-for-service payments. Yet hospital expenses per discharge are also up 13.5 percent, dampening profitability.
Though the CARES Act has been a stopgap solution for the vast majority of hospitals, a handful, most notably HCA Healthcare, have proactively returned the money. While motivations for doing so are varied, we’ve been hearing that the ever-changing reporting and spending requirements associated with CARES Act funding have many hospital leaders concerned about possible future claw-backs.
With COVID-19 hospitalizations now reaching record-breaking highs, potentially forcing another round of shut-downs, and with little movement on another round of federal relief, hospitals may be on their own for the time being—and the greatest hit to health system finances may still be yet to come.
Dallas-based Baylor Scott & White Health said it will lay off 102 employees in finance and accounting roles as part of an effort to reshape operations and reduce costs, according to The Dallas Morning News.
The duties of the affected workers will be outsourced to a third-party vendor in India. About 18 of the affected Baylor employees will be offered positions with the vendor, according to the report.
A spokesperson for Baylor Scott & White told Becker’s Hospital Review that the system will retain about two-thirds of its corporate finance department.
“Our system is continuously looking for ways to reduce costs and improve our ability to provide affordable and quality healthcare for our patients and members. As part of this, we are transforming the way we deliver our corporate finance services,” the nonprofit health system wrote in a statement obtained by Becker’s.
The cuts follow a larger round of layoffs and furloughs announced in May, which affected about 1,200 employees, or 3 percent of its workforce.
The health system said it is working to be more efficient and intentional in how resources are used. It is working to add front-line caregivers and has more than 2,000 open clinical jobs, a spokesperson told Becker’s.
“We care deeply about all our colleagues and are committed to supporting them through this process,” the statement read.
Roommates Madilyn Dennington, Bailey Mills and Olivia Noe, all 23, were issued misdemeanor citations in connection with an Oct. 31 football watch party at their East Nashville home on the 1200 block of Boscobel Street south of Fatherland Street.
Police spokesman Don Aaron said the women were served with court summonses on Monday and are slated to appear on the charges Dec. 16.
According to an arrest affidavit, officers responded about 6:30 p.m. to a complaint about a loud party at the home, heard music blaring and saw several people in the yard. In all, police said they found more than 100 people inside and outside the home.
When officers spoke to Dennington, Mills and Noe outside, they told police they had organized a watch party at their home for a football game, the affidavit states. The officers told the women that at that time, no more than 25 people were permitted to gather in Davidson County unless the gathering was approved by the city.
The women then went inside and told everyone to leave, police reported.
Police then alerted Metro Health officials about the party. Hugh Atkins, Metro Health’s environmental health services director, confirmed the Health Department did not receive an event application for the gathering.
On Tuesday, Davidson County reportedan increase of 851 cases in 24 hours — the second-highest ever daily increase. So far 369 people in Nashville have died from the virus.
Dennington is a registered nurse at TriStar Skyline Medical Center, authorities said.
It was not immediately known whether the hospital had taken any disciplinary action against Dennington. She did not return an immediate request for comment and blocked her Facebook page from a Tennessean reporter shortly after being contacted.
“Properly following pandemic regulations is extremely important to help reduce the spread of COVID-19,” Anna-Lee Cockrill, a spokeswoman for TriStar, said regarding the party. “We are looking into this further.”
According to their social media pages, all three roommates formerly attended the University of Mississippi before moving to Nashville, and Dennington and Noe both graduated from the University of Mississippi Medical Center.
Noe and Mills also could not immediately be reached for comment.
More than 50 arrests, 315 citations
Police data shows at least 50 people have been arrested and more than 315 have been cited under local emergency health orders that went into effect earlier this year.
As of Tuesday, only one of the arrested defendants had pleaded guilty: Jeffrey Mathews, a 36-year-old Goodlettsville dentist arrested for throwing an Aug. 1 house party on Fern Avenue in East Nashville. He was one of two men criminally charged for the party that drew hundreds.
Many hospitals are temporarily or permanently reducing the size of their workforce as they grapple with depleted revenues and the thorny question of when they can return to normal operating capacity. Here’s a tracker to follow the latest updates.
Hospitals across the country, financially battered as they face the dual challenges of sick COVID-19 patients and a precipitous decline in patient volume, are struggling to balance quickly shifting staffing needs. While some face and others brace for intense demand, many have announced furloughs of specialists and others that work in elective surgeries that have been drastically scaled back.
Thousands of healthcare workers at hospitals big and small have been asked not to return to work, and it’s still unclear how soon non-essential services will return. While some governors announce plans to reopen businesses, others have extended stay-at-home orders.
Most recent data from the U.S Bureau of Labor doesn’t cover the second half of March or early April, but during the first half of March, the healthcare industry shed 43,000 jobs — reversing a decade of growth in the sector. According to BLS data, the industry added 49,000 jobs in March 2019.
“Even our emergency room has seen a significant drop in patients coming in,” Sue Philips, an ICU nurse at Palomar Pomerado Health in Northern San Diego, told Healthcare Dive.
Phillips is a spokesperson with National Nurses United, the country’s largest nurses union.Palomar Health, which runs three medical centers in northern San Diego County, recently instituted 21-day temporary layoffs of 221 employees.
On April 28, Palomar announced that most of those layoffs were becoming permanent. The system laid off 5% of its workforce, eliminating 317 positions. Fifty of those employees were clinical RNs, mostly in part-time positions, and the rest spread across the organization ranging from clerical staff to technicians.
Due to a 50% decrease in patient volumes, Palomar lost $10 million in revenue in March alone, according to a statement. In April the system said it stands to lose $20 million or more.
“I’m an ICU nurse, so my job is pretty much protected,” Phillips said. “But you didn’t think you were expendable until you became expendable, and that’s a hard pill for nurses and caregivers to swallow.”
Congress has attempted to financially support struggling hospitals through ongoing coronavirus relief legislation, approving some $175 billion thus far. But without knowing what will come next, hospitals are attempting to remain nimble while reining in one of their most costly expenses — paying employees.
The following information is based on publicly reported data, along with interviews with hospital representatives and union members.
It’s not an exhaustive list, but features nonprofit and for-profit hospital systems that reported revenue above $10 billion in 2019. It also takes a look at smaller, more regionally based systems that have announced similar cutbacks.
Use the dropdown to find a company (Click on link above to access layoff tracker)
The Federal Trade Commission is revamping a key tool in its arsenal to police competition across a plethora of industries, a development that could have direct implications for future healthcare deals.
In September, the FTC said it was expanding its retrospective merger program to consider new questions and areas of study that the bureau previously has not researched extensively.
One avenue it will zero in on is labor markets, including workers and their wages, and how mergers may ultimately affect them.
It’s an area that could be ripe for scrutinizing healthcare deals, and the FTC has already begun to use this argument to bolster its case against anticompetitive tie-ups. Prior to this new argument, the antitrust agency — in its legal challenges and research — has primarily focused on how healthcare mergers affect prices.
The retrospective program is hugely important to the FTC as it is a way to examine past mergers and produce research that can be used as evidence in legal challenges to block future anticompetitive deals or even challenge already consummated deals.
“I do suspect that healthcare is a significant concern underlying why they decided to expand this program,” Bill Horton, an attorney with Jones Walker LLP, said.
So far this year, the FTC has tried to block two proposed hospital mergers. The agency sued to stop a proposed tie-up in Philadelphia in February between Jefferson Health and Albert Einstein Healthcare Network.
In both cases, the agency alleges the deals will end the robust competition that exists and harm consumers in the form of higher prices, including steeper insurance premiums, and diminished quality of services.
The agency has long leaned on the price argument (and its evidence) to challenge proposed transactions. However, recent actions signal the FTC will include a new argument: depressed wages, particularly those of nurses.
In a letter to Texas regulators in September, the FTC warned that if the state allowed a health system to acquire its only other competitor in rural West Texas, it would lead to limited wage growth among registered nurses as an already consolidated market compresses further.
Last year, the agency sent orders to five health insurance companies and two health systems to provide information so it could further study the affect COPAs, or Certificates of Public Advantage, have on price and quality. The FTC also noted it was planning to study the impact on wages.
FTC turned to review after string of defeats
A number of losses in the 1990s led the agency to conduct a hospital merger retrospective, Chris Garmon, a former economist with the FTC, said. Garmon has helped conduct and author retrospective reviews.
Between 1994 and 2000, there were about 900 hospital mergers by the U.S Department of Justice’s count. The bureau lost all seven of the cases they attempted to litigate in that time period, according to the DOJ.
The defendants in those cases succeeded by employing two types of defenses. The nonprofit hospitals would argue they would not charge higher prices because as nonprofits they had the best interests of the community in mind. Second, hospitals tried to argue that their markets were much larger than the FTC’s definition, and that they compete with hospitals many miles away.
Retrospective studies found evidence that undermined these claims. That’s why the studies are so important, Garmon said.
“It really is to better understand what happens after mergers,” Garmon said. It’s an evaluation exercise, given many transaction occur prospectively or before a deal is consummated. So the reviews help the FTC answer questions like: “Did we get it right? Or did we let any mergers we shouldn’t let through?”
The Federal Trade Commission is suing to block New Jersey’s largest health system, Hackensack Meridian Health, from acquiring a close competitor, Englewood Health. That system operates Englewood Hospital, an independent hospital and one of the last in the area, according to the Star-Ledger.
After the tie-up, Hackensack would control three of the six acute care hospitals in Bergen County, the most populated county in the state.
The loss of competition between the two would leave insurers with few options and would allow Hackensack to obtain higher prices from insurers, leading to higher premiums and higher out-of-pocket costs for consumers, the FTC alleged in a statement Thursday.
In each case, the FTC has argued the deals would eliminate close competitors and lead to higher costs and lower quality of care.
At the time, Hackensack said Englewood would become a tertiary hub for Hackensack with a focus on a slew of services lines including cardiovascular care, neurosciences and oncology. Englewood said it would also benefit from the affiliations Hackensack enjoyed with Memorial Sloan Kettering Cancer Center.
As part of the announcement, Hackensack committed to invest $400 million in Englewood Health.
Hackensack operates its flagship hospital, Hackensack University Medical Center, and partially owns Pascack Valley Medical Center, which are both within 10 miles of Englewood Hospital, according to the FTC.
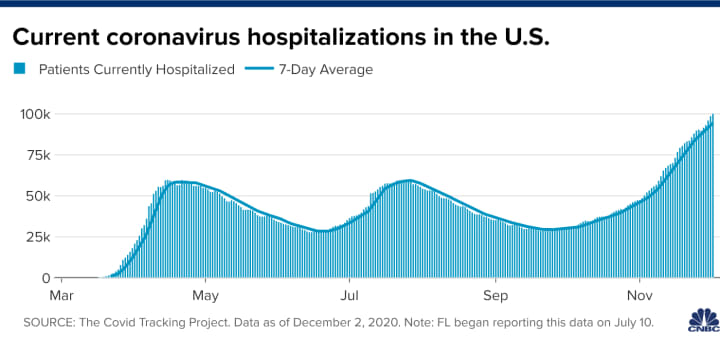
More than 100,000 Americans are now in the hospital with coronavirus infections — a new record, an indication that the pandemic is continuing to get worse and a reminder that the virus is still very dangerous.
Why it matters:Hospitalizations are a way to measure severe illnesses — and severe illnesses are on the rise across the U.S. In some areas, health systems and health care workers are already overwhelmed, and outbreaks are only getting worse.
By the numbers: For weeks, every available data point has said the same thing — that the pandemic is as bad as it’s ever been in the U.S.
Yesterday’s grim new milestone represents an 11% increase in hospitalizations over the past week, and a 26% jump over the past two weeks.
Hospitalizations are rising in 38 states, in some cases reaching unsustainable levels.
A staggering 29% of all the hospital beds in Nevada are occupied by coronavirus patients, the highest rate in the country.
That represents an enormous influx of new patients, on top of all the other people who are in the hospital for other reasons — which puts a serious strain on hospitals’ overall capacity, and on the doctors and nurses who staff them.
Fueled by that surge in coronavirus patients, 77% of Nevada’s inpatient beds and 80% of its intensive-care beds are now in use, according to federal data. And coronavirus infections are continuing to rise, so many more beds will soon be full.
Between the lines:Many rural areas already have more patients than they can handle, prompting local hospitals to send their coronavirus patients to the nearest city with some capacity left to spare. But as cases keep rising, everyone’s capacity shrinks.
In New Mexico, for example, coronavirus patients are using 27% of hospital beds. To put that number in perspective: It’s a surge that has left the entire state with just 16 ICU beds left to spare.
Coronavirus patients are also filling 20% of the hospital beds in Colorado and Arizona. And in 32 more states, at least 10% of all hospital beds have a coronavirus patient in them.
How it works: Each week, Axios has been tracking the change in new coronavirus cases. But the Thanksgiving holiday disrupted states’ reporting of those numbers, and we’re afraid that could paint a distorted picture this week.
The holiday led to some significant reporting delays, which would make the number of new cases seem artificially low — and then when states report that backlog of data all at once, the spike in cases could be artificially high.
Hospitalization data is not subject to the same reporting issues, so we’re using that this week as a more reliable measure of where the pandemic stands.
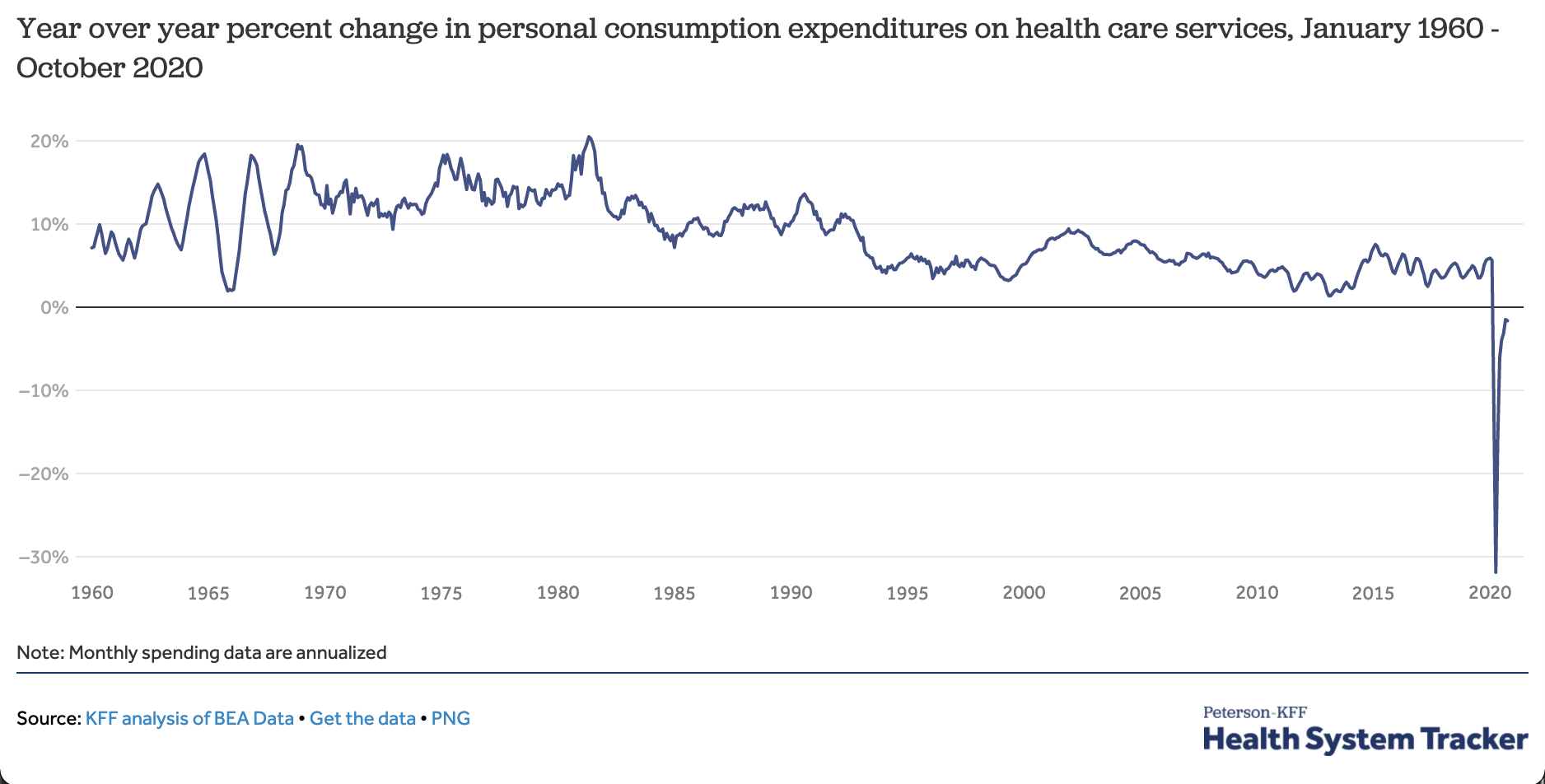
The coronavirus pandemic has caused national health care spending to go down this year — the first time that’s ever happened.
The big picture:Any big recession depresses the use of health services because people have less money to spend. But this pandemic has also directly attacked the health system, causing people to defer or skip care for fear of becoming infected.
By the numbers: Year-to-date spending on health services is down about 2% from last year. Health spending for the calendar year may end up lower than it was in 2019.
In April, when the pandemic forced many facilities to temporarily close, spending on health services had fallen an eye-popping 32% on an annualized basis.
The largest drop-offs were in outpatient care. Telehealth visits increased dramatically but did not make up all of the difference.
Context: This is the first time expenditures for patient care have fallen year-over-year since data became available in the 1960s.
What’s next: Spending and utilization have been recovering, but could fall again if the current spike in cases prompts either hospitals or patients to again hold off on elective care.
There has been a decline in cancer screenings and visits to manage chronic conditions, but it will take more research before we know precisely how this has affected outcomes.



/cloudfront-us-east-1.images.arcpublishing.com/dmn/62UNYPDOKVH6DNM7N2WSPAZQRM.JPG)