We spoke this week with a medical group president looking to deploy a more consistent consumer experience across his health system’s physician practices, beginning with primary care.
The discussion quickly turned to two large primary care practices, acquired several years ago, whose doctors are extremely resistant to change. “These guys have built a fee-for-service model that has been extremely lucrative,” the executive shared. “It was a battle getting them on centralized scheduling a few years ago, and now they’re pushing back against telemedicine.”
With ancillary income included, many of these “entrepreneurial” primary care doctors are making over $700K annually, while the rest of the system’s full-time primary care physicians average around $250K.
The situation raises several questions. Standardized access and consistent experience are foundational to consumer strategy; in the words of one CEO, if our system’s name is on the door, any of our care sites should feel like they are part of the same system, from the patient’s perspective.
But how can we get physicians on board with “systemization” if they think it puts their income at risk? Should the system guarantee income to “keep them whole”, and for how long? And is it possible to create consensus across a group of doctors with a three-fold disparity in income, and widely divergent interests? While there are no easy answers, putting patients and consumers first must be the guiding goal of the system.
Throughout the COVID-19 pandemic, experts have been warning of the dangers of postponed health care services. In January, the American Cancer Society, the National Comprehensive Cancer Network, and 73 other organizations, including many major health care systems, issued a statement stressing the urgency of preventive care. “We urge people across the country to talk with their health care provider to resume regular primary care checkups, recommended cancer screening, and evidence-based cancer treatment (PDF) to lessen the negative impact the pandemic is having on identifying and treating people with cancer,” the groups said.
That was sound advice not everyone could follow, as ProPublica’s Duaa Eldeib reported last week in a tragic story about Teresa Ruvalcaba. The 48-year-old single mother of three worked for 22 years at a candy factory on Chicago’s West Side. During the pandemic, disaster struck. “For more than six months, the 48-year-old factory worker had tried to ignore the pain and inflammation in her chest. She was afraid of visiting a doctor during the pandemic, afraid of missing work, afraid of losing her job, her home, her ability to take care of her three children,” Eldeib reported.
“Even though her chest felt as if it was on fire, she kept working. She didn’t want to get COVID-19 at a doctor’s office or the emergency room, and she was so busy she didn’t have much time to think about her symptoms,” Eldeib wrote.
Ruvalcaba’s pandemic fears were typical of patients across the nation, surveys revealed. A 2020 CHCF poll of 2,249 California adults revealed that even when people wanted to see a doctor for an urgent health problem, one-third did not receive care. Nearly half of those surveyed didn’t receive care for their nonurgent health problems.
Nationally, more than one in three people delayed or skipped care because they were worried about exposure to Covid-19, or because their doctor limited services, according to an Urban Institute analysis of a September 2020 survey.
The toll of this disruption in care — the forgone cancer screening, the chest pain that isn’t reported — will devastate some patients and families. Ruvalcaba had to face a diagnosis with a terrible prognosis, inflammatory breast cancer. “If she would have come six months earlier, it could have been just surgery, chemo and done,” Ruvalcaba’s doctor told Eldeib. “Now she’s incurable.”
“Unfortunately, we know we’re going to see some tragedies related to the delays,” Wiley Fowler, an oncologist at Dignity Health in Sacramento, told Ibarra.
Consequences of Delayed Care
Public health messages early in the pandemic urged people to avoid public places, including doctor’s offices. In April, as Hayley Smith noted in a Los Angeles Times story, the US Centers for Disease Control and Prevention (CDC) and the Centers for Medicare & Medicaid Services “both published guidelines recommending the postponement of elective and nonurgent procedures, including ‘low-risk cancer’ screenings, amid the first wave of the pandemic.”
Patients and doctors listened. Appointments were canceled. “Nonurgent” procedures encompassing a wide array of treatments and operations, including cancer surgeries, were delayed.
Preventive cancer screenings dropped 94% over the first four months of 2020, Eldeib reported. The National Cancer Institute expects to see 10,000 preventable deaths over the next decade because of pandemic-related delays in diagnosis and treatment of breast and colorectal cancer. Screenings for these cancers, which account for about one in six cancer deaths, are routine features of preventive care.
I know I should get another check soon, but the anxiety of COVID feels like more of a priority than the anxiety of cervical cancer.
—Molly Codner, a Southern Californian who received an abnormal Pap smear last summer
In California, cancer deaths have remained roughly the same as prepandemic rates, but that stability is not expected to last. Based on the National Cancer Institute data, Ibarra calculates that an additional 1,200 Californians will die from breast and colon cancer. The National Cancer Institute estimate is conservative “because it only accounts for a six-month delay in care, and people are postponing care longer than that,” Ibarra reported.
Nationally, death rates from cancer are expected to increase in a year or two. Slow-growing cancers will remain treatable despite a delayed diagnosis, Norman Sharpless, MD, director of the National Cancer Institute, told Eldeib. Yet for conditions like Ruvalcaba’s inflammatory breast cancer, delayed care can be disastrous.
Women, People of Color Disproportionately Affected
For women across Southern California, appointments have been delayed, exams canceled, and screenings postponed during the pandemic, Smith reported in the Los Angeles Times. “Some are voluntarily opting out for fear of encountering the virus,” Smith wrote, “while others have had their appointments canceled by health care providers rerouting resources to COVID-19 patients.”
Before Pap smears became part of routine American health care, cervical cancer was one of the deadliest cancers for women. Today, as many as 93% of cervical cancer cases are preventable, according to the CDC, and screenings are a crucial component of preventive care. Yet during the first phase of California’s stay-at-home orders, cervical cancer screenings dropped 80% among the 1.5 million women in Kaiser Permanente’s regional network, Smith wrote.
The effects of the pandemic shutdown extended beyond delayed Pap smears. Women who spoke to Smith said that “mammograms, fertility treatments and even pain prevention procedures have been waylaid by the pandemic.”
Sometimes, obstacles other than the pandemic are continuing to interfere with access to care. One woman had an appointment delayed and then lost her job and her health insurance, Smith reported.
“Molly Codner, 30, has needed a checkup ever since she received an abnormal Pap smear last summer,” Smith wrote, “but like many Southern Californians, the trauma of the last year still weighs heavily on her mind: Nearly a dozen people she knows have had COVID-19.” Codner told Smith that “I know I should get another check soon, but the anxiety of COVID feels like more of a priority than the anxiety of cervical cancer.”
People who face disparities in treatment and care are most likely to be hard hit by pandemic delays. That includes Black people, who were already more likely to die from cancer than any other racial group. Cancer also is the leading cause of death among Latinx people. Breast cancer is the most common cancer diagnosis for Latinx women. Overall, more Americans die of heart disease.
Black adults are more likely than White or Latinx adults to delay or forgo care, according to researchers from the Urban Institute.
Telehealth Solved Access Issues for Some, Not All
Telehealth was a boon for patients during the pandemic year. Yet, as Ibarra notes, “there’s only so much that doctors and nurses can do through a screen.” Dental visits, mammograms, and annual wellness checks were also put on hold by the pandemic.
Unequal access is another challenge for telehealth. The benefits of the telehealth boom were not shared equally, according to a statewide survey conducted last month by the University of Southern California and the California Emerging Technology Fund.
Latinx, Asian, and Black respondents did not use telehealth as often as White respondents. USC researchers attribute these differences to “disparities in income, education and access to any kind of health care.”
Researchers at the Urban Institute report similar findings: “Black and Latinx adults were more likely than White adults to report having wanted a telehealth visit but not receiving one since the pandemic began, and that difficulties getting a telehealth visit were also more common among adults who were in poorer health or had chronic health conditions.”
After controlling for socioeconomic factors and health status, patients with limited English were half as likely to use telehealth compared to fluent English-speaking patients, the Urban Institute said. “Much work remains to ensure all patients have equitable access to remote care during and after the pandemic,” the researchers wrote.
Whether telehealth is conducted by video or phone may be crucial to ensuring access to care. A study of telehealth use at Federally Qualified Health Centers in California in 2020 found that “more primary care visits among health centers in the study occurred via audio-only visits (49%) than in-person (48%) or via video (3%). Audio-only visits comprised more than 90% of all telemedicine visits.”
“For many Californians with low incomes, the ability to connect with a doctor or their care team by phone or video is much more than a convenience,” Chris Perrone, director of CHCF’s Improving Access team, explained on The CHCF Blog. “It’s really the difference between canceling a visit because the barriers are too great or getting the timely care that they or their child needs.”
Pandemic Health Effects Will Outlast COVID-19
Public health efforts might need to focus on two goals at the same time as the US recovers from the pandemic: increasing vaccine uptake to keep COVID-19 in check and proactively managing the fallout from delayed care.
“As we focus on recovery, we have to ensure that we get vaccinated,” Efrain Talamantes, a primary care physician in East Los Angeles, told Ibarra. “But also that we have a concerted effort to manage the chronic diseases that haven’t received the attention required to avoid complications.”
Late last week, retail giant Walmart announced its plan to acquire national telemedicine provider MeMD, for an undisclosed sum. According to Dr. Cheryl Pegus, Walmart’s executive vice president for health, the acquisition “complements our brick-and-mortar Walmart Health locations”, allowing the company to “expand access and reach consumers where they are”.
MeMD, founded in 2010, provides primary care and mental health services to five million patients nationally. The acquisition extends Walmart’s health delivery capabilities beyond the handful of in-store and store-adjacent clinics it runs, and follows the launch of its own Medicare Advantage-focused broker business, and partnership with Medicare Advantage start-up Clover Health to offer a co-branded insurance product.
Walmart has been climbing the healthcare learning curve for several years, building on its sizeable retail pharmacy business, and seems to have hit on a successful formula in its latest in-person clinic model, which includes primary care, behavioral health, vision, and dental services. The retailer plans to add 22 new clinic locations by the end of this year, and its new telemedicine offering will allow it to expand its virtual reach even further.
The MeMD acquisition alsorepresents a new front in Walmart’s head-to-head competition with Amazon, which launched its own national telemedicine service earlier this year. That service, Amazon Care, is targeted at the employer market, and right on cue, Amazon announced its first customer sale last week—to Precor, a fitness equipment company.
Both retail giants are slowly circling the $3.6T healthcare industry, targeting inefficiencies by deploying their expertise in convenience and consumer engagement.Incumbents beware.
Though consumers say they’re increasingly confident in returning to healthcare settings, hospital volume is not returning with the same momentum across the board. Using the most recent data from analytics firm Strata Decision Technology, covering the first quarter of this year, the graphic above shows that observation, inpatient, and emergency department volumes all remain below pre-COVID levels.
Consumers are still most wary about returning to the emergency department, with volume down nearly 20 percent across the past year. Meanwhile, hospital outpatient visits rebounded quickly, and have been growing steadily month over month, finishing March 2021 at 36 percent above the 2019 level.
Meanwhile, a recent report from the Commonwealth Fund shows that no ambulatory specialty fully made up for the COVID volume hit by the end of last year. But some areas, including rheumatology, urology, and adult primary care, have bounced back faster than others.
With continued success in rolling out vaccines and reducing COVID cases, we’d expect a continued recovery of most hospital visit volume. It may be, however, that some areas, such as the emergency department, will never fully recover to pre-COVID levels. To the extent those visits are now being replaced by more appropriate telemedicine and urgent care utilization, that’s welcome news.
But the continued lag of inpatient admissions indicates that some of the loss of emergency volume is more worrisome—warranting continued efforts on the part of providers to reassure patients it’s safe to use healthcare services. Stay tuned as our team continues to dig into this data.
A new study out this week revived an old argument about whether telehealth visits spur more downstream care utilization compared to in-person visits, potentially raising the total cost of care. Researchers evaluated three years of claims data from Blue Cross Blue Shield of Michigan to compare patients treated for an acute upper respiratory infection via telemedicine versus an in-person visit, finding that patients who used telemedicine were almost twice as likely to have a related downstream visit (10.3 percent vs. 5.9 percent, respectively).
They concluded that these increased rates of follow-up likely negate any cost savings from replacing an in-person encounter with a less costly telemedicine visit.
Our take: so what?The study failed to address the question of whether a telemedicine visit was easier to access, or more timely than an in-person visit. Further, it evaluated data from 2016-2019, so the results should be caveated as pertaining to the “pre-COVID era”, before last year’s explosion in virtual care. Moreover, it’s unsurprising that patients who have a telemedicine visit may need more follow-up care (or that providers who deliver care virtually may be more aggressive about suggesting follow-up if symptoms change).
This focus on increased downstream care as a prima facie failure also ignores the fact that telemedicine services likely tap into pent-up, unmet demand for access to care. More access is a good thing for patients—and policymakers should consider that limiting reimbursement for virtual access to primary care (which accounts for less than 6 percent of total health spending) is unlikely to deliver the system-wide reduction in healthcare spending we need.
The uncertainty and isolation of the pandemic has taken a heavy toll on mental health.Over a third of adults are currently experiencing anxiety or depression—more than three times as many as early last year. And with access to behavioral health services already challenged before the pandemic, many patients have been turning to telemedicine for support.
Health insurer Cigna found that while use of virtual care for both non-behavioral and behavioral healthcare services peaked in spring 2020, consumers have continued to use telemedicine for mental health needs, while demand for other virtual services tapered off. As of December, about 70 percent of behavioral health claims were for care rendered virtually, compared to just 20 percent across all other services.
The recent surge in demand for virtual mental health services has spurred an influx of investment into digital solutions. A recent Rock Health analysis found investments in the space have more than tripled since 2015. The injection of funds extends to both “generalist” companies (focused on a wide range of virtual services, including behavioral health) and “specialist” companies (focused solely on virtual behavioral health solutions).
Virtual behavioral health not only provides much needed access to care, but patients also prefer the privacy and ready access offered by telemedicine. Moving forward, telemedicine may become the preferred alternative for patients seeking support for mental health needs.
Amazon is expanding its virtual care pilot program, Amazon Care, to employees and outside companies nationwide beginning this summer in a major evolution of its telehealth initiative, as the COVID-19 pandemic continues to drive unprecedented demand for virtual care.
Amazon will also offer its on-demand primary care service to other Washington state-based companies and plans to expand its in-person service to Washington, D.C., Baltimore and other cities in the following months, the e-commercebehemoth announced Wednesday.
Amazon Care launched 18 months ago as a pilot program in Washington state offering free telehealth consults and in-home visits for a fee for its employees and their families.
Dive Insight:
The nationwide expansion, and the potential of the e-retailer’s heft and technological know-how leveraged in the medical delivery space, threatens existing telehealth providers and retail giants like CVS Health and Walgreens that maintain their own networks of community health clinics.
Amazon Care has two main components: urgent and primary care telehealth with a nurse or doctor via an app, and in-person care, along with prescription delivery, to the home. The Seattle-based company says it will offer the gamut from preventative care like annual vaccinations, to on-demand urgent care including COVID-19 testing, to services like family planning.
Amazon plans to roll out the virtual care offering for its employees and third party companies nationwide this year, but in-person services will only be available shortly after in Washington state and near its second headquarters in Washington, D.C., and Baltimore, a spokesperson said.
Making Amazon Care available to outside companies puts Amazon in direct competition with virtual care giants like Teladoc, Amwell and Doctor on Demand, which bring in a sizable chuck of their revenue through deals with employer and payer clients.
Amazon is in discussions with a number of outside companies on supplying Amazon Care, the spokesperson said.
It’s unclear what differentiates the virtual care offering alone from other vendors. Most telehealth platforms are available to consumers right now at little to no cost and offer relatively short wait times, though Amazon contends it provides free access to a medical professional in 60 seconds or less and will eventually link telehealth with in-home care across the U.S.
The timing for the broader U.S. rollout couldn’t be better for Amazon, as telehealth has seen exponential growth during the COVID-19 pandemic. As a result of historic consumer demand and investor interest, virtual care giants have spent billions to gobble up market share and build out their suite of services.
The race to offer end-to-end telehealth offerings has resulted in a flurry of recent M&A, the most notable deal being Teladoc’s $18.5 billion acquisition of chronic care manager Livongo last year. In February, Cigna’s health services arm Evernorth also bought vendor MDLive for undisclosed amount. The insurer plans to sell MDLive’s telehealth offerings to third-party clients and offer it to beneficiaries. And just on Tuesday, telemedicine company Doctor on Demand announced plans to merge with clinical navigator Grand Rounds to try and better coordinate virtual care.
Shares in publicly traded telehealth vendors dove following Amazon Care’s announcement Wednesday. As of late morning, Teladoc’s stock had dropped 7.4%, while Amwell was down 6.7%.
But heft doesn’t necessarily translate to disruption in healthcare.Earlier this year, Amazon, J.P. Morgan and Berkshire Hathaway disbanded their venture to lower healthcare costs after three years of stagnancy. One reason was a failure for its initiatives to take precedence at its three separate parent companies, all pursuing their own avenues to cut costs.
Now going at it alone, Amazon has a slew of independent initiatives to reshape the U.S. healthcare industry. The $386 billion company bought and launched its own online pharmacy, PillPack, a few years ago, and also partnered last year with employer health provider Crossover Health to offer employee primary care clinics. Currently, Amazon and Crossover operate clinics in 17 locations across Arizona, California, Kentucky, Michigan and Texas.
However, though Amazon Care does give patients the option to fill prescriptions through Amazon Pharmacy, it operates independently of the other services. It remains to be seen how Amazon Care could tie in with these other businesses, but the answer to that question could have major ramifications for current market leaders.
A key Medicare advisory panel is calling for a 2% bump to Medicare payments for acute care hospitals for 2022 but no hike for physicians.
The report, released Monday from the Medicare Payment Advisory Commission (MedPAC)—which recommends payment policies to Congress—bases payment rate recommendations on data from 2019. However, the commission did factor in the pandemic when evaluating the payment rates and other policies in the report to Congress, including whether policies should be permanent or temporary.
“The financial stress on providers is unpredictable, although it has been alleviated to some extent by government assistance and rebounding service utilization levels,” the report said.
MedPAC recommended that targeted and temporary funding policies are the best way to help providers rather than a permanent hike for payments that gets increased over time.
“Overall, these recommendations would reduce Medicare spending while preserving beneficiaries’ access to high-quality care,” the report added.
MedPAC expects the effects of the pandemic, which have hurt provider finances due to a drop in healthcare use, to persist into 2021 but to be temporary.
It calls for a 2% update for inpatient and outpatient services for 2022, the same increase it recommended for 2021.
The latest report recommends no update for physicians and other professionals. The panel also does not want any hikes for four payment systems: ambulatory surgical centers, outpatient dialysis facilities, skilled nursing facilities and hospices.
MedPAC also recommends Congress reduce the aggregate hospice cap by 20% and that “ambulatory surgery centers be required to report cost data to [Centers for Medicare & Medicaid Services (CMS)],” the report said.
But it does call for long-term care hospitals to get a 2% increase and to reduce payments by 5% for home health and inpatient rehabilitation facilities.
The panel also explores the effects of any policies implemented under the COVID-19 public health emergency, which is likely to extend through 2021 and could continue into 2022.
For instance, CMS used the public health emergency to greatly expand the flexibility for providers to be reimbursed for telehealth services. Use of telehealth exploded during the pandemic after hesitancy among patients to go to the doctor’s office or hospital for care.
“Without legislative action, many of the changes will expire at the end of the [public health emergency],” the report said.
MedPAC recommends Congress temporarily continue some of the telehealth expansions for one to two years after the public health emergency ends. This will give lawmakers more time to gather evidence on the impact of telehealth on quality and Medicare spending.
“During this limited period, Medicare should temporarily pay for specified telehealth services provided to all beneficiaries regardless of their location, and it should continue to cover certain newly-covered telehealth services and certain audio-only telehealth services if there is potential for clinical benefit,” according to a release on the report.
After the public health emergency ends, Medicare should also return to paying the physician fee schedule’s facility rate for any telehealth services. This will ensure Medicare can collect data on the cost for providing the services.
“Providers should not be allowed to reduce or waive beneficiary cost-sharing for telehealth services after the [public health emergency],” the report said. “CMS should also implement other safeguards to protect the Medicare program and its beneficiaries from unnecessary spending and potential fraud related to telehealth.”
The Medicare Act “prohibits Medicare payment for services that are not furnished within the United States,” according to the filing.
RemoteICU, a telemedicine provider group, is suing the Department of Health and Human Services and the Centers for Medicare and Medicaid Services for not reimbursing telehealth services provided by physicians who are located outside the United States, according to a federal lawsuit filed last week in Washington.
RICU wants reimbursement for telehealth services provided within the U.S., but not necessarily by a physician who lives within its borders.
The company employs physicians who live outside the country, but are U.S. board-certified critical-care specialists and licensed in one or more U.S. jurisdictions. With RICU’s telecommunications system, these physicians can provide critical-care services in U.S. hospital ICUs, the lawsuit said.
“Although RICU’s physicians live abroad, they serve as full-time, permanent staff members of the U.S. hospitals at which they serve patients,” the company said in the court filing.
“By employing U.S.-licensed intensivists who live overseas, RICU has enabled the American healthcare system to recapture talent that would otherwise be lost to it – and this has helped to alleviate the ongoing shortage of intensivists in American hospitals.“
When CMS expanded the list of telehealth services for which it reimbursed in December 2020 to include critical care services, RICU began offering its physicians to hospitals that couldn’t afford ICU telehealth without Medicare reimbursement, the court filing said.
However, after the company reached out to several officials from HHS and CMS, it was notified that Medicare could not reimburse the client hospitals for RICU’s services, because the Medicare Act “prohibits Medicare payment for services that are not furnished within the United States,” according to the filing.
The company is seeking a preliminary injunction to stop HHS and CMS from denying Medicare reimbursement for telehealth services on the basis of a provider’s physical location outside of the United States at the time of service.
WHAT’S THE IMPACT?
RICU claims that, by failing to reimburse for the critical care telehealth services provided by its physicians, HHS and CMS are causing “immediate harm both to RICU and to the public.”
It argues that it’s filling a gap in critical care that has been exacerbated by the pandemic.
“There remains [a] significant unmet need for critical care services, as desperately sick patients have overwhelmed ICU resources across the country,” RICU said in the court filing.
“In some cases, lack of adequate care can mean the difference between life or death. And one of the groups most at risk from death and serious illness due to COVID-19 is the elderly – the very same population that relies upon Medicare.”
Without reimbursement, RICU says that some of its current clients, as well as potential customers, will not be able to offer its services.
The company argues that this causes “significant, unrecoverable monetary damages” because tele-ICU providers that use physicians located within the U.S. are eligible for reimbursement and therefore have a competitive edge over RICU.
Further, it says that it has already begun losing business because of hospitals’ inability to receive Medicare reimbursement.
THE LARGER TREND
CMS has widely expanded the list of telehealth services it will reimburse for during the pandemic to include services such as emergency department visits, initial inpatient and nursing facility visits, and discharge-day management.
While only 14 states currently have true “payment parity” for telehealth, 43 states and D.C. have implemented a telemedicine coverage law, according to Foley & Lardner report.
That report, among others, claims telehealth will continue to grow as an integral part of healthcare as time goes on.
Last year, Geisinger health system in Danville, Pennsylvania, implemented telehealth ICU technology in several of its hospitals to support its in-person clinical staff.
ON THE RECORD
“The Critical Care Ban is causing irreparable harm to RICU, which is suffering ongoing financial and reputational harms that cannot be remedied in the future,” the court filing said.
“The balance of the equities favors an injunction, because Defendants have already admitted that there is a desperate medical need for the critical care that RICU would provide but for the Critical Care Ban.
“And, finally, preliminary injunction would be in the public interest because, across the United States, Americans stricken by the COVID-19 pandemic are in desperate need of critical care – a need that RICU can help meet. It is not hyperbole to say that the requested injunctive relief is in the public interest because it could save lives.”
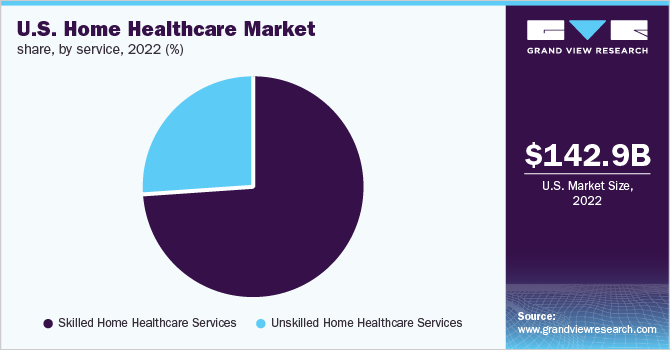
This week Brookdale Senior Living, the nation’s largest operator of senior housing, with 726 communities across 43 states and annual revenues of about $3B, announced the sale of 80 percent of its hospice and home-based care division to hospital operator HCA Healthcare for $400M. The transaction gives HCA control of Brookdale’s 57 home health agencies, 22 hospice agencies, and 84 outpatient therapy locations across a 26-state footprint, marking its entry into new lines of business, and allowing it to expand revenue streams by continuing to treat patients post-discharge, in home-based settings.
Like other senior living providers, Brookdale has struggled economically during the COVID pandemic; its home and hospice care division, which serves 17,000 patients, saw revenue drop more than 16 percent last year. HCA, meanwhile, has recovered quickly from the COVID downturn, and has signaled its intention to focus on continued growth by acquisition across 2021.
In separate news, Optum, the services division of insurance giant UnitedHealth Group, was reported to have struck a deal to acquire Landmark Health, a fast-growing home care company whose services are aimed at Medicare Advantage-enrolled, frail elderly patients. Landmark, founded in 2014, also participates in Medicare’s Direct Contracting program.
The transaction is reportedly valued at $3.5B, although neither party would confirm or comment on the deal. The acquisition would greatlyexpand Optum’s home-based care delivery services, which today include physician home visits through its HouseCalls program, and remote monitoring through its Vivify Health unit.
The Brookdale and Landmark deals, along with earlier acquisitions by Humana and others, indicate that the home-based care space is heating up significantly,reflecting a broader shift in the nexus of care to patients’ homes—a growing preference among consumers spooked by the COVID pandemic.
Along with telemedicine, home-based care may represent a new front in the tug-of-war between providers and payers for the loyalty of increasingly empowered healthcare consumers.