UPDATE: May 15, 2020: This article has been updated to include information from a Moody’s Investors Service report.
From the Mayo Clinic to Kaiser Permanente, nonprofit hospitals are posting massive losses as the coronavirus pandemic upends their traditional way of doing business.
Fitch Ratings analysts predict a grimmer second quarter: “the worst on record for most,” Kevin Holloran, senior director for Fitch, said during a Tuesday webinar.
Over the past month, Fitch has revised its nonprofit hospital sector outlook from stable to negative. It has yet to change its ratings outlook to negative, though the possibility wasn’t ruled out.
Some have already seen the effects.Mayo estimates up to $3 billion in revenue losses from the onset of the pandemic until late April — given the system is operating “well below” normal capacity. It also announced employee furloughs and pay cuts, as several other hospitals have done.
Data released Tuesday from health cost nonprofit FAIR Healthshow how steep declines have been for larger hospitals in particular. The report looked at process claims for private insurance plans submitted by more than 60 payers for both nonprofit and for-profit hospitals.
Facilities with more than 250 beds saw average per-facility revenues based on estimated in-network amounts decline from $4.5 million in the first quarter of 2019 to $4.2 million in the first quarter of 2020. The gap was less pronounced in hospitals with 101 to 250 beds and not evident at all in those with 100 beds or fewer.
Funding from federal relief packages has helped offset losses at those larger hospitals to some degree.
Analysts from the ratings agency said those grants could help fill in around 30% to 50% of lost revenues, but won’t solve the issue on their own.
They also warned another surge of COVID-19 cases could happen as hospitals attempt to recover from the steep losses they felt during the first half of the year.
Anthony Fauci, the nation’s top infectious disease expert, warned lawmakers this week that the U.S. doesn’t have the necessary testing and surveillance infrastructure in place to prep for a fall resurgence of the coronavirus, a second wave that’s “entirely conceivable and possible.”
“If some areas, cities, states or what have you, jump over these various checkpoints and prematurely open up … we will start to see little spikes that may turn into outbreaks,” he told a Senate panel.
That could again overwhelm the healthcare system and financially devastate some on the way to recovery.
“Another extended time period without elective procedures would be very difficult for the sector to absorb,” Holloran said, suggesting if another wave occurs, such procedures should be evaluated on a case-by-case basis, not a state-by-state basis.
Hospitals in certain states and markets are better positioned to return to somewhat normal volumes later this year, analysts said, such as those with high growth and other wealth or income indicators. College towns and state capitols will fare best, they said.
Early reports of patients rescheduling postponed elective procedures provide some hope for returning to normal volumes.
“Initial expectations in reopened states have been a bit more positive than expected due to pent up demand,” Holloran said. But he cautioned there’s still a “real, honest fear about returning to a hospital.”
Moody’s Investors Service said this week nonprofit hospitals should expect the see the financial effects of the pandemic into next year and assistance from the federal government is unlikely to fully compensate them.
How quickly facilities are able to ramp up elective procedures will depend on geography, access to rapid testing, supply chains and patient fears about returning to a hospital, among other factors, the ratings agency said.
“There is considerable uncertainty regarding the willingness of patients — especially older patients and those considered high risk — to return to the health system for elective services,” according to the report. “Testing could also play an important role in establishing trust that it is safe to seek medical care, especially for nonemergency and elective services, before a vaccine is widely available.”
Hospitals have avoided major cash flow difficulties thanks to financial aid from the federal government, but will begin to face those issues as they repay Medicare advances. And the overall U.S. economy will be a key factor for hospitals as well, as job losses weaken the payer mix and drive down patient volumes and increase bad debt, Moody’s said.
Like other businesses, hospitals will have to adapt new safety protocols that will further strain resources and slow productivity, according to the report.
Another trend brought by the pandemic is a drop in ER volumes. Patients are still going to emergency rooms, FAIR Health data show, but most often for respiratory illnesses. Admissions for pelvic pain and head injuries, among others declined in March.
“Hospitals may also be losing revenue from a widespread decrease in the number of patients visiting emergency rooms for non-COVID-19 care,” according to the report. “Many patients who would have otherwise gone to the ER have stayed away, presumably out of fear of catching COVID-19.”
Despite rebounding patient volumes at some health systems, an overall slow and bumpy recovery period is most likely to last into next year, according to analysts with S&P Global Ratings. Operating margins will remain below historic levels for the rest of 2020 and into early 2021.
The ratings agency took negative action against companies in health sub-sectors facing more sudden and dramatic declines in business and now face less certain paths to recovery than others, such as dental companies, along with physical therapy and ambulatory surgery centers.
Medical staffing and physician groups were also downgraded or had their outlooks revised, due to major declines in emergency room and doctors office visits coupled with declining demand for anesthesia and radiology services related to delayed surgeries.
Dive Insight:
Federal relief grants are helping offset major financial losses for some health systems in the short-term, but factors like a second surge causing another total lockdown, rising unemployment and hesitancy from patients as they return to medical settings make long-term prospects unpredictable.
S&P Global Ratings said in a report this week that it took 36 negative actions in health services companies during the pandemic. The most affected sub-sector was dental companies. It also changed outlooks on ambulatory surgery centers given significant volume declines.
Hospitals and home healthcare were rated at moderate to high financial risk, though analysts expect those businesses to recover faster due to the more essential nature of their services, according to the report. And in the short-term, government relief funds will help bolster hospitals’ liquidity as they attempt to return to normal operations and recover from steep losses.
Delayed elective care that’s just restarting in some states led most hospitals to the financial fallout. But even hospitals treating a large number of COVID-19 patients will be hurt, as these patients are expensive to treat due to higher supply and labor costs, the report said.
It also found that nonprofit and for-profit operators could fare differently in their financial recoveries. Non-profit hospitals generally have larger cash reserves than for profit systems, which rely instead almost exclusively on cash flow and borrowings for liquidity.
Providers are relying specifically on the Coronavirus Aid, Relief and Economic Security Act which allocated $100 billion for providers that they don’t have to pay back, though there has been some criticism about how the money was distributed and whether it advantages some providers over others.
A Kaiser Family Foundation report found that CARES funding tends to favor for profit, higher margin hospitals with a higher mix of private payer revenue compared to those that rely on government payers such as Medicare and Medicaid.
Other legislation to help financially struggling health systems include advanced Medicare payments in the form of loans that must be paid back roughly four months after they are received.
The U.S. House of Representatives also passed a $3 trillion bill dubbed the Health and Economic Recovery Omnibus Emergency Solutions (HEROES) Act that allocates $100 billion for provider reimbursement and creates special enrollment periods for Medicare and Affordable Care Act plans, though the Trump administration said it’s too soon for additional relief funding.
Lab companies were put in the moderate risk category, and seeing a “40% decline in lab tests net of COVID testing,” S&P said.
Still, it said despite the drop in overall testing for LabCorp and Quest Diagnostics, S&P predicted “their services to become even more important, and for their services to recover reasonably well as testing related to the pandemic continues to grow and as medical procedures and physician visits ramp-up through the rest of the year and into 2021.”
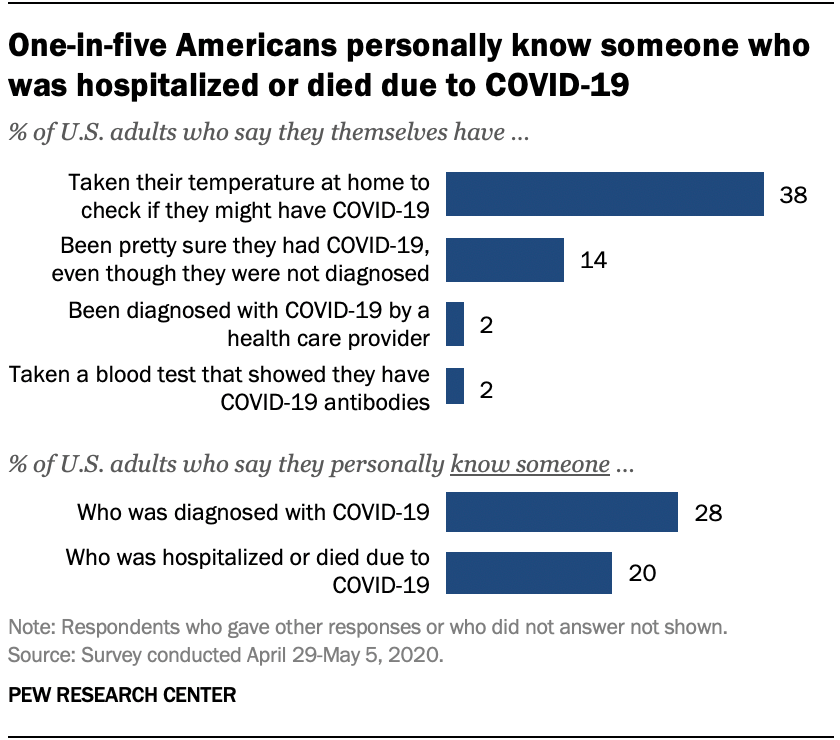
Relatively few Americans say they have been diagnosed with COVID-19 or tested positive for coronavirus antibodies, but many more believe they may have been infected or say they personally know someone who has been diagnosed.
Only 2% of U.S. adults say they have been officially diagnosed with COVID-19 by a health care provider, according to a new Pew Research Center survey. And 2% say they have taken a blood test that showed they have COVID-19 antibodies, an indication that they previously had the coronavirus. But many more Americans (14%) say they are “pretty sure” they had COVID-19, despite not getting an official diagnosis. And nearly four-in-ten (38%) say they’ve taken their temperature to check if they might have the disease.
Although few Americans have been diagnosed with COVID-19 themselves, many more say they know someone with a positive diagnosis. More than one-in-four U.S. adults (28%) say they personally know someone who has been diagnosed by a health care provider as having COVID-19. A smaller share of Americans (20%) say they know someone who has been hospitalized or who has died as a result of having the coronavirus.
Some groups are more likely than others to report personal experiences with COVID-19. For instance, black adults are the most likely to personally know someone who has been hospitalized or died as a result of the disease. One-third of black Americans (34%) know someone who has been hospitalized or died, compared with 19% of Hispanics and 18% of white adults. Black Americans (32%) are also slightly more likely than Hispanic adults (26%) to know someone diagnosed with COVID-19. Public health studies have found black Americans are disproportionately dying or requiring hospitalization as a result of the coronavirus.
Areas in the northeastern United States have recorded some of the highest rates of coronavirus cases and fatalities, and this is reflected in the Center’s survey. About four-in-ten adults living in the Northeast (42%) say they personally know someone diagnosed with COVID-19, significantly more than among adults living in any other region. People living in the Northeast (31%) are also the most likely to know someone who has been hospitalized or died as a result of the disease.
One aspect of personal risk for exposure to the coronavirus is whether someone is employed in a setting where they must have frequent contact with other people, such as at a grocery store, hospital or construction site. Given the potential for the spread of the coronavirus within households, risk to individuals is also higher if other members of the household are employed in similar settings. Among people who are currently employed full-time, 35% are working in a job with frequent public contact. Among those working part-time, almost half work (48%) in such a setting. For those living in a household with other adults, 35% report that at least one of those individuals is working in a job that requires frequent contact with other people.
Taken together, nearly four-in-ten Americans (38%) have this type of exposure – either currently working in a job that requires contact with others, living in a household with others whose jobs require contact, or both.
Hispanics (at 48%) are more likely than either blacks (38%) or whites (35%) to have this type of personal or household exposure. An earlier Center analysis of government data found Hispanic adults were slightly more likely to work in service-sector jobs that require customer interaction, and that are at higher risk of layoffs as a result of the virus. In fact, the current Center survey found Hispanics were among the most likely to have experienced pay cuts or job losses due to the coronavirus outbreak.
Interpersonal exposure in the workplace is also more widespread among younger adults. And there is a 10 percentage point difference between upper- and lower-income Americans in exposure, with lower-income adults more likely to work in situations where they have to interact with the public, or to live with people who do.
Health experts warn that COVID-19 is particularly dangerous to people who have underlying medical conditions. In the survey, one-third of adults say they have such a condition. Among this group, nearly six-in-ten (58%) say that the coronavirus outbreak is a major threat to their personal health. Among those who do not report having an underlying medical condition, just 28% see the outbreak as a major threat to their health. Americans who have an underlying health condition are also more likely than those who do not to say they’ve taken their temperature to check if they might have COVID-19 (47% vs. 33% of those without a health condition).
Self-reports of an underlying health condition vary greatly by age. Among those ages 18 to 29, just 16% say they have a condition; this rises steadily with age to 56% among those 65 and older. Whites are a little more likely than blacks and Hispanics to report having a health condition, but both blacks (at 54%) and Hispanics (52%) are far more likely than whites (32%) to say that the coronavirus outbreak is “a major threat” to their health.
Seconds Count Survey Highlights New research shows fear of COVID-19 is stopping people from seeking care during medical emergencies, like heart attacks or strokes.
As States start to re-open, more than one-third of Americans (36 percent) consider going to the hospital to be one of the riskiest behaviors to take part in compared to going to a hair salon (27 percent) or going to the beach (16 percent)
61 percent of respondents think they are either somewhat likely or very likely to acquire COVID-19 in a hospital
Half of respondents are more afraid of contracting COVID-19 than experiencing a heart attack or stroke
Nearly 60 percent of respondents are more afraid of a family member or loved one contracting COVID-19 than experiencing a heart attack or stroke
When asked which are you more afraid of, contracting COVID-19, experiencing a heart attack or experiencing a stroke – twice as many people over the age of 60 are more afraid of contracting COVID-19 (52 percent) than they are of experiencing a heart attack (23 percent) or stroke (25 percent)
Months into the pandemic, the U.S. faces an ongoing shortage of PPE and some of it is still subject to tariffs.
Gojo Industries, which makes Purell, builds automated hand sanitizer dispensers in the U.S. The devices rely on an electronic input made in China. But in early March, the U.S. Trade Representative (USTR) turned down Gojo’s tariff exemption request for the specific part needed for its dispensers, just before President Donald Trump declared a national emergency due to COVID-19.
The government later reversed its decision and waived the tariff after a senator from Ohio, where Gojo Industries is based, pressured the USTR because of the product’s importance to public health.
But several months into the COVID-19 pandemic, many consumers still struggle to find public-health-related products, from hand sanitizer to wipes. There’s also a shortage of personal protective equiptment (PPE) in the United States, and some of it is still subject to tariffs, throwing a wrench into pandemic preparedness and response.
Health supply chain experts sound the warning bell
The healthcare industry warned the Trump administration long before COVID-19 that imposing tariffs on Chinese-produced essential healthcare products put the nation’s public health preparedness at risk.
In August 2018, Matt Rowan, president of the Health Industry Distributors Association (HIDA) told the U.S. Trade Representative (USTR) 301 Committee that products on the proposed list were widely used in healthcare settings and “are a critical component of our nation’s response to public health emergencies, such as Ebola.”
Tariffs on items like masks, medical gloves, isolation gowns and wet wipes would not only increase U.S. healthcare costs, but impact government and commercial suppliers supporting patients and providers during a medical crisis, the industry warned.
“We did not make up for the lack of imports from China by more imports from the rest of the world.”
Jennifer Hillman
Senior fellow for trade and international political economy, Council on Foreign Relations
Disrupting this supply chain would erode the industry’s ability to deliver quality outcomes, and “placing tariffs on these products would lead to product shortages and further exacerbate public health challenges during times of crisis. It would significantly limit the ability of all levels of government, as well as the commercial healthcare supply chain, to adequately support response efforts during emergency events,” Rowan said.
In spite of healthcare industry testimony, the U.S. slapped 15% to 25% tariffs on many of these essential healthcare items. That included 25% Section 301 tariffs on items like disposable medical headwear, hand sanitizers and pulse oximeters. It included 15% Section 301 tariffs on medical protective clothing, protective goggles, and Nitrile and sterile gloves.
In 2018, the American Action Forum estimated if import numbers remained consistent, medical supply costs would rise by $400 million.
“A good portion of the reason why we are in such a difficult position is imports of those products went way down once those tariffs were imposed on China,” Jennifer Hillman, senior fellow for trade and international political economy at the Council on Foreign Relations, told reporters on a press call. “Our traditional stockpiles, the amount that we had just in storage, by FEMA, by Veterans Affairs, by HHS, and by a lot of state and local hospitals, they decreased the amount of their imports and decreased their stockpiles because of the tariffs.”
Shefali Kapadia / Supply Chain Dive, data from World Trade Organization
In placing the tariffs, one Trump administration goal was for buyers to procure items from other countries or manufacture in the U.S. instead. And that happened, but not to the extent necessary to maintain the stockpiles.
“We did not make up for the lack of imports from China by more imports from the rest of the world,” Hillman said. China was the largest exporter of medical face masks globally, accounting for 25% of the world’s supply in 2019, according to the World Trade Organization (WTO).
The U.S. was the largest medical products importer during the last three years, with 19% of total world imports of these products in 2019, according to the WTO. Personal protective products (including face masks, hand sanitizer and protective eyewear) made up 10% of U.S. medical imports. Worldwide trade of products labeled “critical” and in severe shortage during the pandemic, included 1.7% of the total world trade for 2019, totaling $597 billion. The U.S. imported $5.2 billion in medical equipment in 2019.
The time-consuming exemption process
Trump refused a blanket exemption for medical products when COVID-19 hit, but did grant some exemptions retroactively to Sept. 1, 2019, through Sept. 1, 2020, on supplies like sterile drapes, disposable gowns, some face masks and disposable shoe covers. The government granted exemptions in executive orders on March 10, March 16 and March 17.
“They issued over 200 exclusions from the tariffs, with more than a hundred of these items are the ones that were needed for medical devices and to fight COVID,” said Hillman.
Still, $1.1 billion worth of healthcare imports that could be used for treating COVID-19 remain subject to the 25% tariffs, according to a report by Chad P. Brown, senior fellow at the Peterson Institute for International Economics. Tariffs from another $3.3 billion of critical healthcare product imports were lowered from 15% to 7.5%.
General Motors (GM), partnering with Ventec to produce ventilators under the Defense Production Act, needed to source more than 700 components for the new machines. While GM could obtain most from North America, it sourced components from a handful of categories from China, which fell under a 25% tariff. They included grommets, filter parts, compressor silencers and a power cord set. GM requested exclusions from the USTR for individual parts.
GM is producing ventilators in response to the pandemic. The company needed to source more than 700 component parts for the ventilators, many of which come from China and face 25% tariffs.
AJ Mast for General Motors
These types of requests are time-consuming, especially when efforts might be better spent on other priorities during this crisis, according to legislators. Senators on both sides of the aisle pointed this out in an April letter to U.S. Trade Representative Robert Lighthizer, saying “[companies] should not be subjected to the lengthy process of submitting tariff exemption requests for each individual input required to make products essential for addressing the ongoing pandemic.”
Tethered to China
Procuring from outside of China can alleviate the risk of single sourcing and increased costs from tariffs, but it’s not always possible due to availability of raw materials, FDA clearance or production capabilities,
In June 2019, Lara Simmons, Group President of Medline Industries, explained to the USTR why a manufacturer wasn’t easily able to source many of its healthcare products, like gloves, outside of China. She said 97% of vinyl gloves come from China.
“These products are not made in the United States and some of these products are effectively available only from China. Starting production in the U.S. or any third country would be a time-consuming expensive process due to the FDA regulatory procedure that is required for these products,” she said.
The process for FDA regulated Class I and Class II medical devices can take more than two years, she said, and includes development and installation of environmental controls, facility upgrades, equipment purchase, installation, process validation and multiple rounds of audits to ensure regulatory compliance and verification of the quality system effectiveness.
Personal protective products include face masks, hand soap, sanitizer and protective spectacles.
Shefali Kapadia / Supply Chain Dive, data from World Trade Organization
Even gloves used for hospital cleaning and industrial food prep are in short supply, sending buyers back to China in spite of high tariffs.
Minnesota-based Global Glove & Safety Manufacturing applied for a tariff exemption for unsupported gloves (rubber gloves without a fabric lining), which are subject to a 25% tariff. The company’s clients that traditionally use disposable supported gloves can’t keep those in stock and are now using unsupported gloves.
“Once stability is achieved in the marketplace, we won’t buy from China for unsupported gloves, especially because of the tariffs.”
Tanner Brehmer
Product development manager, Global Glove & Safety Manufacturing
Global Glove typically buys from producers in countries including Malaysia, Sri Lanka and Thailand, but due to lockdowns and limited production in those countries, it’s trying to source some from China. “It’s tough because nothing is really shipping and lead times are pushed out so far. We don’t know when we’ll get it from other countries,” Tanner Brehmer, the company’s product development manager, told Supply Chain Dive.
The 25% tariff on the gloves produced in China greatly increases the cost, yet China is one of the only countries producing these products at full speed, he said. So in spite of tariffs, his company may move some procurement back to China. “Once stability is achieved in the marketplace, we won’t buy from China for unsupported gloves, especially because of the tariffs,” Brehmer said.
A diversified future?
Lighthizer and the Trump administration has a long-term vision for the tariffs. “Indeed, if there is one lesson to be drawn from this crisis, it is that dependence on other countries as the source of key medical products has created a strategic vulnerability for the U.S. By encouraging diversification of supply chains and—better yet—more manufacturing in the U.S., President Trump’s economic and trade policies are helping to overcome that vulnerability,” Lighthizer wrote in the The Wall Street Journal.
As healthcare systems sourced PPE and other supplies to treat COVID-19, they often paid the tariffs if needed, even if that meant paying more for the products. Healthcare systems and the government also purchased from manufacturing companies converting their domestic factories to produce needed items for COVID-19 treatment.
“We need a more resilient supply chain, which means we need to have multiple sources of supply.”
Jennifer Hillman
Senior fellow for trade and international political economy, Council on Foreign Relations
Which of these production lines will continue when the acute need for PPE is over, is hard to know. However, healthcare systems are now more aware of the risk in relying on foreign sources for their supplies.
“We need a more resilient supply chain, which means we need to have multiple sources of supply rather than sole sources of supply, and we need to do a better job of creating stockpiles,” said Hillman. “Part of the reason why we’re in such a world of hurt is because of our stockpiles were allowed to be depleted, again, in response to these tariffs.”
Ascension reported a total loss of $2.7 billion in the first three months of 2020, compared to income of $1.2 billion during the same time last year, according to new financial statements from the nonprofit giant.
The Catholic system, one of the largest hospital operators in the country, saw operating revenue decrease 2.5% year over year in the period ending March 31 to $6.1 billion. That came as expenses like salaries and supplies ticked up by more than 3% to $6.4 billion.
Ascension also reported losses from investments of $2.48 billion, compared to return from investments of $1.1 billion from the same time last year. Nonprofit operators are reporting massive investment hits as the stock market slid in the beginning of the year following widespread business closures and shelter-in-place orders stifling the economy.
Dive Insight:
Nonprofit hospitals are posting huge losses for the outset of 2020 as analysts predict an even grimmer second quarter to come. However, though losses in the first three months of the year dragged St. Louis-based Ascension into the red, the provider behemoth is still in a relatively good position to weather the pandemic, with current assets of $38.3 billion and 231 days of cash on hand.
Though patient volume was up prior to the pandemic, revenue from providing medical care flagged in the three-month period, as inpatient and ambulatory care slowed as the coronavirus surfaced in the U.S. In mid-March, Ascension deferred all non-essential procedures as stay-at-home orders kept potential patients in the home, impacting the system’s volumes.
Total net patient service revenue was $5.7 billion, down 3% year over year. Net patient service revenues had the sharpest drop off in March, decreasing more than 15% in that month alone.
“COVID-19 has been encountered across all Ascension markets, to varying degrees, and has had an adverse effect,” Ascension management wrote in comments on the results.
The system, which operates more than 2,600 sites of care, including 150 hospitals across 20 states and the District of Columbia, has received federal help to make up for lower-than-expected revenue. Ascension said in the filing it has received Coronavirus Aid, Relief and Economic Security Act funding before March 31. Though a spokesperson declined to tell Healthcare Dive a specific figure, Ascension has received at least $211 million from HHS, according to a New York Times review of the grants finding large hospitals with deep pockets are receiving the lion’s share of congressional funds.
Smaller hospitals that serve more vulnerable populations were deeply critical of HHS’ initial method to distribute the CARES funds, which put high margin hospitals at an advantage. The department did not take into account hospitals’ existing financial resources in distributing the pot.
Nine-year-old Ascension also received just under $2 billion in accelerated loans from the Medicare program.
Normal increases in operations compounded the negative effect of the pandemic, Ascension said. The system was funneling money into expanding service lines and sites of care and standardizing revenue cycle services prior to the COVID-19 crisis, which sharply increased expenses.
Supplies expenses particularly jumped in March by almost 7%, as the system hustled to procure needed equipment at unexpected rates to prepare for an anticipated surge in COVID-19 patients.