Dive Brief:
- Most states with budget projections expect Medicaid shortfalls due to rising spending as more people lose jobs and enroll into the safety net insurance for low-income Americans due to the COVID-19 pandemic, according to a new Kaiser Family Foundation survey.
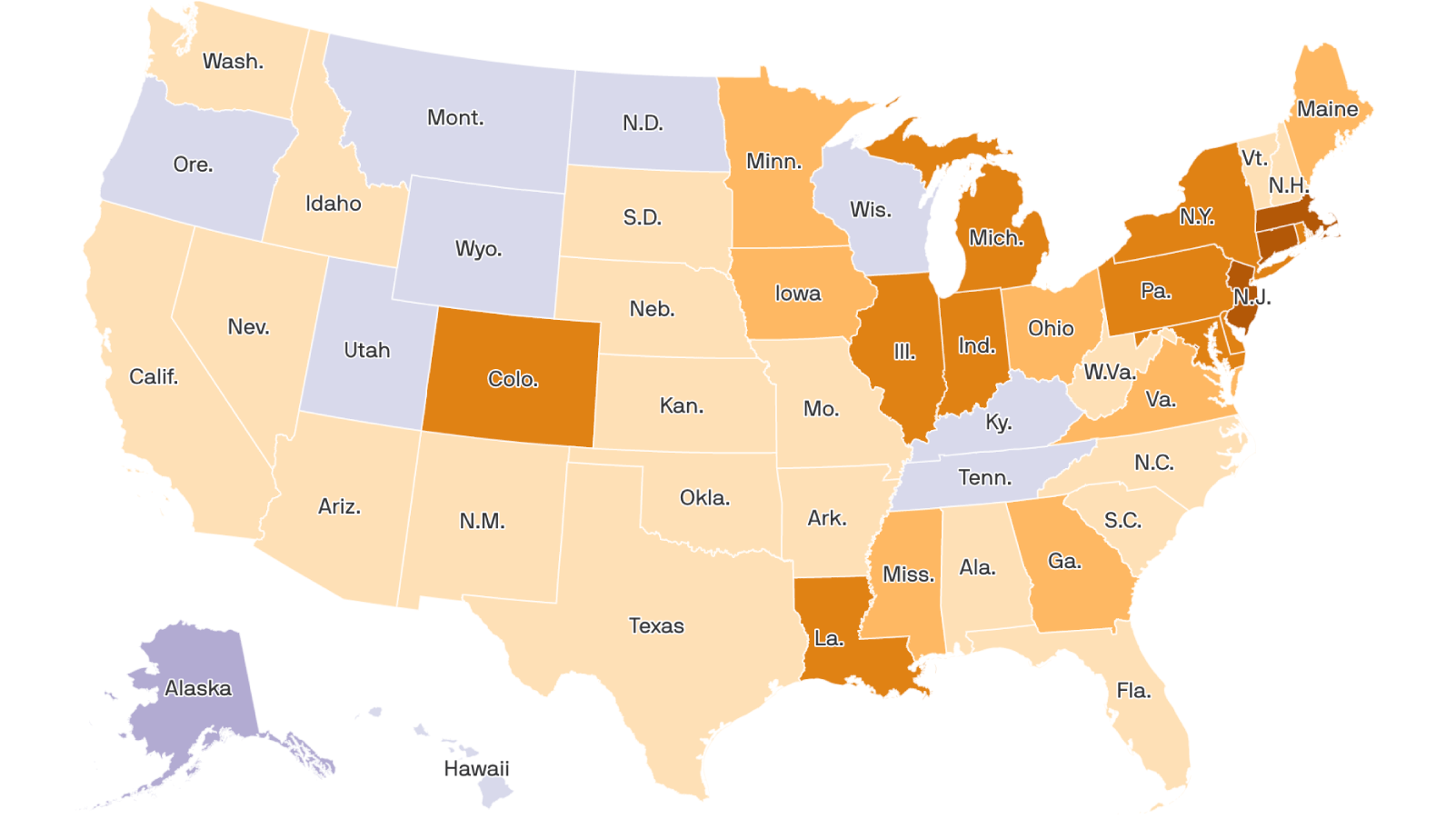
- Almost all states with enrollment projections and more than half with spending projections expect program growth to surpass pre-pandemic estimates. Nearly all states anticipate growth will accelerate even more in the 2021 fiscal year, KFF found. As a result of that growth, 17 of 19 states with budget projections report a shortfall is “nearly certain” or “likely” for the upcoming fiscal year.
- The survey comes as Congress once again considers raising the federal match rate for Medicaid in the $3 trillion Health and Economic Recovery Omnibus Emergency Solutions Act, passed by the House of Representatives on Friday.
Dive Insight:
Medicaid is often the top line spending item in state budgets, sending states scrambling for ways to reduce spend in the safety net health insurance program, including controversial block grants for funding.
At the start of the 2020 fiscal year, states anticipated modest Medicaid spending growth, and flat enrollment growth due to the strong economy. That forecast quickly shifted as the coronavirus spread in the U.S., which lost some 21 million jobs in April as businesses shutter their doors in compliance with stay-at-home orders, sending the unemployment rate to 15%.
Because the U.S. generally couples coverage to employment, skyrocketing job loss could make an estimated 17 million people newly eligible for Medicaid and 6 million eligible for subsidies in the Affordable Care Act marketplaces by January 2021.
Medicaid officials from 38 states shared their budget projections with KFF for the survey. States that did not respond were still gathering data about the coronavirus or didn’t have updated enrollment or spending projections for the 2020 or 2021 fiscal years, KFF researchers Robin Rudowitz and Elizabeth Hinton said.
Thirty-two of 34 states with enrollment projections think enrollment will exceed initial projections in 2020, and 30 of 31 states anticipate that growth in 2021 will outpace the current fiscal year.
States are more mixed on spending projections. Over half of states with projections, 18 of 32, expect 2020 Medicaid spending to exceed pre-pandemic estimates. Eight states anticipate no change, and the remaining six project slightly lowered spending due to lower healthcare utilization as non-essential services have largely ground to a halt.
State Medicaid officials are more in lockstep when it comes to 2021 spending projections. Nearly all states with projections — 29 of 30 — think Medicaid spending rates in 2021 will increase over 2020.
Without greater support from the federal government, the survey hints states will face significant spending cuts for Medicaid for the upcoming fiscal year, which begins July 1 for most states. Multiple groups, including the National Governors Association and the National Association of State Medicaid Directors, have called for a higher federal match rate.
One of the first legislative packages designed to mitigate the fallout of COVID-19, the Families First Coronavirus Response Act passed March 18, authorized a 6.2 percentage point increase in the rate for Medicaid if states meet certain requirements. States can’t increase premiums or restrict eligibility standards and must cover COVID-19 testing and treatment without cost-sharing.
The HEROES Act passed by Democrats in the House on Friday would increase the match rate by 14 percentage points from July 1, 2020, through June 30, 2021, along with benchmarking an additional $100 billion for providers.
However, Senate Majority Leader Mitch McConnell, R-Ky., and President Donald Trump have said they’re in no rush to pass another round of legislation adding to the more than $3 trillion Congress has approved so far.