Dr. Christine Choi, 32, a medical resident at Harbor-UCLA Medical Center in Torrance, prepares to enter an isolation area for COVID-19 inpatients. Health care providers must face daily patient death and suffering.
Soon after the COVID-19 pandemic began last spring, Christine Choi, DO, a second-year medical resident at Harbor-UCLA Medical Center, volunteered to enter COVID-19 patient rooms. Since then, she has worked countless nights in the intensive care unit in full protective gear, often tasked with giving the sickest patients and their families the grim choice between intubation or near-certain death.
“I’m offering this guy two terrible options, and that’s how I feel about work: I can’t fix this for you and it sucks, and I’m sorry that the choices I’m giving you are both terrible,” Choi told the Los Angeles Times’ Soumya Karlamangla about one patient encounter.
While Choi exhibits an “almost startlingly positive attitude” in her work, it’s no match for the psychological burdens placed on her shoulders by the global pandemic, Karlamangla wrote. When an older female COVID-19 patient died in the hospital recently, her husband — in the same hospital with the same diagnosis — soon began struggling to breathe. Sensing that he had little time left, Choi held a mobile phone at his bedside so that each of his children could come on screen to tell him they loved him. “I was just bawling in my [personal protective equipment],” Choi said. “The sound of the family members crying — I probably will never forget that,” she said.
It was not the first time the young doctor helped family members say goodbye to a loved one, and it would not be the last. Health care providers like Choi have had to work through unimaginable tragedies and unprecedented circumstances because of COVID-19, with little time to dedicate to their own mental health or well-being.
It has been nearly a year since the US reported what was believed at the time to be its first coronavirus death in Washington State. Since then, the pandemic death toll has mushroomed to nearly 500,000 nationwide, including 49,000 Californians. These numbers are shocking, and yet they do not capture the immeasurable emotional weight that falls on the health care providers with the most intimate view of COVID-19’s deadly progression.“The horror of the pandemic has unfolded largely outside public view and inside hospitals, piling a disproportionate share of the trauma on the people whose work takes them inside their walls,” Karlamangla wrote.
Experts are deeply concerned about the psychological and physical burdens that providers must bear, and the fact that there is still no end in sight. “At least with a natural disaster, it happens, people get scattered all over the place, property gets damaged or flooded, but then we begin to rebuild,” Lawrence Palinkas, PhD, MA, a medical anthropologist at USC, told Karlamangla. “We’re not there yet, and we don’t know when that will actually occur.”
Sixty-eight percent of providers said they feel emotionally drained from their work, 59% feel burned out, 57% feel overworked, and 50% feel frustrated. The poll asked providers who say they feel burned out what contributes most to that viewpoint. One doctor from the Central Valley wrote:
“Short staffed due to people out with COVID. I’m seeing three times as many patients, with no time to chart or catch up. Little appreciation or contact from my bosses. I have never had an N95 [mask]. The emotional toll this pandemic is taking. Being sick myself and spreading it to my wife and young kids. Still not fully recovered but needing to be at work due to physician shortages. Lack of professional growth, and a sense of lack of appreciation at work and feeling overworked. The sadness of the COVID-related deaths and the stories that go along with the disease. That’s a lot of stuff to unpack.”
The pandemic has been especially challenging for female health providers, who compose 77% of health care workers with direct patient contact. “The pandemic exacerbated gender inequities in formal and informal work, and in the distribution of home responsibilities, and increased the risk of unemployment and domestic violence,” an international group of experts wrote in the Lancet. “While trying to fulfill their professional responsibilities, women had to meet their families’ needs, including childcare, home schooling, care for older people, and home care.”
For one female doctor from the Bay Area who responded to the CHCF survey, the extra burdens of the pandemic have been unrelenting: “Having to work more, lack of safe, affordable, available childcare while I’m working. As a single mother, working 15 hours straight, then having to care for my daughter when I get home. Just exhausted with no days off. So many Zoom meetings all day long. Miss my family and friends.”
It is unclear how the pandemic will affect the health care workforce in the long term. For now, the damage “can be measured in part by a surge of early retirements and the desperation of community hospitals struggling to hire enough workers to keep their emergency rooms running,” Andrew Jacobs reported in the New York Times.
One of the early retirements Jacobs cited was Sheetal Khedkar Rao, MD, a 42-year-old internist in suburban Chicago. Last October, she decided to stop practicing medicineafter “the emotional burden and moral injury became too much to bear,” she said. Two of the main factors driving her decision were a 30% pay cut to compensate for the decline in revenue from primary care visits and the need to spend more time at home after her two preteen children switched to remote learning.
“Everyone says doctors are heroes and they put us on a pedestal, but we also have kids and aging parents to worry about,” Rao said.
Working Through Unremitting Sickness and Death
In addition to the psychological burden, health care providers must cope with a harsh physical toll. People of color account for most COVID-19 cases and deaths among health care workers, according to a KFF issue brief. Some studies show that health care workers of color “are more likely to report reuse of or inadequate access to [personal protective equipment] and to work in clinical settings with greater exposure to patients with COVID-19.”
“Lost on the Frontline,” a collaboration of Kaiser Health News and the Guardian, has counted more than 3,400 deaths among US health care workers from COVID-19. Eighty-six percent of the workers who died were under age 60, and nurses accounted for roughly one-third of the deaths.
“Lost on the Frontline” provides the most comprehensive picture available of health care worker deaths, because the US still lacks a uniform system to collect COVID-19 morbidity and mortality data among health care workers. A year into the project, the federal government has decided to take action. Officials at the US Department of Health and Human Services cited the project when asking the National Academies of Sciences, Engineering, and Medicine for a rapid expert consultation to understand the causes of deaths among health care workers during the pandemic.
The National Academies’ report, published December 10, recommends the “adoption and use of a uniform national framework for collecting, recording, and reporting mortality and morbidity data” along with the development of national reporting standards for a core set of morbidity impacts, including mental well-being and psychological effects related to working through public health crises. Some health care experts said the data gathering could be modeled on the federal government’s World Trade Center Health Program, which provides no-cost medical monitoring and treatment for workers who responded to the 9/11 terrorist attacks 20 years ago.
“We have a great obligation to people who put their lives on the line for the nation,” Victor J. Dzau, MD, president of the National Academy of Medicine, told Jacobs.
A view of the JHMR slopes and the village at the base of the mountain in Jackson, Wyoming.
Tucked in the shadow of the Tetons, the town of Jackson, Wy., and surrounding Teton County is home to less than 25,000 fulltime residents, but annually hosts over 2.5 million visitors. The valley’s natural beauty attracts an influx of tourists, who in turn are responsible for roughly 30% of the region’s jobs and over $1 billion in annual revenue, but this year, visitors came with an unwelcome price tag for locals: “Every time in this pandemic that we’ve had an influx of visitation, whether that’s second homeowners, or people just coming for a weekend, it follows with an uptick in cases and hospitalizations” says Dr. Jeff Greenbaum, medical director at the Emergency Department for St. John’s hospital and the Jackson Hole Mountain Ski Resort (JHMR) ski patrol.
With just one major hospital and eight emergency room physicians serving Teton County, any increase in COVID-19 cases is cause for concern. And in January, following the Christmas and New Year’s tourism rush, COVID-19 cases in Teton County skyrocketed to some of their highest levels since the pandemic began. Despite these developments, the ski resort, hotels, bars and restaurants remain open in the town. And Greenbaum remains optimistic that with the right strategies and precautions, the small hospital will not be overwhelmed by cases and skiing can stay open during the season for both visitors and locals. “The nightmare scenario is if the patients are stacking up in the emergency room and we don’t have enough personnel to treat them,” says Greenbaum. “But we’ll see that coming in advance, and we are not there yet.” The local hospital still has over 50% of its ICU beds unoccupied and has no COVID-19 patient on a ventilator. JHMR is similarly optimistic that it can stay open the entire season, trusting in the protocols it has put in place to protect both guests and staff.
Teton is the wealthiest county in the U.S., with a per capita income of over $250,000. At the start of the pandemic, a flurry of private jets landed at the Jackson Hole Airport, sometimes with a private ventilator in tow, as second homeowners and new buyers escaped to this rural paradise. Greenbaum posits that part of the reason why St. John’s hasn’t been overrun by cases is that many of the tourists that get COVID-19 in Teton County might not stay to get treatment in Teton County. At a time when millions of Americans are out of work, when daily infection rates are at an all-time high, and when thousands across the country are dying daily from the virus, should the wealthy indulge in an après ski, looking out onto the beautiful Teton mountains, all while potentially shuttling COVID-19 into and out of Jackson?
“This place is pretty much a gigantic country club, relying on second homeowners and tourism for its revenue,” says Jesse Bryant, a doctoral candidate in American Sociology at Yale University and creator of Yonder Lies, a podcast exploring the history of Jackson Hole. “But Jackson has to balance the ultra-wealthy with the real reality of people eking out a living here.” Teton County has the largest income gap of any county in the U.S., with the top 1% making almost 150 times more than the other 99%. From mountain guides to house cleaners to bartenders, much of the employment in Jackson cannot easily be transitioned to remote work, meaning that Jackson’s working class are among the most susceptible to unemployment from the pandemic. All across America the costs of the pandemic are being born by the poorest members of society; a Pew Research Center survey from September found that about 50% of low-income Americans say they or someone in their household has lost employment or had take a pay cut due to the pandemic, and similarly about 50% of low-income Americans reported having trouble paying their bills since the pandemic started.
During the spring and summer, the Coronavirus Aid, Relief, and Economic Security Act passed by the federal government at the start of the pandemic had provided $600 in additional unemployment payment per week, assuring many local and seasonal workers that their livelihoods were safe even if their jobs weren’t. But almost a year into the pandemic, Jackson’s working class are left with far fewer options: federal unemployment relief dropped to $300 and state unemployment benefits in Wyoming, although extended by 13 weeks, dry up after 39 weeks. “Many of the workers here don’t have a six-month buffer saved up,” said one restaurant worker who wished to remain anonymous for risk of losing their job, “so, while tourism presents a risk, we’re willing to take it to keep our paychecks coming in.”
This is the predicament that America has put herself in: a country with a limited safety net during the pandemic forces her workers to choose between the risk of getting sick, or losing their livelihoods. The mountain and the town are left trying to find a balance between keeping the economy open for tourists, and keeping COVID-19 out. As the second largest employer in Teton County, JHMR takes center stage in this unfolding drama. The resort is responsible for the livelihood of around 2,000 seasonal and local workers, and if the mountain were to shut down, many of the ancillary services in the town, like hotels, restaurants, rental shops, clothing stores and other retailers, would likely shutter their doors as well. In 2017, when the resort had to close for five days because of a power outage, the net economic impact to the local economy topped $5.5 million. “What’s happening in Jackson isn’t just a story of wealthy people coming into the rural west and getting the locals sick,” says Bryant. “This place has become more like a symbiotic relationship.”
One particularly vulnerable population is the Latino community, a significant number of which is undocumented, that lives in Jackson, and in the neighboring towns of Victor and Driggs. While it’s difficult to get exact numbers of their contribution to the economy, these workers keep Jackson running by filling jobs in all sectors, from house cleaners and construction workers to cooks and waiters.
“I’ve lived in Jackson for 25 years and used to go back to Mexico every winter because it was just too cold,” says Jorge, an undocumented construction worker in the town. “But then I got used to the cold and began skiing every single day.” Asked whether opening up the resort is worth the risk of bringing more COVID-19 into Jackson, Jorge says that by and large the Latino community welcomes the tourism with open arms, because it means job security. This lines up with findings from a survey undertaken by the Yale School of Environment this past summer, showing that Latino residents in the rural West had some of the highest rates of COVID-related unemployment in the country. “My wife and I work hard, her as a house cleaner, me in construction,” said Jorge. “The resort opening up and tourists coming to town is how many of us make our living.”
For its part, JHMR has been doing nearly everything within its power to keep COVID-19 from spreading on its slopes, iterating as the situation evolves to try to keep the 2021 season operating. In March of 2020, as the first wave of the pandemic was sweeping across the globe, the Wyoming State Health Officer shut down JHMR for the remainder of the season. The resort reopened in May, first for hikers and then mountain bikers—the summer tourists that in total are only about 10% the size of the winter tourist population. Before reopening for the summer crowd, it tested every single one of its staff members for COVID-19, and the resort’s human resources department transitioned into a contact-tracing team, coordinating with town officials whenever a case arose. While Wyoming didn’t issue a statewide mask mandate until Dec. 7, the resort instituted a mandatory mask policy during the summer. JHMR also learned to be more flexible in its operations: staff are now trained to perform a number of different functions, so they can sub in if there’s a shortage in a department, and shifts function as separate pods, meaning that if a person in one group has been exposed to COVID-19, another totally isolated pod can come in to take its place.
Over the summer and fall, tourists came in droves to Jackson, with as many as 40,000 total visitors in a day. According to the Jackson Hole Chamber of Commerce, both Yellowstone and Grand Teton National Parks—both within a quick drive from of Jackson—had about 50% more visitors in October of 2020 than they did for the same month in 2019. While many of the outdoor activities that bring people to Teton County during the summer—hiking, biking, climbing—have been deemed relatively safe during the pandemic, tourists also flocked indoors to the bars, restaurants and stores that remained open throughout most of the summer and fall. As a result, Teton County experienced large COVID-19 spikes in July and again at the end of October and into November.
Unsurprisingly, workers got sick. In response, Teton County’s Health Officer, Travis Riddell, sent out a series of recommendations pressing citizens to not gather with groups outside of their immediate family, avoid crowded indoor spaces and not congregate at trail heads, parks or other outside spaces. Still, most businesses stayed open as patrons kept coming. Riddell noted that the town had little choice: “Economic disasters are public health disasters,” Riddell said in an interview in July 2020 to National Geographic. “We know that when there are economic downturns, where there is an increase in poverty, an increase in uninsured numbers—that has direct health effects.”
Once JHMR opened for skiing the weekend after Thanksgiving, it was clear that demand for outdoor recreation would carry into winter; even with almost no international travel, JHMR expects demand during the 2021 winter months to be comparable to past years, at least. “If we just opened up [completely], the mountain would be packed, because demand itself is through the roof,” says LaMotte, “but we’ve imposed a maximum daily capacity for the mountain, to keep guests and staff safe.”
On a bluebird day near Christmas, the resort was sold out. It had snowed almost 15 inches the day before, and cars inched into the packed parking lot. Skiers and snowboarders waited in line for the lot shuttle bus, which, despite operating at 25% capacity, still felt uncomfortably full. The restaurants and bars looking out onto the sunny mountain were similarly capped at 25% capacity, and while masks and social distancing were required, patrons waiting for tables escaped the cold by standing shoulder to shoulder in the foyer.
At the resort, the socially distanced lines for the gondola were dangerously compressing. A resort worker cheerfully reminded guests from every corner of the U.S. to keep their distance and their masks above their noses. “We’re going to make it all the way through the season, without closing” yelled the worker, to cheers from the crowds. The lines moved slow—normally eight people fit onto the gondola, but under the new policies there was no mixing between groups, so often times the gondola ascends with just one or two passengers. At the top of the mountain, with views of the valley floor against the backdrop of the jagged Tetons, everyone breathed a bit easier.
Rob Kingwill and Emilé Zynobia, professional snowboarders based out of Jackson, stepped off the gondola into the cold Wyoming air, about 4,000 feet above the valley floor. Both sported COVID-19 masks made by Kingwill’s apparel company, Avalon 7. “I feel like this is almost an essential service, to give people the opportunity to be outside, said Kingwill. “We need this for our mental health.” When JHMR shut down in March of 2020, Kingwill strapped his snowboard to his backpack and hiked up Teton Pass’s infamous 1,300-foot Glory Boot Pack—every day for 77 days until all the snow had melted. But, he points out, most recreational skiers don’t have the knowledge and skills to navigate such technical terrain—and without the money those tourists bring in, Jackson’s working class would suffer. “It seems like the benefits outweigh the costs of keeping the resort open,” agreed Zynobia, as she and Kingwill strapped onto their boards. “Even though this is an activity skewed towards to wealthier people, it is helping a remote economy, and it is getting people outside at a time when we feel caged in.”
By the middle of January, Teton County’s COVID-19 cases were skyrocketing.Teton County currently has the highest caseload per capita of any county in the state of Wyoming and the highly contagious U.K. variant of COVID-19 was found to be circulating in the area. While the state of Wyoming had loosened COVID-19 gathering restrictions, the county reissued a series of guidelines on Jan. 25 that kept indoor gatherings capped at 25% and limited outdoor gatherings to 250 guests. At the resort, group ski lessons have been replaced by private lessons (at no extra cost), and the gondolas and lifts are ascending the mountain with minimal group mixing. Still JHMR can only control what happens on the mountain; “My main concern is not skiing itself,” says Greenbaum. “But rather I’m concerned about peripheral activity to skiing that lead people indoors, whether it’s a bar, a restaurant, a hotel lobby, a rental shop, a bus.”
Across the nation cases are surging, and other Colorado mountain towns like Telluride and Crested Butte have had similar spikes, likely due to an influx of winter tourism. The infection ratein Pitkin County, Colo., home to the Aspen and Snowmass ski resorts, was skyrocketing in the middle of January, with an incidence rate of about 3,500 per 100,000 people. In response, the county’s health department shut down all indoor dinning operations, but left the ski resorts open. The results were promising: in the past two weeks the COVID-19 rates for Pitkin County dropped by over 50%. “We’re on pace to be below 700 [cases per 100,000 people] in early February and I don’t think any of us thought that would happen so quickly,” said Josh Vance, the county’s epidemiologist, in an interview with the Aspen Times. “I’ll be honest—I think not having indoor dining plays a role.”
In Teton County, restaurants and bars remain open for indoor operations long as they follow social distancing guidelines. The reliance on the ultra-rich creates an undeniable risk to the livelihood of Jackson residents and workers. In the early days of the pandemic, ski resorts across Europe became super spreaders, with visitors transporting the virus like carry-on luggage, threatening other tourists and locals alike. As a result, resorts have been closed this winter across much of Europe, including in France, Germany and Italy. These precautions protect remote mountain towns from an influx of the virus, but there are other, massive costs associated with closing down. Without government support, there is little option for communities like Jackson but to stay open, follow existing public health guidelines and hope for the best. “When the pandemic first started coming to work felt like entering the lion’s den,” said the restaurant worker from Jackson who wished to remain anonymous. “But by now we’re all used to the risk, and really what choice do we have?”
Some teachers don’t want to return to the classroom until they’ve been vaccinated — setting up potential clashes with state and local governments pushing to reopen schools.
Why it matters:Extended virtual learning is taking a toll on kids, and the Biden administration is pushing to get them back in the classroom quickly. But that will only be feasible if teachers are on board.
Where it stands:Although the rise of new, more contagious variants has scrambled the calculus on school reopening, for now the expert consensus is that vaccinations aren’t essential to safely reopening schools.
A pair of studies from the CDC this week reiterated the agency’s stance that schools can operate safely with the proper precautions, along with other mitigation measures in the broader community.
Most states haven’t put teachers at the front of the line for vaccines. Only 18 have included teachers in the early priority groups that can get vaccinated now, and in all but four of those states, teachers are competing for shots with other higher-risk populations, including the elderly.
Yes, but: Teachers in some large school districts don’t want to return to the classroom without being vaccinated — which could mean several more months of virtual classes.
The Chicago teachers union has asked to delay reopening until teachers receive at least the first dose of the vaccine, but the city’s public health commissioner has said it could take months for teachers to be vaccinated, the Chicago Tribune reports.
“If you are required to work with students in person — which thousands of educators have been doing for months now — you should be vaccinated as soon as possible,” Jessica Tang, president of the Boston Teachers Union, said in statement after teachers were bumped behind the elderly in the state’s priority line, per Boston.com.
What they’re saying:“The issue is that we should be aligning vaccination with school opening. That doesn’t mean every single teacher has to be vaccinated before you open one school, it means there has to be that alignment,” Randi Weingarten, the president of the American Federation of Teachers, told ABC News.
Teachers should be eligible for vaccination by “late January,” she wrote in a USA Today op-ed over the weekend.
The other side: Ohio Gov. Mike DeWine has said school staff will be prioritized for vaccination, with the goal of having students return to classrooms by March 1.
But prioritizing teachers can be controversial. Oregon Gov. Kate Brown has been criticized for the decision to vaccinate teachers ahead of the elderly, high-risk essential workers and other vulnerable communities.
In a rural county in Georgia and at a private school in Philadelphia, teacher vaccine clinics were shut down by their state health departments, which said that educators were not yet eligible.
The bottom line:“It’s challenging to make those decisions about how to prioritize different populations, all of whom are at significant risk,” the Kaiser Family Foundation’s Jennifer Tolbert said.
Norma Leiva, a Food 4 Less warehouse manager, waits Saturday to be let into work in Panorama City, Calif. The state’s decision to expand vaccine eligibility to millions of older residents has stark consequences for communities of color disproportionately affected by the pandemic.
As a warehouse manager at a Food 4 Less in Los Angeles, Norma Leiva greets delivery drivers hauling in soda and chips and oversees staff stocking shelves and helping customers. At night, she returns to the home she shares with her elderly mother-in-law, praying the coronavirus isn’t traveling inside her.
A medical miracle at the end of last year seemed to answer her prayers: Leiva, 51, thought she was near the front of the line to receive a vaccine, right after medical workers and people in nursing homes. Now that California has expanded eligibility to millions of older residents — in a bid to accelerate the administration of the vaccines — she is mystified about when it will be her turn.
“The latest I’ve heard is that we’ve been pushed back. One day I hear June, another mid-February,” said Leiva, whose sister, also in the grocery business, was sickened last year with the virus, which has pummeled Los Angeles County — the first U.S. county to record 1 million cases. “I want the elderly to get it because I know they’re in need of it, but we also need to get it, because we’re out there serving them. If we’re not healthy, our community’s not healthy.”
Delaying vaccinations for front-line workers, especially food and grocery workers, has stark consequences for communities of color disproportionately affected by the pandemic. “In the job we do,” Leiva said, “we are mostly Blacks and Hispanics.”
Many states are trying to speed up a delayed and often chaotic rollout of coronavirus vaccines by adding people 65 and older to near the front of the line. But that approach is pushing others back in the queue, especially because retired residents are more likely to have the time and resources to pursue hard-to-get appointments. As a result, workers who often face the highest risk of exposure to the virus will be waiting longer to get protected, according to experts, union officials and workers.
The shifting priorities illuminate political and moral dilemmas fundamental to the mass vaccination campaign: whether inoculations should be aimed at rectifying racial disparities, whether the federal government can apply uniform standards and whether local decision-making will emphasize more than ease of administration.
Speed has become all the more critical with the emergence of highly transmissible variants of the virus. Only by performing 3 million vaccinations a day — more than double the current rate — can the country stay ahead of the rapid spread of new variants, according to modeling conducted by Paul Romer, a Nobel Prize-winning economist.
People with appointments wait in line to receive coronavirus vaccine in Los Angeles.
But low-wage workers without access to sick leave are among those most likely to catch and transmit new variants, said Richard Besser, president of the Robert Wood Johnson Foundation and former acting director of the Centers for Disease Control and Prevention. Because there are not enough doses of the vaccines to immunize front-line workers and everyone over 65, he said, officials should carefully weigh combating the pernicious effects of the virus on communities of color against the desire to expedite the rate of inoculation.
“If the obsession is over the number of people vaccinated,” Besser said, “we could end up vaccinating more people, while leaving those people at greatest risk exposed to ongoing rates of infection.”
The move to broaden vaccine availability to a wider swath of the elderly population — backed by Trump administration officials in their final days in office and members of President Biden’s health team — marks a departure from expert guidance set forth in December, as the vaccine rollout was getting underway.
A panel of experts advising the CDC recommended that the second priority group include front-line essential workers, along with adults 75 and older. The guidance represented a compromise between the desire to shield people most likely to catch and transmit the virus — because they cannot socially distance or work from home — and the effort to protect people most prone to serious complications and death.
People of color and immigrants are overrepresented not just in grocery jobs but also in meatpacking, public transit and corrections facilities, where outbreaks have taken a heavy toll. Black and Latino Americans are three to four timesmore likely than White people to be hospitalized and almost three times more likely to die of covid-19, the illness caused by the coronavirus, according to the CDC.
The desire to make vaccine administration equitable was central to recommendations from the Advisory Committee on Immunization Practices.
“We cannot abandon equity because it’s hard to measure and it’s hard to do,” Grace Lee, a committee member and a pediatrics professor at Stanford University’s School of Medicine, said at the time.
On Wednesday at a committee meeting, Lee said officials need both efficiency and equity to “ensure that we are accountable for how we’re delivering vaccine.”
“Absolutely agree we do not want any doses in freezers or wasted in any way,” Lee said.
But efficiency has won out in most places.
Some state leaders, such as Florida Gov. Ron DeSantis (R) and Texas Gov. Greg Abbott (R), acted on their own, lowering the age threshold to 65 soon after distribution began last year. Others followed with the blessing of top federal officials.
Biden’s advisers have said equity will be central to their efforts, calling access in underserved communities a “moral imperative” and promising, in a national vaccination strategy document, “we remain focused on building programs to meet the needs of hard-to-reach and high-risk populations.” In the meantime, they have similarly encouraged states to broaden vaccine availability to a larger segment of their older populations without providing guidance about how to ensure front-line workers remain a priority.
Experts studying health disparities say prioritizing people over 65 disproportionately favors White people, because people of color, especially Black men, tend to die younger, owing to racism’s effect on physical health. Twenty percent of White people are 65 or over, while just 9 percent of people of color are in that age group, according to federal figures.
“People are thinking about risk at an individual level as opposed to at a structural level. People are not understanding that where you work and where you live can actually bring more risks than your age,” said Camara Phyllis Jones, a family physician, epidemiologist and past president of the American Public Health Association. “It’s worse than I thought.”
The constantly changing priorities have made the uneven rollout all the more difficult to navigate. There is confusion over when, where and how to get shots, with different jurisdictions taking different approaches in an illustration of the nation’s decentralized public health system.
While praising the effort to expand access and speed up the administration of shots, Marc Perrone, president of the United Food and Commercial Workers International Union, said increasing reliance on age-based eligibility “must not come at the expense of the essential workers helping families put food on the table during this crisis.
“Public health officials must work with governors in all 50 states to end the delays and act swiftly to distribute the vaccine to grocery and meatpacking workers on the front lines, before even more get sick and die,” he said.
Mary Kay Henry, president of the Service Employees International Union, said the only way to ensure front-line workers get the vaccines they need is to involve them and their union representatives in decisions about eligibility and access. Unions, she said, could also be tapped to conduct outreach in hard-to-reach communities, including those not conversant in English.
“Essential workers who’ve been on the front lines both in health care but also across the service and care sectors — child care, airline, janitorial, security — face extraordinary risk,” she said.
Leiva, a 33-year member of UFCW Local 770, said the celebration of essential workers should come with recognition of their sacrifice, which is unevenly felt across racial groups. When the virus tore through the grocery store, she said, “every single one of them in that cluster was Hispanic.”
But with hospitals dangerously full in recent weeks, and less than half of distributed vaccine doses administered, many states broadened their top priority groups to include older adults, hoping to lessen the burden on hospitals and expedite vaccine administration.
Leiva is concerned about bringing the coronavirus into the home she shares with her elderly mother-in-law. She wants the elderly to receive the vaccine, “but we also need to get it, because we’re out there serving them. If we’re not healthy, our community’s not healthy.”
Protecting people 65 and older, officials say, saves the lives of those who face the gravest consequences and reduces the stress on intensive care units. Risk for severe covid-19 illness increases with age; 8 out of 10 deaths reported in the United States have been in people 65 and older.
Older people in the United States have also encountered enormous hurdles in gaining access to the vaccines. Faced with overloaded sign-up websites and jammed phone lines, they have sometimes spent nights waiting in line.
In more than half the states — at least 28, by one count — people 65 and older are in the top two priority groups, behind health-care workers and residents in long-term care facilities. As a result, front-line workers either fall behind the older group or are squeezed into the same pool, according to a Kaiser Family Foundation analysis.
“When you make that pool of eligible people much bigger, you’re creating much longer wait times for some of these groups,” said Jennifer Kates, a senior vice president at the foundation.
Front-line workers often labor in crowded conditions. Some live in multigenerational households. By contrast, many older adults are retired, have greater access to sign-up portals and have more time to wait in lines outside of clinics, health officials said.
People wait in line for coronavirus vaccine at a Sarasota, Fla., health department clinic.
“The 65-year-old person who is wealthier and can stay home and isn’t working and is retired and can ride it out for another two months … is less likely to get infected than the person who has to go outside every day for work,” said Roberto B. Vargas, assistant dean for health policy at Charles R. Drew University of Medicine and Science in Los Angeles.
In California, Gov. Gavin Newsom (D) announced Jan. 13 that the state was “significantly increasing our efforts to get these vaccines administered, get them out of freezers and get them into people’s arms” by increasing the number of people eligible to receive shots. “Everybody 65 and over — about 6.6 million Californians — we are now pulling into the tier to make available vaccines.”
On Jan. 25, Newsom said the state would move to an age-based eligibility system after vaccinating those now at the front of the line, including health-care workers, food and agriculture workers, teachers, emergency personnel and seniors 65 and older.
The abrupt changes confused local health officials.
Julie Vaishampayan, public health officer in San Joaquin Valley’s Stanislaus County, said the county had just finished vaccinating health-care workers and was getting ready to reach out to farm laborers at a tomato-packing company and food-processing workers. When the state added those 65 and older, the county had to pivot abruptly,as it faced a quintessential supply-and-demand dilemma.
“There isn’t enough vaccine to do it all, so how do we balance?” she said in an email. “This is really hard.”
In Tennessee, teachers were initially promised access but then were told to wait until people 70 and older got their shots. The state’s health commissioner, Lisa Piercey, said she was moving more gradually through the age gradations so as not to crowd out workers, treating the federal framework as guidance, which is often how officials have characterized it. “It’s not an either/or situation,” she said in an interview this month.
Keyona Simms puts a hat on Nylah Cooper, 2, at a day-care center in Baltimore. Day-care staff are considered essential workers in many states.
But with vaccine supply sharply limited, priorities had to be narrowed. By vaccinating older residents, she said, the state was also protecting its medical infrastructure by reducing the likelihood that older people, who are more likely to be hospitalized, would fall ill. Once there is more supply, she said, she would be able to amplify aspects of the state’s planning geared toward underserved and hard-to-reach populations. “I can’t wait to manifest that equity plan.”
In Nebraska, the health department in Douglas County, which includes Omaha, prioritized older residents over “critical industry workers who can’t work remotely” after the state expanded eligibility to residents 65 and older, according to a January news release. Meatpacking workers, grocery store employees, teachers and public transit workers were bumped lower in line.
Omaha’s teachers union had wanted its approximately 4,100 members to get shots before the district resumes full-time, in-person instruction for elementary and middle school students Tuesday. Now, they must wait until late spring, said Robert Miller, president of the Omaha Education Association.
“The fear, it goes hand in glove with going back to school five days a week,” he said, despite CDC reports that schools operating in person have seen scant transmission. “We’ve had some teachers who have multigenerational homes, who live in the basement, … and they can’t interact with their parents. We have some teachers who are staying at a different apartment away from their elder loved ones.”
Some state leaders sought to defend broadening eligibility to more of the elderly population, saying it was consistent with efforts to address racial disparities. Illinois had reduced the age requirement to 65, Gov. J.B. Pritzker (D) said recently, “in order to reduce covid-19 mortality and limit community spread in Black and Brown communities.” His office did not respond to a request for comment about how lowering the age threshold would have that effect.
In Massachusetts, state leaders announced Jan. 25 that people 65 and older and those with at least two high-risk medical conditions were next in line, ahead of educators and workers in transit, utility, food and agriculture, sanitation, and public works and public health.
That means Dorothy Williams, who runs a day-care center in a predominantly Black community where the infection rate is among the highest in Boston, has to wait. Her center stayed open throughout the pandemic, caring for children of essential workers, many of them in low-wage jobs in hospitals or nursing homes.
She recognizes the long hours and the exposure risks of those health-care aides. That means “we’re exposed,” she said, “each and every single day.” She has been able to keep the coronavirus at bay, but two weeks ago, she had a scare that forced her to close and get everyone tested after a child became ill. The tests came back negative, but the fear remains.
The annual J.P. Morgan Healthcare Conference is one of the best ways to diagnose the financial condition of the healthcare industry. Every January, every key stakeholder — providers, payers, pharmaceutical companies, tech companies, medical device and supply companies as well as bankers, venture capital and private equity firms — comes together in one exam room, even when it is virtual, for their annual check-up. But as we all know, this January is unlike any other as this past year has been unlike any other year.
You would have to go back to the banking crisis of 2008 to find a similar moment from an economic perspective. At the time, we were asking, “Are banks too big to fail?” The concern behind the question was that if they did fail, the economic chaos that would follow would lead to a collapse with the consumer ultimately picking up the tab. The rest is history.
Healthcare is “Too Vital to Fail”
2020 was historic in too many ways to count. But in a year when healthcare providers faced the worst financial crisis in the history of healthcare, the headline is that they are still standing. And what they proved is that in contrast to banks in 2008 that were seen by many as “too big to fail,” healthcare providers in 2020 proved that they were “too vital to fail.”
One of the many unique things about the COVID-19 pandemic is we are simultaneously experiencing a health crisis, where healthcare providers are the front line in the battle, and an economic crisis, felt in a big way in healthcare given the unique role hospitals play as the largest employer in most communities. Hospitals and health systems have done the vast majority of testing, treating, monitoring, counseling, educating and vaccinating all while searching for PPE and ventilators, and conducting clinical trials. And that’s just the beginning of the list.
Stop and think about that for a minute. What would we have done without them? Thinking through that question will give you some appreciation for the critical, challenging and central role that healthcare providers have had to play over the past year.
Simply stated, healthcare providers are the heart of healthcare, both clinically (essentially 100 percent of the care) and financially (over 50 percent of the $4 trillion annual spend on U.S. healthcare). Over the last year they stepped up and they stepped in at the moment where we needed them the most. This was despite the fact that, like most businesses, they were experiencing calamitous losses with no assurances of any assistance.
Healthcare is “Pandemic-Proof”
This was absolutely the worst-case scenario and the biggest test possible for our nation’s healthcare delivery system. Patient volume and therefore revenue dropped by over 50 percent when the panic of the pandemic was at its peak, driving over $60 billion in losses per month across hospitals and healthcare providers. At the same time, they were dramatically increasing their expenses with PPE, ventilators and additional staff. This was not heading in a good direction. While failure may not have been seen as an option, it was clearly a possibility.
The CARES Act clearly provided a temporary lifeline, providing funding for our nation’s hospitals to weather the storm. While there are more challenging times ahead, it is now clear that most are going to make it to the other side. The system of care in our country is often criticized, but when faced with perhaps the most challenging moment in the history of healthcare, our nation’s hospitals and health systems stepped up heroically and performed miraculously. The work of our healthcare providers on the front line and those who supported them was and is one thing that we all should be exceptionally proud of and thankful for.In 2020, they proved that not only is our nation’s healthcare system too vital to fail, but also that it is “pandemic proof.”
Listening to Front Line at the 2021 J.P. Morgan Healthcare Conference
There has never been a more important year to listen to the lessons from healthcare providers. They are and were the front line of our fight against COVID-19. If there was a class given about how to deal with a pandemic at an institutional level, this conference is where those lessons were being taught.
This year at the J.P. Morgan Healthcare Conference, CEOs, and CFOs from many of the most prestigious and most well-respected health systems in the world presented including AdventHealth, Advocate Aurora Health, Ascension, Baylor Scott & White Health, CommonSpirit Health, Henry Ford Health System, Intermountain Healthcare, Jefferson Health, Mass General Brigham, Northwell Health, OhioHealth, Prisma Health, ProMedica Health System, Providence, Spectrum Health and SSM Health.
I’ve been in healthcare for 30 years and this is my fifth year of writing up the summary of the non-profit provider track of the conference for Becker’s Healthcare to help share the wisdom of the crowd of provider organizations that share their stories. Clearly, this year was different and not because the presentations were virtual, but because they were inspirational.
What did we learn? The good news is that they have made many changes that have the potential to move healthcare in a much better direction and to get to a better place much faster. So, this year instead of providing you a nugget from each presentation, I am going to take a shot at summarizing what they collectively have in motion to stay vital after COVID.
10 Moves Healthcare Providers are Making to Stay Vital After-COVID
As a leader in healthcare, you will never have a bigger opportunity to drive change than right now. Smart leaders are framing this as essentially “before-COVID (BC)” and “after-COVID (AC)” and using this moment as their burning platform to drive change. Credit to the team at Providence for the acronym, but every CEO talked about this concept. As the saying goes, “never let a good crisis go to waste.” Well, we’ve certainly had a crisis, so here is a list of what the top health systems are doing to ensure that they don’t waste it and that they stay vital after-COVID:
1. Take Care of Your Team and They’ll Take Care of You: In a crisis, you can either come together as a team or fall apart. Clearly there has been a significant and stunning amount of pressure on healthcare providers. Many are fearing that mental health might be our nation’s next pandemic in the near future because they are seeing it right now with their own team. Perhaps one of their biggest lessons from this crisis has been the need to address the mental, physical and spiritual health of both team members as well as providers. They have put programs in place to help and have also built a tremendous amount of trust with their team by, in many cases, not laying off and/or furloughing employees. While they have made cuts in other areas such as benefits, this collective approach proved incredibly beneficial. And the last point here that relates to thinking differently about their team is that similar to other businesses, many health systems are making remote arrangements permanent for certain administrative roles and moving to a flexible approach regarding their team and their space in the future.
2. Focus on Health Equity, Not Just Health Care: This was perhaps the most notable and encouraging change from presentations in past years at J.P. Morgan. I have been going to the conference for over a decade, and I’ve never heard someone mention this term or outline their efforts on “health equity” — this year, nearly everyone did. In the past, they have outlined many wonderful programs on “social determinants of health,” but this year they have seen the disproportionate impact of COVID on low-income communities bringing the ongoing issue of racial disparities in access to care and outcomes to light. As the bedrock of employment in their community, this provides an opportunity to not just provide health care, but also health equity, taking an active role to help make progress on issues like hunger, homelessness, and housing. Many are making significant investments in a number of these and other areas.
3. Take the Lead in Public Health — the Message is the Medicine:One of the greatest failings of COVID, perhaps the greatest lesson learned, is the need for clear and consistent messaging from a public health perspective. That is a role that healthcare providers can and should play. In the pandemic, it represented the greatest opportunity to save lives as the essence of public health is communication — the message is the medicine. A number of health systems stepped into this opportunity to build trust and to build their brand, which are essentially one in the same. Some organizations have created a new role — a Chief Community Health Officer — which is a good way to capture the work that is in motion relative to social determinants of health as well as health equity. Many understand the opportunity here and will take the lead relative to vaccine distribution as clear messaging to build confidence is clearly needed.
4. Make the Home and Everywhere a Venue of Care:A number of presenters stated that “COVID didn’t change our strategy, it accelerated it.” For the most part, they were referring to virtual visits, which increased dramatically now representing around 10 percent of their visits vs. 1 percent before-COVID. One presenter said, “Digital has been tested and perfected during COVID,” but that is only considering the role we see digital playing in this moment. It is clear some organizations have a very narrow tactical lens while others are looking at the opportunity much more strategically. For many, they are looking at a “care anywhere and everywhere” strategy. From a full “hospital in the home” approach to remote monitoring devices, it is clear that your home will be seen as a venue of care and an access point moving forward. The pandemic of 2020 may have sparked a new era of “post-hospital healthcare” — stay tuned.
5. Bury Your Budget and Pivot to Planning:The budget process has been a source of incredible distrust, dissatisfaction and distraction for every health system for decades. The chaos and uncertainty of the pandemic forced every organization to bury their budget last year. With that said, many of the organizations that presented are now making a permanent shift away from a “budget-based culture” where the focus is on hitting a now irrelevant target set that was set six to nine months ago to a “performance-based culture” where the focus is on making progress every day, week, month and quarter. Given that the traditional annual operating budget process has been the core of how health systems have operated, this shift to a rolling forecast and a more dynamic planning process is likely the single most substantial and permanent change in how hospitals and health systems operate due to COVID. In other words, it is arguably a much bigger headline than what’s happened with virtual visits.
6. Get Your M&A Machine in Motion: It was clear from the presentations that activity around acquisitions is going to return, perhaps significantly. These organizations have strong balance sheets and while the strong have gotten stronger during COVID, the weak have in many cases gotten weaker. Many are going to be opportunistic to acquire hospitals, but at the same time they have concluded that they can’t just be a system of care delivery. They are also focused on acquiring and investing in other types of entities as well as forming more robust partnerships to create new revenue streams. Organizations that already had diversified revenue streams in place came through this pandemic the best. Most hospitals are overly reliant on the ED and surgical volume. Trying to drive that volume in a value-based world, with the end of site of service differentials and the inpatient only list, will be an even bigger challenge in the future as new niche players enter the market. As I wrote in the headline of my summary two years ago, “It’s the platform, stupid.” There are better ways to create a financial path forward that involve leveraging their assets — their platform — in new and creative ways.
7. Hey, You, Get into the Cloud:With apologies for wrapping a Rolling Stones song into a conference summary, one of the main things touted during presentations was “the cloud” and their ability to pull clinical, operational and financial dashboards together to monitor the impact of COVID on their organization and organize their actions. Focus over the last decade has been on the clinical (implementing EHRs), but it is now shifting to “digitizing operations” with a focus on finance and operations (planning, cost accounting, ERPs, etc.) as well as advanced analytics and data science capabilities to automate, gather insight, manage and predict. It is clear that the cloud has moved from a curiosity to a necessity for health systems, making this one of the biggest areas of investment for every health system over the next decade.
8. Make Price Transparency a Key Differentiator: One of the great lessons from Amazon (and others) is that you can make a lot of money when you make something easy to buy. While many health systems are skeptical of the value of the price transparency requirements, those that have a deep understanding of both their true cost of care and margins are using this as an opportunity to prove their value and accelerate their strategy to become consumer-centric. While there is certainly a level of risk, no business has ever been unsuccessful because they made their product easier to understand and access. Because healthcare is so opaque, there is an opening for healthcare providers to build trust, which is their main asset, and volume, which is their main source of revenue, by becoming stunningly easy to do business with. This may be tough sledding for some as this isn’t something healthcare providers are known for. To understand this, spend a few minutes on Tesla’s website vs. Ford’s. The concept of making something easy, or hard, to buy will become crystal clear as fast as a battery-driven car can go from zero to 60.
9. Make Care More Affordable:This represents the biggest challenge for hospitals and health systems as they ultimately need to be on the right side of this issue or the trust that they have will disappear and they will remain very vulnerable to outside players. All are investing in advanced cost accounting systems (time-driven costing, physician costing, supply, and drug costing) to truly understand their cost and use that as a basis to price more strategically in the market. Some are dropping prices for shoppable services and using loss leader strategies to build their brand. The incoming Secretary of Health and Human Services has a strong belief regarding the accountability of health systems to be consumer centric. The health systems that understand this are working to get ahead of this issue as it is likely one of their most significant threats (or opportunities) over the next decade. This means getting all care to the right site of care, evaluating every opportunity to improve, and getting serious about eliminating the need for expensive care through building healthy communities. If you’re worried about Wal-Mart or Amazon, this is your secret weapon to keep them on the sideline.
10. Scale = Survival: One of the big lessons here is that the strong got stronger, the weak got weaker. For the strong, many have been able to “snapback” in financial performance because they were resilient. They were able to designate COVID-only facilities, while keeping others running at a higher capacity. To be clear, while most health systems are going to get to the other side and are positioned better than ever, there are many others that will continue to struggle for years to come. According to our data at Strata, we see 25 percent operating at negative margins right now and another 50 percent just above breakeven. They key to survival moving forward, for those that don’t have a captive market, will be scale. If this pandemic proved one thing relative to the future of health systems it is this — scale equals survival.
When Will We Return to Normal?
Based on what the projections that these health systems shared, the “new normal” for health systems for the first half of 2021 will be roughly 95 percent of prior year inpatient volume with a 20 percent year-over-year drop in ED volume and a drop of 10-15 percent in observation visits. So, the pain will continue, but given the adjustments that were already made in 2020, it looks like they will be able to manage through COVID effectively. While there will be a pickup in the second half of 2021, the safe bet is that a “return to normal” pre-COVID volumes likely won’t occur until 2022. And there are some who believe that some of the volume should have never been there to begin with and we might see a permanent shift downward in ED volume as well as in some other areas.
With that said, I’ll steal a quote from Bert Zimmerli, the CFO of Intermountain Healthcare, who said, “Normal wasn’t ever nearly good enough in healthcare.”In that spirit, the goal should be to not return to normal, but rather to use this moment as an opportunity to take the positive changes driven by COVID — from technology to processes to areas of focus to a sense of responsibility — and make them permanent.
Thanking Our “Healthcare Heroes”
We’ll never see another 2020 again, hopefully. With that said, one of the silver linings of the year is everything we learned in healthcare. The most important lesson was this — in healthcare there are literally heroes everywhere. To each of them, I just want to say “thank you” for being there for us when we needed you the most. We should all be writing love letters to those on the front line who risked their lives to save others. Our nation’s healthcare system has taken a lot of criticism through the years from those on the outside, often with a blind eye to how things work in practice vs. in concept. But this year we all got to see first-hand what’s happening inside of healthcare — the heroic work of our healthcare providers and those who support them.
They faced the worst crisis in the history of healthcare. They responded heroically and were there for our families and friends.
They proved that healthcare is too vital to fail. They proved that healthcare is pandemic-proof.
Workers have rights, but the answer is more complicated than you think.
En español | With millions of people out of work and millions of others forced to work from home, the pandemic has reshaped the nation’s labor force. And it’s not done yet. As the unemployed look ahead to getting hired and remote employees prepare for a return to the workplace, many are contemplating the same question: Could they eventually be required to get a COVID-19 vaccination if they want to keep their jobs?
The question has become more urgent since the U.S. Food and Drug Administration (FDA) granted Pfizer and BioNTech’s coronavirus vaccine emergency use authorization on Dec. 11. The short answer: Yes. An employer can make a vaccination a requirement if you want to continue working there. But there are significant exceptions for potential concerns related to any disability you may have and for religious beliefs that prohibit vaccinations. And experts say that employers are more likely to simply encourage their workers to get immunized rather that issue a company-wide mandate.
On Dec. 16, the Equal Employment Opportunity Commission (EEOC) confirmed that a COVID-19 vaccination requirement by itself would not violate Americans with Disabilities Act (ADA). That law prohibits employers from conducting some types of medical examinations.
“If a vaccine is administered to an employee by an employer for protection against contracting COVID-19, the employer is not seeking information about an individual’s impairments or current health status and, therefore, it is not a medical examination,” the EEOC says.
But some employees may be exempted from mandatory vaccinations based on potential concerns related to any disability you may have and for religious beliefs that prohibit vaccinations. And experts say that employers are more likely to simply encourage their workers to get immunized rather that issue a company-wide mandate.
“Employment in the United States is generally ‘at will,’ which means that your employer can set working conditions,” says Dorit Reiss, a law professor at the University of California, Hastings, who specializes in legal and policy issues related to vaccines. “Certainly, employers can set health and safety work conditions, with a few limits.”
Those restrictions generally are tied to the federal Americans with Disabilities Act (ADA) and Title VII of the Civil Rights Act of 1964. If employees have medical reasons or sincerely held religious beliefs that prevent them from taking a potential coronavirus vaccine, employers could be legally required to give the workers some reasonable alternative to continue to work, Reiss says.
The EEOC guidance notes that even if an employer finds that a worker who cannot be vaccinated due to disability poses a risk to the workplace, the employer cannot exclude the employee from the job — or take any other action — unless there is no way to provide a reasonable accommodation that would reduce this risk to others.
“That might be a [wearing a] mask, a working from home, or a working separately from other people alternative. As long as it’s not too significant a barrier for the employer,” Reiss says. “If you can achieve the same level of safety as the vaccine via mask, or remote working, you can’t fire the employee. You need to give them an accommodation.”
Vaccine recommendations vs. requirements
The potential medical and religious accommodations are just two of the factors employers will have to consider when deciding whether to put a vaccination requirement in place. Experts say that given all the different concerns employers will need to balance with a potential COVID-19 vaccine, many might choose to simply recommend their workers get immunized rather than make vaccination a condition of employment.
For example, employers also need to weigh any liability issues a vaccination requirement might raise. Some federal lawmakers already have raised concerns that employers are vulnerable to lawsuits from workers and customers who might have contracted COVID-19 at the business. A mandate that all their employees get inoculated could complicate the risks for companies.
“It’s a treacherous area for employers,” says Jay Rosenlieb, an employment law attorney at the Klein DeNatale Goldner law group in California. “The reason it’s treacherous for employers is liability that arises from requiring a vaccine where the vaccine goes sideways and creates harm to the employee. That’s going to probably be a workers compensation claim against the employer. And, of course, some kind of claim against the vaccine manufacturer. There’s a lot of weighing that goes on here.”
L.J. Tan, chief strategy officer for the Immunization Action Coalition — an advocacy group that supports vaccinations — says that because potential COVID-19 vaccines are largely being developed in the same manner as earlier vaccines, researchers have the benefit of past scientific experience to better ensure that a vaccine for this coronavirus will be safe. But he noted that the speed of the development of a COVID-19 vaccine — compressed into months rather than the usual years — and the politics that have accompanied it add to the reasons employers may be unwilling to make vaccination a requirement.
“One of the challenges we’re going to be dealing with, obviously, especially now is that there is a shadow of politics over the vaccine,” Tan says. “As a result, there’s some fear about whether the vaccine can be safe, whether it can be approved appropriately. Because of that shadow, I think it’s going to be extremely difficult for an employer to make COVID-19 vaccination a condition of employment.”
Vaccine requirement more likely in health care, other high-risk jobs
The industry most likely to require COVID-19 vaccinations for workers is health care, where most employers already require workers to get a flu shot annually. In fact, interim guidance from the Centers for Disease Control and Prevention (CDC) on which groups might be among the first to have access to a coronavirus vaccine placed “healthcare personnel likely to be exposed to or treat people with COVID-19” at the top of the list.
But once enough doses of a vaccine have been produced for distribution to the broader public, some employers might start to consider a mandate.
“For example, essential workers in retail stores or in food production plants, such as a meat-packing plant, seem to be at high risk,” Reiss says. “Those employers could reasonably require [a COVID vaccination], because remember, if an employee doesn’t vaccinate, it’s not just a risk to them. It’s a risk to other employees, and — if it’s a customer-facing business — a risk to the customers. So, in high-risk places, I think it’s reasonable.”
Some companies may make inoculation voluntary but make it as easy as possible for workers to get the shot. For instance, Ford already has purchased twelve of the ultracold freezers required to store doses of Pfizer’s vaccine so it can provide the shot to employees who want it.
For those workers who might be told to get a vaccination, remember to raise any concerns you might have with your employer.
“Ask for reasonable accommodation and have a discussion with the employer as to whether there might be reasonable alternatives such as work from home or such as continued use” of personal protective equipment, Rosenlieb says.
If vaccination requirements do become more common, both workers and their employers will have to find ways to balance personal concerns with public safety.
“On one hand, [vaccine requirements] do limit the autonomy of workers that have reservations,” Reiss says. “On the other hand, they also protect workers by making the workplace safer from the disease. So, it’s not just a mandate to limit your rights. A mandate can also protect your right to a safe work environment.“
Twenty states and dozens of localities increased their minimum wage on Friday, giving a financial boost to many frontline workers during the pandemic.
New Mexico will see the largest jump, adding $1.50 to its hourly minimum and bringing it up to $10.50. Arkansas, California, Illinois and New Jersey will each increase their minimum wages by $1.
Alaska, Maine and South Dakota will increase wages by just 15 cents an hour, while the rate in Minnesota will rise by half that, at 8 cents, to $10.08 an hour.
Additional increases are scheduled for elsewhere this year, with most changes taking effect on July 1.
Low-income earners, like much of the country’s workforce, have seen their wages remain relatively stagnant for decades when inflation is taken into account. Proponents say the new raises will help reduce poverty and offer much-needed pay hikes to some of the most vulnerable workers.
“Minimum wage increases income levels, reduces poverty, so I think it’s pretty clear that it improves conditions in the lower end of the wage distribution,” said Daniel Kuehn a research associate at The Urban Institute.
Localities are also boosting their minimum pay. Flagstaff, Ariz., will see wages rise from $13 an hour to $15, as will Burlingame, Calif.
In some municipalities, the increases are dependent on business size. Hayward, Calif., for example, will follow the same wage hike as Burlingame, but employers who 25 or fewer workers will need to raise wages from $12 an hour to $14.
Varying minimum wages across localities, Kuehn said, lets governments take into account different cost-of-living conditions.
“I think the ideal policy would include a lot of local variation, but that doesn’t mean a federal floor isn’t helpful,” he said.
The federal minimum wage has been stuck at $7.25 since 2009. In recent years, the goal of a $15 minimum wage has become a standard progressive policy.
House Democrats in July 2019 passed a bill that would gradually increase the federal minimum wage to $15 gradually through 2025, but the measure died in the GOP-controlled Senate.
“While families work hard to make ends meet, their cost of living has surged to unsustainable highs, inflation has eaten nearly 20 percent of their wages and the GOP’s special interested agenda has left them behind,” Speaker Nancy Pelosi (D-Calif.) said at the time.
“No one can live with dignity on a $7.25 an hour wage,” she added.
The issue is back in the political spotlight again with Tuesday’s runoff elections in Georgia that will determine which party controls the Senate for the next two years.
The Democratic challengers are arguing that the federal minimum wage will only increase if they win both races.
“If the federal minimum wage kept up with the cost of living, it would be even higher than $15,” Democratic candidate Jon Ossoff said last week. “The basic premise is that anybody in this country working a single full-time job should be bringing home enough money to sustain themselves and then some.”
But critics argue that minimum wage increases could slow job growth by raising labor costs for employers, an issue of particular concern during the fragile recovery from the coronavirus recession.
“A dramatic increase in the minimum wage even in good economic times has been shown to be harmful,” said Michael Saltsman, the managing director for the Employment Policy Institute, a think tank tied to the restaurant and hospitality industry.
“In the current climate, for many employers it could be the final nail in the coffin,” he added.
Saltsman argued that increasing anti-poverty programs such as the Earned Income Tax Credit are better policies than wage increases. The tax credit essentially operates as a government subsidy for low-wage work, shifting the onus of paying the extra wages from businesses to taxpayers.
Kuehn said there is little evidence to suggest that small and gradual increases of the minimum wage have significant effects on employment.
“The minimum wage increase levels we see get passed are not large enough to have significant employment effects,” he said.
But he concedes that it’s harder to predict the effects of a quick nationwide boost toward $15.
“I think it’s important to note that since we’ve never had a federal increase of that magnitude, there’s a lot we don’t know,” he said. “With something of that size, you would worry about low-wage places like Mississippi or Alabama.”
A report from the nonpartisan Congressional Budget Office in 2019 projected that a gradual increase to $15 through 2025 would mean “1.3 million workers who would otherwise be employed would be jobless in an average week in 2025.”
But it also specified a range of possible outcomes, including no job losses on the low end and as many as 3.7 million jobs lost on the high end.
The report found that 27 million people would see higher income, and that the poorest families would have wages rise as much as 5.2 percent.
Researchers such as Kuehn are adamant that businesses can handle increasing wages at moderate levels, even in the midst of a global health crisis.
“It certainly doesn’t make businesses’ lives easier, but businesses aren’t struggling right now because of wage costs,” he said.
Amid the surge in the ranks of the unemployed during the pandemic, another crucial problem in the labor market has gone mostly overlooked: Workers are calling out sick in record numbers this year.
Whether it’s because they have Covid-19 themselves, are worried about getting it or are taking care of someone who already has it, the number of workers who’ve missed days on the job has doubled in the pandemic.
What’s more, unlike the jobless rate, which has steadily declined from its April peak, the rate of abseenteism — as it is called by economists — has remained stubbornly high. Almost 1.8 million workers were absent in November because of illness, nearly matching the record 2 million set back in April, according to Labor Department data.
These lost days of work are sapping an economic recovery that’s been progressing in fits and starts for much of the past several months. While some indicators have improved markedly, others such as retail sales and consumer spending and incomes have weakened as the pandemic rages on and local governments impose fresh restrictions on businesses and travel.
Michael Gapen, chief U.S. economist at Barclays Plc, said that the vaccine could start driving down absenteeism by the second quarter. Until then, he said, the missed work is leading to supply chain disruptions.
Absenteeism “could lead to shortages, it could lead to higher prices and more restrained output,” Gapen said.
With about 1.5 million new cases per week and deaths at a record pace, employee absenteeism may remain elevated for some time, especially in early 2021 before vaccines are widely distributed and with the rollout in the U.S. moving slower than government officials expected.
Factory Workers
While the Labor Department data tracks people currently in the labor force who are out sick, a separate survey by the Census Bureau captures an even wider view of the challenge. Its latest Household Pulse Survey — based on responses in late November and early December — estimates that more than 11 million people weren’t working because of the virus. The figures also include those who refrained from working because they were worried about getting or spreading the virus, and those caring for someone with symptoms.
The effects of missing workers are especially concentrated in manufacturing. Absenteeism, combined with short-term shutdowns to sanitize facilities and difficulties in returning and hiring workers, limit the sector’s growth potential, according to Timothy Fiore, chair of the Institute for Supply Management’s Manufacturing Business Survey Committee.
The group’s gauge of factory activity grew at a slower pace in November, with the employment component falling back to a level that indicates contraction.
“It’s not a lack of work,” Fiore said on a recent call with reporters, noting absenteeism especially for low- to medium-skill roles. “It’s a lack of people.”
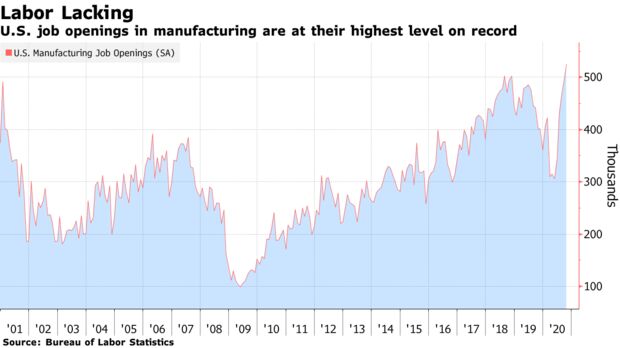
In addition to temporarily absent workers, the manufacturing sector has 525,000 job openings, the most in Labor records back to 2000.
Auto plants are feeling the effects. General Motors Co. put white-collar employees on the production floor in August to cope with high absenteeism amid strong demand. Volkswagen AG Chief Financial Officer Frank Witter has said high levels of missing staff left the automaker “at times struggling to get all the cars built for customer orders.”
U.S. businesses have reported that surging cases precipitated plant closings and infection fears, adding to labor challenges including absenteeism and attrition, according to the Federal Reserve’s latest Beige Book summary of economic conditions. Manufacturers in the Chicago region have used overtime to make up for staff shortages, the Dec. 2 report said.
Sick Leave
For office workers, 90% of professionals said before the pandemic they’d sometimes go to work sick, according to a 2019 study by staffing firm Accountemps. Covid changed the conversation, and more employees are staying home to protect themselves and others.
The Families First Coronavirus Response Act earlier this year made the decision to stay home easier for some Americans by allowing two weeks of paid sick leave for certain employees. The law also allows leave for those unable to work because they must care for a child.
The latest stimulus bill, signed by President Donald Trump on Dec. 27, includes an extension of the act through March 31, but makes paid leave voluntary for employers rather than mandatory as it was in the first iteration. That may continue the trend of workers staying home depending on how many employers choose to grant the leave.
The act, however, excludes essential workers, which means those employed at facilities such as meatpacking plants can’t take advantage of the policy. That in turn can lead to workplace outbreaks and further disrupt production.
With fewer employees at work, slaughter rates at U.S. meat plants fell in the third quarter. Tyson Foods Inc. Chief Executive Officer Dean Banks said on a recent earnings call that absenteeism has “increased the cost and complexity of our operations” and that the company expects that to continue in 2021.