Dallas-based Baylor Scott & White Health will outsource, lay off or retrain 1,700 employees who work in information technology, billing, revenue cycle management and other support services, according to The Dallas Morning News.
The health system said outsourcing the finance and IT jobs and other support services will help it improve efficiencies and focus on reducing costs in noncore business areas. About two-thirds of the 1,700 employees will be joining third-party RCM, IT, billing or support staff vendors.About 600 to 650 positions will be eliminated.
Baylor Scott & White said that employees whose positions are being eliminated will be invited to participate in retraining programs.
The retraining program would allow the employees to remain employed at the health system and receive the same pay or higher, depending on their role, according to the report. Some of the retraining programs that will be available are learning to become a certified medical assistant or learning a job in patient support services.
“In no case — in no case — is anyone going to miss a paycheck,” Baylor Scott & White CEO Jim Hinton, told The Dallas Morning News. “We can afford to make these commitments, and we want to do the right thing for the great employees of Baylor, Scott & White. They’ve really done everything we’ve asked and more during this last year.”
This is the third time Baylor Scott & White has announced cost-cutting initiatives related to its workforce since the pandemic began. Last May, 930 Baylor Scott & White employees were laid off, and in December the health system said it would lay off employees and outsource 102 corporate finance jobs.
Mr. Hinton said that Baylor Scott & White has 2,000 clinical positions open, and it is investing in a new regional medical school campus and a joint venture to improve care for the underinsured.
“This is a transition to a new business model, a transition to a new way of working,” Mr. Hinton told The Dallas Morning News.
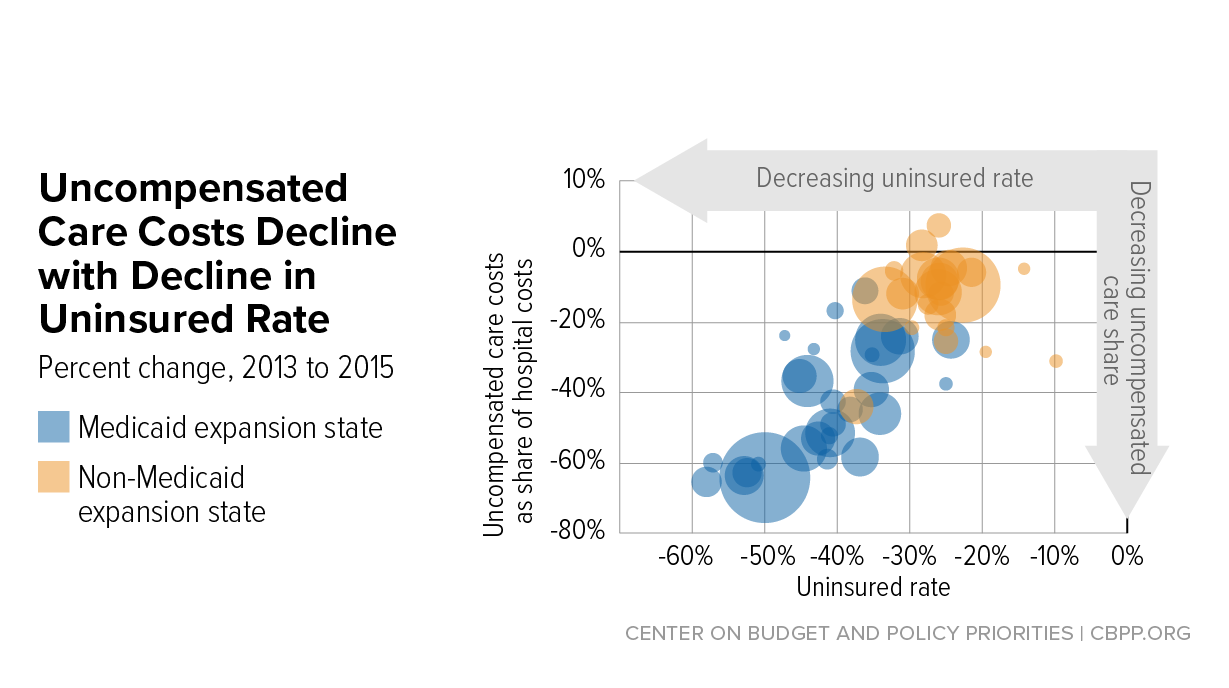
Hospital uncompensated care costs were up from $41.3B in 2018 and $38.4B in 2017, revealing an upward trend, according to AHA data.
Hospital uncompensated care costs increased right before the COVID-19 pandemic hit, according to new data from the American Hospital Association (AHA).
AHA data showed that hospitals incurred a new high of $41.61 billing in uncompensated care costs in 2019, the most recent year for which the group had complete data.
Uncompensated care costs in 2019 were up from $41.3 billion in 2018 and $38.4 billion in 2017 and were the second-highest per AHA records. Hospitals reported the most uncompensated care costs in 2013 when they incurred $46.8 billion.
Hospital uncompensated care costs decreased after the all-time high in 2013, but have recently started to tick back up after holding steady at $38.4 in 2016 and 2017.
In just the last 20 years, hospitals of all types have provided more than $660 billion in uncompensated care to patients, AHA reported. And that figure does not fully account for other ways in which provides provide financial assistance to patients of limited means, the group stated.
Each year, AHA aggregates data on uncompensated care, or care provided for which no reimbursement is received by hospitals from patients or payers. The data comes from the group’s Annual Survey of Hospitals, a comprehensive report of hospital financial data.
Uncompensated care is the sum of a hospital’s bad debt and financial assistance it provides, AHA explained.
Bad debt occurs when a hospital does not expect to obtain reimbursement for care provided, such as when patients are unable to pay their financial responsibility and do not qualify for financial assistance or are unwilling to pay their bills.
Hospitals also provide varying levels of financial assistance, AHA added. Financial assistance supports patients who cannot afford to pay and qualify for support from the hospital based on policies it has established based on the facility’s mission, financial condition, and geographic location, among other factors.
Combined, bad debt and financial assistance charges total a hospital’s uncompensated care charges, which is then multiplied by a hospital’s cost-to-charge ratio to determine total uncompensated care costs.
AHA noted that it expressed uncompensated care in costs versus charges because of significant variations in hospital payer mixes. Publishing the information as costs rather than charges enables better comparison across hospitals, the group said.
Nearly half of hospitals (48 percent) have seen bad debt and uncompensated care increase recently as a result of the ongoing COVID-19 pandemic, an analysis from consulting firm Kaufman Hall revealed.
More than 40 percent of hospitals also reported increases in percentage of uninsured or self-pay patients (44 percent) and the percentage of Medicaid patients (41 percent), which both contribute to unfunded or underfunded care at hospitals.
“The challenges brought on by the COVID-19 pandemic have affected nearly every aspect of hospital financial and clinical operations,” Lance Robinson, a managing director at Kaufman Hall, said at the time. “Organizations have responded to the challenge by adjusting their operations and strengthening important community relationships.”
Hospital uncompensated care costs – and bad debt as a result – are likely to increase in 2020 as hospitals come to terms with the impact COVID-19 has had on their financial health.
Already, hospitals have lost an estimated $323 billion in 2020 as a result of the COVID-19 pandemic, according to earlier projections from AHA.
About half of US hospitals also started the year in the red, AHA and Kaufman Hall stated in a recent report. The organizations predicted that hospital margins would sink to -7 percent in the second half of 2020 without comprehensive financial support from the government, but could decrease to a low of -11 percent if COVID-19 continued to periodically surge as it has.
Hardly one month into 2021, the pressing priorities facing healthcare leaders are abundantly clear.
First, we will be living in a world preoccupied by COVID-19 and vaccination for many months to come. Remember: this is a marathon, not a sprint. And the stark reality is that the vaccination rollout will continue well into the summer, if not longer, while at the same time we continue to care for hundreds of thousands of Americans sickened by the virus. Despite the challenges we face now and in the coming months in treating the disease and vaccinating a U.S. population of 330 million, none of us should doubt that we will prevail. Despite the federal government’s missteps over the past year in managing and responding to this unprecedented public health crisis, historians will recognize the critical role of the nation’s healthcare community in enabling us to conquer this once-in-a-generation pandemic.
While there has been an overwhelming public demand for the vaccine during the past couple of weeks, there remains some skepticism within the communities we serve, including some of the most-vulnerable populations, so healthcare leaders will find themselves spending time and energy communicating the safety and efficacy of vaccines to those who may be hesitant. This is a good thing. It is our responsibility to share facts, further public education and influence public policy.COVID-19 has enhanced public trust in healthcare professionals, and we can maintain that trust if we keep our focus on the right things — namely, how we improve the health of our communities.
And as healthcare leaders diligently balance this work, we also have a great opportunity to reimagine what our hospitals and health systems can be as we emerge from the most trying year of our professional lifetimes. How do you want your hospital or system organized? What kind of structural changes are needed to achieve the desired results? What do you really want to focus on? Amid the pressing priorities and urgent decision-making needed to survive, it is easy to overlook the great reimagination period in front of us. The key is to forget what we were like before COVID-19 and reflect upon what we want to be after.
These changes won’t occur overnight. We’ll need patience, but here are my thoughts on five key questions we need to answer to get the right results.
1. How do you enhance productivity and become more efficient? Throughout 2021, most systems will be in recovery mode from COVID’s financial bruises. Hospitals saw double-digit declines in inpatient and outpatient volumes in 2020, and total losses for hospitals and health systems nationwide were estimated to total at least $323 billion. While federal relief offset some of our losses, most of us still took a major financial hit. As we move forward, we must reorganize to operate as efficiently as possible. Does reorganization sound daunting? If so, remember the amount of reorganization we mustered to work effectively in the early days of the pandemic. When faced with no alternative, healthcare moved heaven and earth to fulfill its mission. Crises bring with them great clarity. It’s up to leaders to keep that clarity as this tragic, exhausting and frustrating crisis gradually fades.
2. How do you accelerate digital care? COVID-19 changed our relationship with technology, personally and professionally. Look at what we accomplished and how connected we remain. We were reminded of how high-quality healthcare can go unhindered by distance, commutes and travel constraints with the right technology and telehealth programs in place. Health system leaders must decide how much of their business can be accommodated through virtual care so their organizations can best offer convenience while increasing access. Oftentimes, these conversations don’t get far before confronting doubts about reimbursement. Remember, policy change must happen before reimbursement catches up. If you wait for reimbursement before implementing progressive telehealth initiatives, you’ll fall behind.
3. How will your organization confront healthcare inequities? In 2020, I pledged that Northwell would redouble its efforts and remain a leader in diversity and inclusion. I am taking this commitment further this year and, with the strength of our diverse workforce, will address healthcare inequities in our surrounding communities head-on. This requires new partnerships, operational changes and renewed commitments from our workforce. We need to look upstream and strengthen our reach into communities that have disparate access to healthcare, education and resources. We must push harder to transcend language barriers, and we need our physicians and medical professionals of color reinforcing key healthcare messages to the diverse communities we serve. COVID-19’s devastating effect on communities of color laid bare long-standing healthcare inequalities. They are no longer an ugly backdrop of American healthcare, but the central plot point that we can change. If more equitable healthcare is not a top priority, you may want to reconsider your mission. We need leaders whose vision, commitment and courage match this moment and the unmistakable challenge in front of us.
4. How will you accommodate the growing portion of your workforce that will be remote?Ten to 15 percent of Northwell’s workforce will continue to work remotely this year. In the past, some managers may have correlated remote work and teams with a decline in productivity. The past year defied that assumption. Leaders now face decisions about what groups can function remotely, what groups must return on-site, and how those who continue to work from afar are overseen and managed. These decisions will affect your organizations’ culture, communications, real estate strategy and more.
5. How do you vigorously hold onto your cultural values amid all of this change? This will remain a test through 2021 and beyond. Culture is the personality of your organization. Like many health systems and hospitals, much of Northwell’s culture of connectedness, awareness, respect and empathy was built through face-to-face interaction and relationships where we continually reinforced the organization’s mission, vision and values. With so many employees now working remotely, how can we continue to bring out the best in all of our people? We will work to answer that question every day. The work you put in to restore, strengthen and revitalize your culture this year will go a long way toward cementing how your employees, patients and community come to see your organization for years to come. Don’t underestimate the power of these seemingly simple decisions.
While we’ve been through hell and back over the past year, I’m convinced that the healthcare community can continue to strengthen the public trust and admiration we’ve built during this pandemic. However, as we slowly round the corner on COVID-19, our future success will hinge on what we as healthcare organizations do now to confront the questions above and others head-on. It won’t be quick or easy and progress will be a jagged line. Let’s resist the temptation to return to what healthcare was and instead work toward building what healthcare can be. After the crisis of a lifetime, here’s our opportunity of a lifetime. We can all be part of it.
Vic Gara, 57, at his home in West Granby Dec. 10, 2020. Gara survived COVID-19 in a hospital ICU bed on a ventilator. Months later, he discovered he was experiencing long-term complications from the virus.
In early March, Vic Gara came down with severe muscle aches, headaches and a rising blood pressure, indicators of COVID-19 that weren’t well understood early on in the pandemic.
“Taking a shower, just the water hurt my body,” he said. “I couldn’t sleep. I slowly became hypoxic. I just couldn’t breathe.”
Eventually, he was admitted to Hartford Hospital, where he was quarantined immediately and separated from his wife, Laura.
“My wife was walking in from after parking the car, and I saw her from maybe 15, 20 feet away and I just barely raised my hand and said goodbye to her,” Gara recalled. “And I was there for a month.”
The 57-year-old was intubated and spent 11 days on a ventilator, which helped him breathe, before he regained consciousness. Like so many others who required intensive care, Gara was first transferred to a rehabilitation hospital for a short time before he could return to his home in West Granby.
He thought the worst was behind him. But by midsummer, Gara struggled with exhaustion, his headaches returned, he had poor balance and trouble speaking and “brain fog” had set in. Then he joined an online support group for COVID-19 survivors.
“Not until I was contacted did I find out, ‘Oh my god, there’s other people like me that are suffering almost identical situations,’” he said.
There is an untold number of COVID-19 survivors worldwide who struggle with long-term symptoms and complications from the virus. Scientists don’t yet know how common this occurs, but what they do know is symptoms can be both physical and mental in nature, and they can delay people from making a full recovery.
As the phenomenon becomes more well-known and researched, health organizations across Connecticut and the country are creating and expanding dedicated COVID-19 recovery programs to help survivors.
“We’re now seeing patients that have had some of those symptoms for eight, nine months,” said Dr. Jerry Kaplan, outpatient medical director at Gaylord Hospital in Wallingford. He runs the organization’s new COVID-19 recovery and rehabilitation program.
The hospital created an online support group over the summer for former COVID-19 rehab patients like Gara. Kaplan said that’s when patients came forward with a wide range of lingering health issues.
Gaylord opened its specialized outpatient program in early fall, and it provides COVID-19 survivors with occupational and physical therapies, nutrition education, psychological treatment and other services.
“Even if you can’t do everything you were doing before, we can get you to the highest possible functional level,” Kaplan said, “and that’s really what the program is designed to do.”
The program has picked up in the last several months as long-term complications from COVID-19 illness become more well-known.
“As we see more patients hospitalized with COVID now, we will continue to see the need for COVID recovery programs in the future,” Kaplan said.
The Post-COVID-19 Recovery Program at Yale Medicine opened several months ago as a Friday clinic with a small patient roster. Dr. Denyse Lutchmansingh said it has now expanded to three days a week as more patients and medical clinicians discover the program.
“I think early on, people would say, give it a couple of weeks and you should feel better,” she said. “And now we’re well past that give-it-a-couple-of-weeks period and people are still having symptoms.”
Lutchmansingh, a pulmonary and critical care physician who leads the Yale recovery program, said she and her colleagues initially expected that patients who had had moderate to severe COVID-19 illness, like Gara, would be the ones needing long-term recovery services the most.
That’s only been partly true.
“Patients who were classified as mild disease have also had persistent symptoms almost as severe as a patient who was hospitalized in an intensive care unit, and that has been quite eye-opening,” she said.
Lutchmansingh said the clinic is also seeing a surprisingly young population. She has patients in their 30s and 40s who were runners, athletically inclined, or generally in good health prior to getting a mild case of COVID-19 “who now struggle to walk up a flight of stairs.”
It’s some of these patients that Lutchmansingh has seen struggle the most mentally with their persistent symptoms.
“Because they expected to recover very quickly and move on,” she said.
Dr. Serena Spudich is the division chief of neurological infections and global neurology at Yale School of Medicine and leads a designated neuro-COVID clinic, which opened in October.
Her team collaborates with Lutchmansingh and other clinicians in the greater community to get referrals for COVID-19 survivors suffering with tingling and numbness, loss or impaired senses of smell, taste and hearing, headaches, cognitive impairment and other complications.
Many of these patients were never hospitalized or never required intensive care for COVID-19.
This is where more research can help make sense of the trends that health providers are seeing in their COVID-19 “long hauler” patients, Spudich said.
“I think it’s really important to try to understand why some people get these neurologic issues, and many people don’t seem to,” she said. “I know lots of people who’ve recovered from COVID who seem completely fine.”
Scientists are still trying to estimate exactly how many people in the world ever had COVID-19, including those who never got tested or people who got false negative results — cases that have not been recorded.
Only then might health experts know how common or rare long-term complications are among survivors, Spudich said.
“I think it’s important to be aware of them, to understand them and of course provide treatment for them,” she said. “But I worry that it’s sort of a fire that can take off where all the social media, all the press attention will suddenly make a lot of people think, ‘Oh, I’m having post-COVID problems.’”
“What is really, really important is getting patients who are having symptoms to a provider who can really critically take care of them and try to understand clinically what’s happening with them.”
What patients often want to know is, when will their health get back to what it was prior to COVID-19? And health experts don’t yet have a good answer to that as scientists continue to follow survivors in their recovery.
“We always make it clear to the patients that we don’t have all the answers. We are looking for answers,” Lutchmansingh said. “We remain hopeful, we have seen patients improve and build back to baseline, but it is a long pathway and it is not necessarily an easy pathway.”
For Gara, he continues recovery treatment at Gaylord on an outpatient basis. He tries to get outside more and build up his endurance with walks. For the most part, he takes it one day at a time.
“I went into it with an open mind and trying to stay positive,” he said. “I learned how to be more positive and look for the good rather than the bad. It helps.”
Hospitals are now required to disclose the prices they secretly negotiate with insurers.
But many are dragging their feet on the new regulations, which were passed under President Donald Trump and could very well stay in place under President Biden.
The rules went into place Jan. 1, but hospital compliance is spotty.
“Hospitals are playing a hide-and-seek game,” said Ge Bai, an expert on health-care pricing at Johns Hopkins Bloomberg School of Public Health.“Even with this regulation, most of them are not being fully transparent.”
Hospitals lost a bruising court battle last year to stop the rules, which require them to publish a list of prices for goods and services. The point is to bring more transparency to prices for medical goods and services — information that has long been inaccessible to consumers. The new rules were a centerpiece of Trump’s promise to inject more price transparency in the health-care system and curb surprise billing.
But Nisha Kurani, a policy analyst at the Kaiser Family Foundation who is tracking hospital responses to the new rule, said she’s seen the full gamut.
MedStar in Washington posted its prices in an Excel sheet on its website, but other hospitals only posted price estimates, uploaded files in difficult to use formats, or promised to release information only after someone inputs their insurance, Kurani said.
A Gothamist investigation found that only one of five major New York hospitals posted a list of their negotiated services to their website, and even then, not for all procedures. The fine for not complying with the new rules — $300 a day — is a drop in the bucket for many hospitals.
The rules probably aren’t going away anytime soon.
The Biden administration hasn’t taken any public position on the rules — and right now, officials are focused on reversing dozens of other Trump administration regulations they believe are damaging to health insurance and costs in the United States.
Revising the hospital transparency rules — if that’s even something the new administration wants to do — would likely be far down on the priority list, despite heavy lobbying by the hospital industry to suspend enforcement of the new rule.
Plus, price transparency is broadly popular among the public and was one of the planks of a joint health policy plan developed by a task force Biden formed with Sen. Bernie Sanders (I-Vt.) after the 2020 primary elections.
The American Hospital Association says staff who would help with compliance are stretched thin.
Molly Smith, the association’s group vice president for public policy, said many of the staff members who would normally be tasked with compiling and formatting the price data are the same people being asked to help set up patient registries and vaccine tracking systems in response to the pandemic.
“We’ve got a lot of hospitals that are at or beyond capacity,” Smith said.
A lawyer for the hospital association said that it is considering petitioning its legal case to the Supreme Court. Meanwhile, the lobbying group has been pushing the Biden administration to suspend enforcement of the new rule.
Consumer advocates like the transparency rules designed to protect patients and drive down health-care costs.
“In the past there was absolutely no power for the consumer. It was like highway robbery being committed every day by the health-care system,” said Cynthia Fisher, head of the nonprofit Patient Rights Advocate, which pushes for price transparency.
But now, Fisher says, “it’s the American consumer who is going to drive down the cost of care.”
But the effect might be modest.
Experts in health-care economics hotly debate whether the price transparency rules will, in fact, drive down costs. Even those who support the changes say the effect might be incremental.
“I don’t think it’s going to be an earthquake in terms of pricing, but it’s a first step in the right direction,” said Bai.
There are several reasons the new price transparency rule may not have a massive effect on hospital prices. Perhaps the biggest, and one often cited by the hospital lobby, is that most Americans are not going to pay the negotiated price for a procedure. Instead, they are likely to pay co-pays or coinsurance that amount to a fraction of this price.
This isn’t always true, of course. Those with high-deductible plans may pay the negotiated rate, and for those without insurance paying out of pocket, it can be helpful to get a peek behind the sticker price. But even for these patients, it may be challenging to extract useful information from unwieldy spreadsheets full of obscure billing codes.
Bai said that she is hopeful that third parties may make some of the pricing information easier for consumers to use. And some self-insured employers may start identifying cheaper providers and incentivizing patients to use them. The rules also require hospitals to provide cost-sharing estimates for commonly used procedures in an easily navigable format.
Still, price competition works only if there are players to compete.
The market for health care has become increasingly consolidated as hospitals merge and buy up physician practices. If a hospital is the only health-care provider in town, then there’s not a whole lot patients can do about high prices, even if they think they’re unfair.
“I don’t think transparency will fundamentally change the power balance between the payer and the hospital in many markets,” Bai said.
Although only 17 states are currently reporting data on the racial and ethnic breakdown of vaccine recipients, the early data indicate that there are significant disparities in who is getting vaccinated, with the share of Black and Latino people among vaccinees lower than their share of the total population in those states.
Alarmingly, in our recent conversations with health system executives,those same disparities seem to be present among healthcare workers employed by hospitals and health systems. Anecdotally, across a half-dozen health systems we’ve spoken with in the past week, most report that they’ve had about 70 percent of their workers agree to get the first dose of the COVID-19 vaccine.
However, that number looks significantly different when broken down by race and ethnicity:on average, the uptake rate among White, Asian, and Pacific Islander workers has been closer to 90-95 percent, while among Black and Latino workers, it’s been closer to 30-40 percent. Bear in mind these are employees of health systems—in many cases they’re frontline caregivers—and given their work environments you might expect them to be less hesitant to get the vaccine.
That 30-40 percent uptake rate is very worrisome, in two ways:caregivers outside of hospital settings, especially home care and nursing home workers, likely include a larger number of workers hesitant to get vaccinated. And in the general population, among whom health literacy is presumably much lower than among healthcare workers,it’s precisely those populations who are at highest risk of COVID infection, hospitalization, and death. (A further complication: health systems made it easy for their employees to get the shot. With vaccines for the general population still scarce, at-risk populations will inevitably have the most difficult time getting signed up, even if they want the vaccine.)
If health systems are the canary in the coal mine for vaccine hesitancy rates, we’re in for a tough challenge in getting the most vulnerable populations vaccinated in the months to come.
As vaccine eligibility guidelines have expanded to include adults over 65, we’ve heard from several friends and acquaintances looking for the inside scoop on getting a place in line. They’ve heard that their local health system is taking appointments, but only for established patients—do we know someone at the local system who could help them (or their mother, or their aunt with Stage IV cancer) get the shot?
One acquaintance was livid that his local hospital was prioritizing established patients:“They’re just rewarding people who have already paid them money. Is that fair?” It’s likely that system was making decisions based not on prior business relationships, but rather logistics. If patients are already “in the system”, they can be contacted and scheduled through the patient portal, fill out information online, and have their doses tracked in the EMR.
As health systems have been thrust into leading frontline vaccine distribution some have recognized an unprecedented opportunity to earn loyalty by connecting current and potential patients with the vaccine.
Outreach must provide clear information around vaccine access and how eligibility decisions are made(consider the difference in message between “we’re offering vaccines to current patients only”, and “because established patients can be quickly scheduled and monitored, we are beginning with this group, and plan to expand quickly”).
Systems’ ultimate goal should be getting vaccines to as many people as possible, as fast as possible, given supply and resource constraints.
The indictment describes an inside job involving Beaumont employees who sold stolen sponges, adhesives and instruments used to inspect eyes and ears. The equipment included cystoscopes, a thin tube with a camera that is inserted through the urethra and into the bladder.
“Some of the medical devices stolen and re-sold over the Internet were possibly contaminated devices that were previously used in various surgical and other medical procedures on patients,” according to the indictment.
The three individuals charged in the indictment are:
Paul Purdy, 49, of Bellbrook, Ohio
Valdet Seferovic, 32, of Auburn Hills
Zafar Khan, 40, of Fenton
Purdy and Seferovic not respond to messages seeking comment Thursday while Harold Gurewitz, a lawyer for Khan, declined comment. The three defendants are scheduled to make initial appearances Jan. 21 in federal court.
“These defendants used their employment status to circumvent the safety protocols established by Beaumont Hospital to profit from the theft of medical devices and put the health and safety of the general public at risk in doing so,” U.S. Attorney Matthew Schneider said in a statement.
The wire fraud and conspiracy charges listed in the 18-count indictment are punishable by up to 20 years in federal prison.
Beaumont officials have cooperated fully with the investigation, health system spokesman Mark Geary wrote in an email to The Detroit News.
“This kind of theft does a disservice to more than just Beaumont — it does a disservice to the community,” Geary wrote. “We have confidence in the legal process and trust a just result will be achieved.”
Purdy and Seferovic were friends who worked at Beaumont and had access to storage areas inside one of the system’s hospitals, prosecutors alleged. The duo gained access to medical supplies and devices, according to the government, and devised a plan to steal the equipment and sell the items throughout the U.S.
Purdy, who worked for Beaumont until resigning in 2017, never told buyers the items were stolen, prosecutors said. After he quit, Purdy recruited Seferovic to continue stealing items from the medical supply, cleaning and disinfecting rooms, according to prosecutors.
“Medical devices that are removed from their rightful place in a hospital or other medical setting put patients’ health at risk by denying them access to needed diagnostic imaging and treatment,” Lynda Burdelik, special agent in charge of the U.S. Food and Drug Administration’s Criminal Investigations field office in Chicago, said in a statement.
Purdy paid Seferovic for stolen items via PayPal and resold the devices on eBay and Amazon, according to the government. On March 28, 2018, the indictment alleges Purdy received a $4,800 wire payment from the sale of two cystoscopes.
That same day, Seferovic received a $2,550 payment via PayPal, according to the government.
In fall 2017, Seferovic also agreed to steal and sell medical devices and supplies to Khan, who owns Wholesale Medical & Surgical Suppliers of America, LLC in Flint, according to the indictment.
Seferovic would transfer stolen supplies to Khan during meetings in metro Detroit, including at a Walmart parking lot, according to the indictment. Khan, in turn, would sell the supplies and devices online at below retail price.
Seferovic’s job duties and status was unclear Thursday.
The investigation and alleged crimes have prompted internal changes at Beaumont.
“…Beaumont has enhanced security protocols and implemented additional checks and balances across the organization to reduce the chances of something like this happening again,” Geary said.
The Medicare Payment Advisory Commission voted Jan. 14 to recommend a 2 percent raise in Medicare payments for hospitals next year.
The commission said it wants to give the payment boost to both acute-care and long-term care hospitals. The 2 percent payment increase will result in about a $750 million to $2 billion increase in acute-care hospital spending for Medicare and about $50 million for long-term care hospitals.
MedPAC also plans to recommend no change to the payment rate for physicians in 2022 and a 5 percent decrease for home health firms and inpatient rehabilitation centers.
Although MedPAC will recommend the payment boost, Congress is not required to implement the recommendation.
The vote occurred at MedPAC’s January public meeting.
The annual J.P. Morgan Healthcare Conference is one of the best ways to diagnose the financial condition of the healthcare industry. Every January, every key stakeholder — providers, payers, pharmaceutical companies, tech companies, medical device and supply companies as well as bankers, venture capital and private equity firms — comes together in one exam room, even when it is virtual, for their annual check-up. But as we all know, this January is unlike any other as this past year has been unlike any other year.
You would have to go back to the banking crisis of 2008 to find a similar moment from an economic perspective. At the time, we were asking, “Are banks too big to fail?” The concern behind the question was that if they did fail, the economic chaos that would follow would lead to a collapse with the consumer ultimately picking up the tab. The rest is history.
Healthcare is “Too Vital to Fail”
2020 was historic in too many ways to count. But in a year when healthcare providers faced the worst financial crisis in the history of healthcare, the headline is that they are still standing. And what they proved is that in contrast to banks in 2008 that were seen by many as “too big to fail,” healthcare providers in 2020 proved that they were “too vital to fail.”
One of the many unique things about the COVID-19 pandemic is we are simultaneously experiencing a health crisis, where healthcare providers are the front line in the battle, and an economic crisis, felt in a big way in healthcare given the unique role hospitals play as the largest employer in most communities. Hospitals and health systems have done the vast majority of testing, treating, monitoring, counseling, educating and vaccinating all while searching for PPE and ventilators, and conducting clinical trials. And that’s just the beginning of the list.
Stop and think about that for a minute. What would we have done without them? Thinking through that question will give you some appreciation for the critical, challenging and central role that healthcare providers have had to play over the past year.
Simply stated, healthcare providers are the heart of healthcare, both clinically (essentially 100 percent of the care) and financially (over 50 percent of the $4 trillion annual spend on U.S. healthcare). Over the last year they stepped up and they stepped in at the moment where we needed them the most. This was despite the fact that, like most businesses, they were experiencing calamitous losses with no assurances of any assistance.
Healthcare is “Pandemic-Proof”
This was absolutely the worst-case scenario and the biggest test possible for our nation’s healthcare delivery system. Patient volume and therefore revenue dropped by over 50 percent when the panic of the pandemic was at its peak, driving over $60 billion in losses per month across hospitals and healthcare providers. At the same time, they were dramatically increasing their expenses with PPE, ventilators and additional staff. This was not heading in a good direction. While failure may not have been seen as an option, it was clearly a possibility.
The CARES Act clearly provided a temporary lifeline, providing funding for our nation’s hospitals to weather the storm. While there are more challenging times ahead, it is now clear that most are going to make it to the other side. The system of care in our country is often criticized, but when faced with perhaps the most challenging moment in the history of healthcare, our nation’s hospitals and health systems stepped up heroically and performed miraculously. The work of our healthcare providers on the front line and those who supported them was and is one thing that we all should be exceptionally proud of and thankful for.In 2020, they proved that not only is our nation’s healthcare system too vital to fail, but also that it is “pandemic proof.”
Listening to Front Line at the 2021 J.P. Morgan Healthcare Conference
There has never been a more important year to listen to the lessons from healthcare providers. They are and were the front line of our fight against COVID-19. If there was a class given about how to deal with a pandemic at an institutional level, this conference is where those lessons were being taught.
This year at the J.P. Morgan Healthcare Conference, CEOs, and CFOs from many of the most prestigious and most well-respected health systems in the world presented including AdventHealth, Advocate Aurora Health, Ascension, Baylor Scott & White Health, CommonSpirit Health, Henry Ford Health System, Intermountain Healthcare, Jefferson Health, Mass General Brigham, Northwell Health, OhioHealth, Prisma Health, ProMedica Health System, Providence, Spectrum Health and SSM Health.
I’ve been in healthcare for 30 years and this is my fifth year of writing up the summary of the non-profit provider track of the conference for Becker’s Healthcare to help share the wisdom of the crowd of provider organizations that share their stories. Clearly, this year was different and not because the presentations were virtual, but because they were inspirational.
What did we learn? The good news is that they have made many changes that have the potential to move healthcare in a much better direction and to get to a better place much faster. So, this year instead of providing you a nugget from each presentation, I am going to take a shot at summarizing what they collectively have in motion to stay vital after COVID.
10 Moves Healthcare Providers are Making to Stay Vital After-COVID
As a leader in healthcare, you will never have a bigger opportunity to drive change than right now. Smart leaders are framing this as essentially “before-COVID (BC)” and “after-COVID (AC)” and using this moment as their burning platform to drive change. Credit to the team at Providence for the acronym, but every CEO talked about this concept. As the saying goes, “never let a good crisis go to waste.” Well, we’ve certainly had a crisis, so here is a list of what the top health systems are doing to ensure that they don’t waste it and that they stay vital after-COVID:
1. Take Care of Your Team and They’ll Take Care of You: In a crisis, you can either come together as a team or fall apart. Clearly there has been a significant and stunning amount of pressure on healthcare providers. Many are fearing that mental health might be our nation’s next pandemic in the near future because they are seeing it right now with their own team. Perhaps one of their biggest lessons from this crisis has been the need to address the mental, physical and spiritual health of both team members as well as providers. They have put programs in place to help and have also built a tremendous amount of trust with their team by, in many cases, not laying off and/or furloughing employees. While they have made cuts in other areas such as benefits, this collective approach proved incredibly beneficial. And the last point here that relates to thinking differently about their team is that similar to other businesses, many health systems are making remote arrangements permanent for certain administrative roles and moving to a flexible approach regarding their team and their space in the future.
2. Focus on Health Equity, Not Just Health Care: This was perhaps the most notable and encouraging change from presentations in past years at J.P. Morgan. I have been going to the conference for over a decade, and I’ve never heard someone mention this term or outline their efforts on “health equity” — this year, nearly everyone did. In the past, they have outlined many wonderful programs on “social determinants of health,” but this year they have seen the disproportionate impact of COVID on low-income communities bringing the ongoing issue of racial disparities in access to care and outcomes to light. As the bedrock of employment in their community, this provides an opportunity to not just provide health care, but also health equity, taking an active role to help make progress on issues like hunger, homelessness, and housing. Many are making significant investments in a number of these and other areas.
3. Take the Lead in Public Health — the Message is the Medicine:One of the greatest failings of COVID, perhaps the greatest lesson learned, is the need for clear and consistent messaging from a public health perspective. That is a role that healthcare providers can and should play. In the pandemic, it represented the greatest opportunity to save lives as the essence of public health is communication — the message is the medicine. A number of health systems stepped into this opportunity to build trust and to build their brand, which are essentially one in the same. Some organizations have created a new role — a Chief Community Health Officer — which is a good way to capture the work that is in motion relative to social determinants of health as well as health equity. Many understand the opportunity here and will take the lead relative to vaccine distribution as clear messaging to build confidence is clearly needed.
4. Make the Home and Everywhere a Venue of Care:A number of presenters stated that “COVID didn’t change our strategy, it accelerated it.” For the most part, they were referring to virtual visits, which increased dramatically now representing around 10 percent of their visits vs. 1 percent before-COVID. One presenter said, “Digital has been tested and perfected during COVID,” but that is only considering the role we see digital playing in this moment. It is clear some organizations have a very narrow tactical lens while others are looking at the opportunity much more strategically. For many, they are looking at a “care anywhere and everywhere” strategy. From a full “hospital in the home” approach to remote monitoring devices, it is clear that your home will be seen as a venue of care and an access point moving forward. The pandemic of 2020 may have sparked a new era of “post-hospital healthcare” — stay tuned.
5. Bury Your Budget and Pivot to Planning:The budget process has been a source of incredible distrust, dissatisfaction and distraction for every health system for decades. The chaos and uncertainty of the pandemic forced every organization to bury their budget last year. With that said, many of the organizations that presented are now making a permanent shift away from a “budget-based culture” where the focus is on hitting a now irrelevant target set that was set six to nine months ago to a “performance-based culture” where the focus is on making progress every day, week, month and quarter. Given that the traditional annual operating budget process has been the core of how health systems have operated, this shift to a rolling forecast and a more dynamic planning process is likely the single most substantial and permanent change in how hospitals and health systems operate due to COVID. In other words, it is arguably a much bigger headline than what’s happened with virtual visits.
6. Get Your M&A Machine in Motion: It was clear from the presentations that activity around acquisitions is going to return, perhaps significantly. These organizations have strong balance sheets and while the strong have gotten stronger during COVID, the weak have in many cases gotten weaker. Many are going to be opportunistic to acquire hospitals, but at the same time they have concluded that they can’t just be a system of care delivery. They are also focused on acquiring and investing in other types of entities as well as forming more robust partnerships to create new revenue streams. Organizations that already had diversified revenue streams in place came through this pandemic the best. Most hospitals are overly reliant on the ED and surgical volume. Trying to drive that volume in a value-based world, with the end of site of service differentials and the inpatient only list, will be an even bigger challenge in the future as new niche players enter the market. As I wrote in the headline of my summary two years ago, “It’s the platform, stupid.” There are better ways to create a financial path forward that involve leveraging their assets — their platform — in new and creative ways.
7. Hey, You, Get into the Cloud:With apologies for wrapping a Rolling Stones song into a conference summary, one of the main things touted during presentations was “the cloud” and their ability to pull clinical, operational and financial dashboards together to monitor the impact of COVID on their organization and organize their actions. Focus over the last decade has been on the clinical (implementing EHRs), but it is now shifting to “digitizing operations” with a focus on finance and operations (planning, cost accounting, ERPs, etc.) as well as advanced analytics and data science capabilities to automate, gather insight, manage and predict. It is clear that the cloud has moved from a curiosity to a necessity for health systems, making this one of the biggest areas of investment for every health system over the next decade.
8. Make Price Transparency a Key Differentiator: One of the great lessons from Amazon (and others) is that you can make a lot of money when you make something easy to buy. While many health systems are skeptical of the value of the price transparency requirements, those that have a deep understanding of both their true cost of care and margins are using this as an opportunity to prove their value and accelerate their strategy to become consumer-centric. While there is certainly a level of risk, no business has ever been unsuccessful because they made their product easier to understand and access. Because healthcare is so opaque, there is an opening for healthcare providers to build trust, which is their main asset, and volume, which is their main source of revenue, by becoming stunningly easy to do business with. This may be tough sledding for some as this isn’t something healthcare providers are known for. To understand this, spend a few minutes on Tesla’s website vs. Ford’s. The concept of making something easy, or hard, to buy will become crystal clear as fast as a battery-driven car can go from zero to 60.
9. Make Care More Affordable:This represents the biggest challenge for hospitals and health systems as they ultimately need to be on the right side of this issue or the trust that they have will disappear and they will remain very vulnerable to outside players. All are investing in advanced cost accounting systems (time-driven costing, physician costing, supply, and drug costing) to truly understand their cost and use that as a basis to price more strategically in the market. Some are dropping prices for shoppable services and using loss leader strategies to build their brand. The incoming Secretary of Health and Human Services has a strong belief regarding the accountability of health systems to be consumer centric. The health systems that understand this are working to get ahead of this issue as it is likely one of their most significant threats (or opportunities) over the next decade. This means getting all care to the right site of care, evaluating every opportunity to improve, and getting serious about eliminating the need for expensive care through building healthy communities. If you’re worried about Wal-Mart or Amazon, this is your secret weapon to keep them on the sideline.
10. Scale = Survival: One of the big lessons here is that the strong got stronger, the weak got weaker. For the strong, many have been able to “snapback” in financial performance because they were resilient. They were able to designate COVID-only facilities, while keeping others running at a higher capacity. To be clear, while most health systems are going to get to the other side and are positioned better than ever, there are many others that will continue to struggle for years to come. According to our data at Strata, we see 25 percent operating at negative margins right now and another 50 percent just above breakeven. They key to survival moving forward, for those that don’t have a captive market, will be scale. If this pandemic proved one thing relative to the future of health systems it is this — scale equals survival.
When Will We Return to Normal?
Based on what the projections that these health systems shared, the “new normal” for health systems for the first half of 2021 will be roughly 95 percent of prior year inpatient volume with a 20 percent year-over-year drop in ED volume and a drop of 10-15 percent in observation visits. So, the pain will continue, but given the adjustments that were already made in 2020, it looks like they will be able to manage through COVID effectively. While there will be a pickup in the second half of 2021, the safe bet is that a “return to normal” pre-COVID volumes likely won’t occur until 2022. And there are some who believe that some of the volume should have never been there to begin with and we might see a permanent shift downward in ED volume as well as in some other areas.
With that said, I’ll steal a quote from Bert Zimmerli, the CFO of Intermountain Healthcare, who said, “Normal wasn’t ever nearly good enough in healthcare.”In that spirit, the goal should be to not return to normal, but rather to use this moment as an opportunity to take the positive changes driven by COVID — from technology to processes to areas of focus to a sense of responsibility — and make them permanent.
Thanking Our “Healthcare Heroes”
We’ll never see another 2020 again, hopefully. With that said, one of the silver linings of the year is everything we learned in healthcare. The most important lesson was this — in healthcare there are literally heroes everywhere. To each of them, I just want to say “thank you” for being there for us when we needed you the most. We should all be writing love letters to those on the front line who risked their lives to save others. Our nation’s healthcare system has taken a lot of criticism through the years from those on the outside, often with a blind eye to how things work in practice vs. in concept. But this year we all got to see first-hand what’s happening inside of healthcare — the heroic work of our healthcare providers and those who support them.
They faced the worst crisis in the history of healthcare. They responded heroically and were there for our families and friends.
They proved that healthcare is too vital to fail. They proved that healthcare is pandemic-proof.