

Relatively few Americans say they have been diagnosed with COVID-19 or tested positive for coronavirus antibodies, but many more believe they may have been infected or say they personally know someone who has been diagnosed.
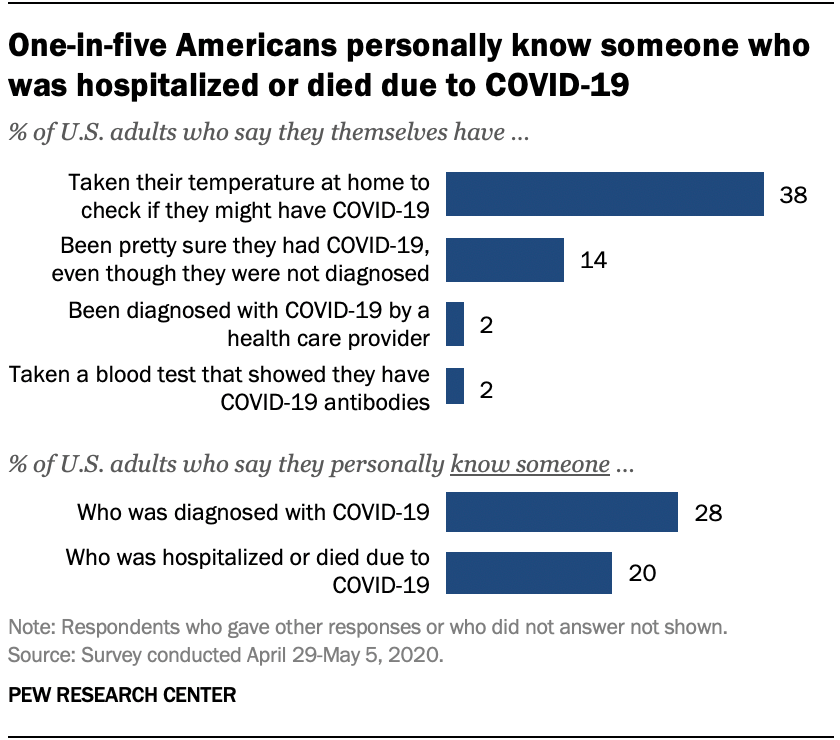
Only 2% of U.S. adults say they have been officially diagnosed with COVID-19 by a health care provider, according to a new Pew Research Center survey. And 2% say they have taken a blood test that showed they have COVID-19 antibodies, an indication that they previously had the coronavirus. But many more Americans (14%) say they are “pretty sure” they had COVID-19, despite not getting an official diagnosis. And nearly four-in-ten (38%) say they’ve taken their temperature to check if they might have the disease.
Although few Americans have been diagnosed with COVID-19 themselves, many more say they know someone with a positive diagnosis. More than one-in-four U.S. adults (28%) say they personally know someone who has been diagnosed by a health care provider as having COVID-19. A smaller share of Americans (20%) say they know someone who has been hospitalized or who has died as a result of having the coronavirus.
Some groups are more likely than others to report personal experiences with COVID-19. For instance, black adults are the most likely to personally know someone who has been hospitalized or died as a result of the disease. One-third of black Americans (34%) know someone who has been hospitalized or died, compared with 19% of Hispanics and 18% of white adults. Black Americans (32%) are also slightly more likely than Hispanic adults (26%) to know someone diagnosed with COVID-19. Public health studies have found black Americans are disproportionately dying or requiring hospitalization as a result of the coronavirus.

Areas in the northeastern United States have recorded some of the highest rates of coronavirus cases and fatalities, and this is reflected in the Center’s survey. About four-in-ten adults living in the Northeast (42%) say they personally know someone diagnosed with COVID-19, significantly more than among adults living in any other region. People living in the Northeast (31%) are also the most likely to know someone who has been hospitalized or died as a result of the disease.
One aspect of personal risk for exposure to the coronavirus is whether someone is employed in a setting where they must have frequent contact with other people, such as at a grocery store, hospital or construction site. Given the potential for the spread of the coronavirus within households, risk to individuals is also higher if other members of the household are employed in similar settings. Among people who are currently employed full-time, 35% are working in a job with frequent public contact. Among those working part-time, almost half work (48%) in such a setting. For those living in a household with other adults, 35% report that at least one of those individuals is working in a job that requires frequent contact with other people.
Taken together, nearly four-in-ten Americans (38%) have this type of exposure – either currently working in a job that requires contact with others, living in a household with others whose jobs require contact, or both.
Hispanics (at 48%) are more likely than either blacks (38%) or whites (35%) to have this type of personal or household exposure. An earlier Center analysis of government data found Hispanic adults were slightly more likely to work in service-sector jobs that require customer interaction, and that are at higher risk of layoffs as a result of the virus. In fact, the current Center survey found Hispanics were among the most likely to have experienced pay cuts or job losses due to the coronavirus outbreak.

Interpersonal exposure in the workplace is also more widespread among younger adults. And there is a 10 percentage point difference between upper- and lower-income Americans in exposure, with lower-income adults more likely to work in situations where they have to interact with the public, or to live with people who do.
Health experts warn that COVID-19 is particularly dangerous to people who have underlying medical conditions. In the survey, one-third of adults say they have such a condition. Among this group, nearly six-in-ten (58%) say that the coronavirus outbreak is a major threat to their personal health. Among those who do not report having an underlying medical condition, just 28% see the outbreak as a major threat to their health. Americans who have an underlying health condition are also more likely than those who do not to say they’ve taken their temperature to check if they might have COVID-19 (47% vs. 33% of those without a health condition).
Self-reports of an underlying health condition vary greatly by age. Among those ages 18 to 29, just 16% say they have a condition; this rises steadily with age to 56% among those 65 and older. Whites are a little more likely than blacks and Hispanics to report having a health condition, but both blacks (at 54%) and Hispanics (52%) are far more likely than whites (32%) to say that the coronavirus outbreak is “a major threat” to their health.
![]()
Some Workers Losing Jobs and Health Insurance Remain Ineligible for Subsidized Coverage.

The Issue
More than 70 percent of the 7.4 million workers with pre-pandemic employer-based insurance through industries now vulnerable to high rates of unemployment were found to be eligible for some assistance with health insurance (Medicaid or marketplace subsidies) if they lost their jobs. However, eligibility differs significantly between workers in states that have and have not expanded Medicaid.
Authors expand upon earlier work to show how varied levels of unemployment insurance provided through the Federal Pandemic Unemployment Compensation program affects eligibility for subsidized coverage.
Authors find that whether unemployment compensation is included in determining eligibility for Medicaid and Affordable Care Act (ACA) marketplace subsidies affects workers living in states that expanded Medicaid differently than those living in states that do not.
If the additional federal unemployment compensation was not used to determine eligibility for health insurance assistance, 78 percent of expansion state workers in the most vulnerable industries would be eligible for assistance compared to 59 percent of their counterparts in the 15 nonexpansion states.
Under current law, more than 70 percent of expansion and nonexpansion state workers with pre-pandemic employer-based insurance through industries now vulnerable to high rates of unemployment would be eligible for some assistance with health insurance if they lost their jobs.
Conclusion
The current limits on marketplace subsidies mean that fewer workers are likely to be eligible for financial assistance in getting or maintaining health insurance coverage. At the same time, additional funds could help them meet other pressing needs. This research suggests that eligibility for financial assistance above 400 percent of the federal poverty level under current rules would address this problem.
About the Urban Institute
The nonprofit Urban Institute is dedicated to elevating the debate on social and economic policy. For nearly five decades, Urban scholars have conducted research and offered evidence-based solutions that improve lives and strengthen communities across a rapidly urbanizing world. Their objective research helps expand opportunities for all, reduce hardship among the most vulnerable, and strengthen the effectiveness of the public sector. Visit the Urban Institute’s Health Policy Center for more information specific to its staff and its recent research.


Here are some significant developments:
https://www.healthcaredive.com/news/fitch-analysts-hospital-worries-FY-2020/577875/

From the Mayo Clinic to Kaiser Permanente, nonprofit hospitals are posting massive losses as the coronavirus pandemic upends their traditional way of doing business.
Fitch Ratings analysts predict a grimmer second quarter: “the worst on record for most,” Kevin Holloran, senior director for Fitch, said during a Tuesday webinar.
Over the past month, Fitch has revised its nonprofit hospital sector outlook from stable to negative. It has yet to change its ratings outlook to negative, though the possibility wasn’t ruled out.
Some have already seen the effects. Mayo estimates up to $3 billion in revenue losses from the onset of the pandemic until late April — given the system is operating “well below” normal capacity. It also announced employee furloughs and pay cuts, as several other hospitals have done.
Data released Tuesday from health cost nonprofit FAIR Health show how steep declines have been for larger hospitals in particular. The report looked at process claims for private insurance plans submitted by more than 60 payers for both nonprofit and for-profit hospitals.
Facilities with more than 250 beds saw average per-facility revenues based on estimated in-network amounts decline from $4.5 million in the first quarter of 2019 to $4.2 million in the first quarter of 2020. The gap was less pronounced in hospitals with 101 to 250 beds and not evident at all in those with 100 beds or fewer.
Funding from federal relief packages has helped offset losses at those larger hospitals to some degree.
Analysts from the ratings agency said those grants could help fill in around 30% to 50% of lost revenues, but won’t solve the issue on their own.
They also warned another surge of COVID-19 cases could happen as hospitals attempt to recover from the steep losses they felt during the first half of the year.
Anthony Fauci, the nation’s top infectious disease expert, warned lawmakers this week that the U.S. doesn’t have the necessary testing and surveillance infrastructure in place to prep for a fall resurgence of the coronavirus, a second wave that’s “entirely conceivable and possible.”
“If some areas, cities, states or what have you, jump over these various checkpoints and prematurely open up … we will start to see little spikes that may turn into outbreaks,” he told a Senate panel.
That could again overwhelm the healthcare system and financially devastate some on the way to recovery.
“Another extended time period without elective procedures would be very difficult for the sector to absorb,” Holloran said, suggesting if another wave occurs, such procedures should be evaluated on a case-by-case basis, not a state-by-state basis.
Hospitals in certain states and markets are better positioned to return to somewhat normal volumes later this year, analysts said, such as those with high growth and other wealth or income indicators. College towns and state capitols will fare best, they said.
Early reports of patients rescheduling postponed elective procedures provide some hope for returning to normal volumes.
“Initial expectations in reopened states have been a bit more positive than expected due to pent up demand,” Holloran said. But he cautioned there’s still a “real, honest fear about returning to a hospital.”
Moody’s Investors Service said this week nonprofit hospitals should expect the see the financial effects of the pandemic into next year and assistance from the federal government is unlikely to fully compensate them.
How quickly facilities are able to ramp up elective procedures will depend on geography, access to rapid testing, supply chains and patient fears about returning to a hospital, among other factors, the ratings agency said.
“There is considerable uncertainty regarding the willingness of patients — especially older patients and those considered high risk — to return to the health system for elective services,” according to the report. “Testing could also play an important role in establishing trust that it is safe to seek medical care, especially for nonemergency and elective services, before a vaccine is widely available.”
Hospitals have avoided major cash flow difficulties thanks to financial aid from the federal government, but will begin to face those issues as they repay Medicare advances. And the overall U.S. economy will be a key factor for hospitals as well, as job losses weaken the payer mix and drive down patient volumes and increase bad debt, Moody’s said.
Like other businesses, hospitals will have to adapt new safety protocols that will further strain resources and slow productivity, according to the report.
Another trend brought by the pandemic is a drop in ER volumes. Patients are still going to emergency rooms, FAIR Health data show, but most often for respiratory illnesses. Admissions for pelvic pain and head injuries, among others declined in March.
“Hospitals may also be losing revenue from a widespread decrease in the number of patients visiting emergency rooms for non-COVID-19 care,” according to the report. “Many patients who would have otherwise gone to the ER have stayed away, presumably out of fear of catching COVID-19.”
https://mailchi.mp/f4f55b3dcfb3/the-weekly-gist-may-15-2020?e=d1e747d2d8

Even after hearing dozens of reports from health systems about how steep their COVID-related volume losses have been, we were still floored by this analysis from healthcare analytics firm Strata Decision Technology, documenting a 55 percent drop in patients seeking hospital care across the country.
The report, which analyzed data from 228 hospitals in 51 health systems across 40 states, found that no clinical service line was immune from steep volume losses. The graphic below shows volume loss by service line in March-April 2020 compared to the same period in 2019.
Unsurprisingly, ophthalmology, gynecology, ortho/spine and ENT—all specialties with a high portion of elective cases, and heavily dependent on procedures—saw volume declines of greater than 70 percent. But even obstetrics and neonatology (which we expected to be “pandemic proof”) and infectious disease (which we thought might be busier in the throes of COVID-19) saw losses of 20-30 percent.
Looking at specific procedures, complex elective surgeries like spinal fusion and hip and knee replacements were almost completely obliterated. Precipitous declines in encounters for chronic diseases like coronary heart disease and diabetes (down 75 and 67 percent, respectively) and cancer screenings (a 55 percent decline in breast health and a 37 percent decline in cancer care overall) point to the likelihood of worrisome disease exacerbations, and a future full of more complex patients.
The volume losses, plus a 114 percent rise in uninsured patients, led to average two-week losses of $26.5M per health system across the study’s cohort. Strata will continue to track and publish volume changes, but this early snapshot paints a bleak picture of staggering financial hits, and “lost” patient care that will carry lasting ramifications for the health of communities nationwide.

Data: U.S. Employment and Training Administration via FRED; Chart: Andrew Witherspoon/Axios
Another 2.98 million Americans filed for unemployment last week, the Labor Department said on Thursday.
Why it matters: The coronavirus is still forcing a historically high number of Americans out of work. In two months alone, more than 36 million people have filed jobless claims.
Between the lines: The pace of new applications has slowed from its peak in March, but the weekly numbers are still way higher than before businesses shuttered to contain the outbreak.
By the numbers: The total number of people continuing to receive unemployment benefits — after initially applying — rose, bringing the total to a record 22.8 million.
The bottom line: Goldman Sachs estimates the unemployment rate will hit 25%, matching the peak level of joblessness during the Great Depression.
.png)
Private equity companies have spent millions in dark money to stall and effectively kill all versions of surprise billing reform. But this week, the issue will come before Congress again. Legislation was introduced Tuesday in the House that, among other things, would further assist hospitals with more relief funds. With this potential third disbursement of federal dollars comes an opportunity to finally address the embarrassing problem of surprise billing that has eroded the public trust in our great medical profession.
Physicians across the country are now signing a letter urging leaders of Congress to address surprise billing once and for all. I have already signed this letter and encourage you to consider doing so as well.
One reason the medical profession is the greatest profession in the world is that patients put their faith and trust in us. But 64% of Americans now say they have avoided or delayed medical care for fear of the bill. As more and more patients lose faith in the system, the doctor-patient relationship is being undermined by surprise billing and the modern-day business practices of price gouging and predatory billing. In fact, these egregious practices have become part of the business model of some private equity groups, which seek to replace physician autonomy with corporate medicine.
Our system today is unnecessarily complicated and works against patients’ interests by putting them in the middle of a finger-pointing blame game, which leaves them holding the bag. It doesn’t make sense for us to accept people with open arms, treat their ailment, and then ruin their lives financially. Medical science is a bastion of scientific and intellectual genius. We can fix this problem. Already, some efforts are advancing price transparency by creating a transparent marketplace for patients.
I’ve spent many years looking at the systematic cost issues that face our health system and patients. Simply put, the lack of fairness and transparency in pricing and billing practices has created financial toxicity and increased the general mistrust of the medical system for millions of Americans. No one designed it to be this bad. In fact, we have good people working in a bad system. When I explain details of pricing, billing, and collections with doctors and hospital leaders, they are invariably shocked and furious to learn how out of control their billing offices have gotten in overcharging patients and shaking people down for more than a reasonable amount for a service.
The current COVID-19 crisis is a stark reminder of the gaps in our health system that exacerbate the pressures facing providers and patients. Many Americans are getting crushed right now. Despite many years of debate in Washington and bipartisan agreement that something must be done, there is still no federal protection in place to safeguard consumers from an egregious surprise medical bill if they need emergency care or have limited options. The reality is that special interests — including the very private equity firms that stand to benefit financially from these exploitative business practices — continue to spend millions to maintain the status quo.
It’s time for a bipartisan compromise to end the non-transparent game of surprise medical billing. It’s time that Congress takes meaningful action to protect patients during this COVID-19 crisis and finally address this issue. Congress has solutions on the table that would bring much greater fairness and transparency to the healthcare system, protect patients from these predatory charges, and ensure that physicians are paid fairly for our services, as we deserve. It’s time we put an end to the cycle of financial toxicity and rebuild the great public trust in the medical profession.

