As COVID hospitalizations surge to new highs, healthcare workers have become the rate-limiting factor for most hospitals’ ability to deliver care. Using self-reported data collected by the Department of Health and Human Services, the graphic above shows that hospital staffing concerns reached an all-time high this month, with nearly one in three hospitals reporting a critical shortage. (Anecdotal evidence from our conversations with hospital leaders suggests that the actual number in crisis may be even higher, with every system we’ve spoken to in the past month reporting severe staffing challenges.)
During previous surges, COVID hospitalizations and reported staffing shortages have ebbed and flowed together. However, staffing challenges and case numbers became decoupled during the Delta surge, as the percentage of hospitals reporting staffing shortages did not go down as the Delta wave subsided.
With a growing number of nurses and other staff choosing early retirement or looking for jobs in other sectors, health systems are navigating the Omicron spike with a smaller pool of workers. And now the high transmissibility of the Omicron variant is forcinghealthcare workers to quarantine in droves.
As shown on the map, this is playing out both in highly vaccinated states like Vermont and California, and less-vaccinated places like West Virginia and Wyoming. That’s leading some state health officials and health systems to allow COVID-positive staff who are asymptomatic or experiencing mild symptoms to continue working—a policy which is being sharply criticized by nurses.
While the end of the Omicron surge should bring some relief, longer-term staffing challenges will surely remain for most health systems.
Some pundits claim that current reporting on COVID hospital admissions is overly pessimistic, failing to account for a distinction between patients admitted explicitly “for COVID”, and those admitted for other reasons who also, incidentally, have COVID. The latter now comprise up to half of some health systems’ COVID patients.
In an article in The Atlantic this week, reporter Ed Yong rejects this dichotomy, on the grounds that it ignores both the significant number of people for whom COVID exacerbates underlying chronic conditions, as well as the challenges any patient with COVID poses to hospitals. As he points out, those patients still require isolation and special safety measures, further worsening the burden on an already-strained staff.
The Gist: For hospitals, dealing with endemic COVID will mean establishing strategies to manage COVID-positive patients without postponing much needed non-emergency care, and without overly taxing a stretched workforce. Downplaying the burden of “incidental COVID” is not helpful, but sustaining operations while on perpetual crisis footing will prove untenable.
Every hospital in America has been affected by the growing shortage of nursing talent as the pandemic persists. This week a health system chief operating officer shared her greatest concern about the future of the nursing workforce: “We’re under immense pressure to find any nurses we can to keep units and operating rooms open. But if I think about the long-term impact, what I am most worried about is losing our most experienced nurses en masse.”
The average age of a nurse is 52, and 19 percent of nurses are over 65. Health systems have been facing a wave of retirements of Baby Boomer nurses, and the stresses of the pandemic, both in the workplace and at home, have dramatically accelerated the rate of tenured nurses leaving the profession, taking their well-honed clinical acumen with them.
“We’re looking at ways to increase the nursing pipeline, but you can’t replace a nurse with decades of experience one-to-one with someone just out of school, and expect the same level of clinical management, particularly for complex patients,” our COO colleague shared.
In the near term, her system is looking at two sets of strategies to maintain the nursing “brain trust”.
First, they hope to retain tenured nurses with job flexibility: “We’re not just losing nurses to retirement, we’re losing them to Siemens and Aetna—not because they are excited about that work, but because they don’t want to work a 12-hour shift. We have to be better about creating part-time, flexible schedules.”
Second, they are piloting telenursing and decision-support solutions to provide guidance and a second set of eyes for new nurses. These tools have also helped in new nurse recruitment. We’d predict the workforce crisis will persist far beyond the pandemic, and require rethinking of training, process automation, and the boundaries of practice license. But in the near-term, retaining and upskilling the talent we have is essential to maintaining access and quality.
The incredibly contagious new coronavirus variant is sidelining healthcare workers with breakthrough infections and quarantines, as patients flood into hospitals across the country. While hospitals are reporting that most infected patients are less sick, the sheer number of patients is pushing an already stressed system into crisis.
The Gist: Given mounting evidence that Omicron is both causing less severe disease and evading vaccines, health systems will need tobalance employee COVID testing and quarantine protocols against the constraints caused by mounting numbers of otherwise asymptomatic care workers out sick. As COVID becomes endemic, health systems must find a way to normalize operations even as they manage employee infections. It won’t be sustainable to continually revert to canceling non-emergent procedures (many of which carry clinical consequences to patients if they are delayed) and shifting to crisis standards of care.
While Omicron’s rapid spread is causing COVID hospitalizations to surge once again, the impact on consumer confidence may be different this time around. Drawing on the most recent data from analytics firm Strata Decision Technology, the graphic above shows how hospital volumes have fluctuated throughout the pandemic. Hospital volumes mostly returned to pre-COVID levels early last summer, until the Delta surge caused patients to begin avoiding care across all settings once again.
It remains to be seen if the forty percent of consumers who said they were less likely to seek non-emergency care during the Delta surge feel similarly about the Omicron spike. So far, consumer sentiment seems to be holding steady at last summer’s levels, though we’re still a few weeks away from Omicron’s expected peak.
As the pandemic enters its third year, it’s also likely that consumers who have been delaying care will simply be unwilling or unable to hold off any longer. But even if Omicron doesn’t dissuade consumers from seeking non-COVID care, health systems will be hard pressed to accommodate both COVID and non-COVID care amid worrisome staffing shortages.
Hospitals across the U.S. are feeling the wrath of the omicron variant and getting thrown into disarray that is different from earlier COVID-19 surges.
This time, they are dealing with serious staff shortages because so many health care workers are getting sick with the fast-spreading variant. People are showing up at emergency rooms in large numbers in hopes of getting tested for COVID-19, putting more strain on the system. And a surprising share of patients — two-thirds in some places — are testing positive while in the hospital for other reasons.
At the same time, hospitals say the patients aren’t as sick as those who came in during the last surge. Intensive care units aren’t as full, and ventilators aren’t needed as much as they were before.
The pressures are nevertheless prompting hospitals to scale back non-emergency surgeries and close wards, while National Guard troops have been sent in in several states to help at medical centers and testing sites.
Nearly two years into the pandemic, frustration and exhaustion are running high among health care workers.
“This is getting very tiring, and I’m being very polite in saying that,” said Dr. Robert Glasgow of University of Utah Health, which has hundreds of workers out sick or in isolation.
About 85,000 Americans are in the hospital with COVID-19, just short of the delta-surge peak of about 94,000 in early September, according to the Centers for Disease Control and Prevention. The all-time high during the pandemic was about 125,000 in January of last year.
But the hospitalization numbers do not tell the whole story. Some cases in the official count involve COVID-19 infections that weren’t what put the patients in the hospital in the first place.
Dr. Fritz François, chief of hospital operations at NYU Langone Health in New York City, said about 65% of patients admitted to that system with COVID-19 recently were primarily hospitalized for something else and were incidentally found to have the virus.
At two large Seattle hospitals over the past two weeks, three-quarters of the 64 patients testing positive for the coronavirus were admitted with a primary diagnosis other than COVID-19.
Joanne Spetz, associate director of research at the Healthforce Center at the University of California, San Francisco, said the rising number of cases like that is both good and bad.
The lack of symptoms shows vaccines, boosters and natural immunity from prior infections are working, she said. The bad news is that the numbers mean the coronavirus is spreading rapidly, and some percentage of those people will wind up needing hospitalization.
This week, 36% of California hospitals reported critical staffing shortages. And 40% are expecting such shortages.
Some hospitals are reporting as much as one quarter of their staff out for virus-related reasons, said Kiyomi Burchill, the California Hospital Association’s vice president for policy and leader on pandemic matters.
In response, hospitals are turning to temporary staffing agencies or transferring patients out.
University of Utah Health plans to keep more than 50 beds open because it doesn’t have enough nurses. It is also rescheduling surgeries that aren’t urgent. In Florida, a hospital temporarily closed its maternity ward because of staff shortages.
In Alabama, where most of the population is unvaccinated, UAB Health in Birmingham put out an urgent request for people to go elsewhere for COVID-19 tests or minor symptoms and stay home for all but true emergencies. Treatment rooms were so crowded that some patients had to be evaluated in hallways and closets.
As of Monday, New York state had just over 10,000 people in the hospital with COVID-19, including 5,500 in New York City. That’s the most in either the city or state since the disastrous spring of 2020.
New York City hospital officials, though, reported that things haven’t become dire. Generally, the patients aren’t as sick as they were back then. Of the patients hospitalized in New York City, around 600 were in ICU beds.
“We’re not even halfway to what we were in April 2020,” said Dr. David Battinelli, the physician-in-chief for Northwell Health, New York state’s largest hospital system.
Similarly, in Washington state, the number of COVID-19-infected people on ventilators increased over the past two weeks, but the share of patients needing such equipment dropped.
In South Carolina, which is seeing unprecedented numbers of new cases and a sharp rise in hospitalizations, Gov. Henry McMaster took note of the seemingly less-serious variant and said: “There’s no need to panic. Be calm. Be happy.”
Amid the omicron-triggered surge in demand for COVID-19 testing across the U.S., New York City’s Fire Department is asking people not to call for ambulance just because they are having trouble finding a test.
In Ohio, Gov. Mike DeWine announced new or expanded testing sites in nine cities to steer test-seekers away from ERs. About 300 National Guard members are being sent to help out at those centers.
In Connecticut, many ER patients are in beds in hallways, and nurses are often working double shifts because of staffing shortages, said Sherri Dayton, a nurse at the Backus Plainfield Emergency Care Center. Many emergency rooms have hours-long waiting times, she said.
“We are drowning. We are exhausted,” Dayton said.
Doctors and nurses are complaining about burnout and a sense their neighbors are no longer treating the pandemic as a crisis, despite day after day of record COVID-19 cases.
“In the past, we didn’t have the vaccine, so it was us all hands together, all the support. But that support has kind of dwindled from the community, and people seem to be moving on without us,” said Rachel Chamberlin, a nurse at New Hampshire’s Dartmouth-Hitchcock Medical Center.
Edward Merrens, chief clinical officer at Dartmouth-Hitchcock Health, said more than 85% of the hospitalized COVID-19 patients were unvaccinated.
Several patients in the hospital’s COVID-19 ICU unit were on ventilators, a breathing tube down their throats. In one room, staff members made preparations for what they feared would be the final family visit for a dying patient.
One of the unvaccinated was Fred Rutherford, a 55-year-old from Claremont, New Hampshire. His son carried him out of the house when he became sick and took him to the hospital, where he needed a breathing tube for a while and feared he might die.
If he returns home, he said, he promises to get vaccinated and tell others to do so too.
“I probably thought I was immortal, that I was tough,” Rutherford said, speaking from his hospital bed behind a window, his voice weak and shaky.
But he added: “I will do anything I can to be the voice of people that don’t understand you’ve got to get vaccinated. You’ve got to get it done to protect each other.”
At the 390-bed Terrace View nursing home on the east side of Buffalo, 22 beds are shut down. There isn’t enough staff to care for a full house, safely or legally.
That means some fully recovered patients in the adjacent Erie County Medical Center must stay in their hospital rooms, waiting for a bed in the nursing home. Which means some patients in the emergency department, who should be admitted to the hospital, must stay there until a hospital bed opens up. The emergency department becomes stretched so thin that 10 to 20 percent of arrivals leave without seeing a caregiver — after an average wait of six to eight hours, according to the hospital’s data.
“We used to get upset when our ‘left without being seen’ went above 3 percent,” said Thomas Quatroche, president and chief executive of the Erie County Medical Center Corp., which runs the 590-bed public safety net hospital.
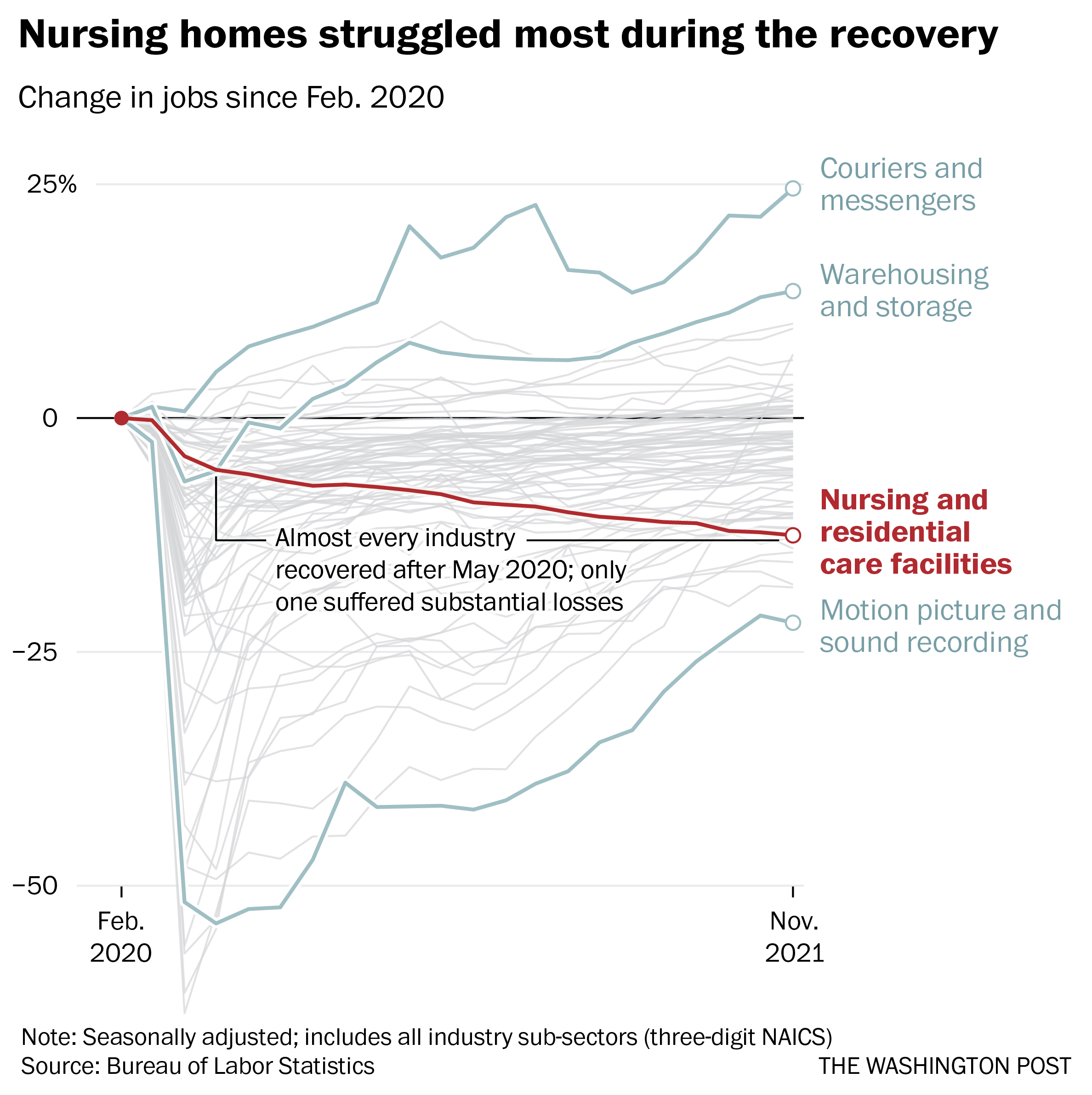
Nursing home bed and staff shortages were problems in the United States before the coronavirus pandemic. But the departure of 425,000 employees over the past two years has narrowed the bottleneck at nursing homes and other long-term care facilities at the same time that acute care hospitals are facing unending demand for services due to a persistent pandemic and staff shortages of their own.
With the omicron variant raising fears of even more hospitalizations, the problems faced by nursing homes are taking on even more importance. Several states have sent National Guard members to help with caregiving and other chores.
Hospitalizations, which peaked at higher than 142,000 in January, are rising again as well, reaching more than 71,000 nationally on Thursday, according to data tracked by The Washington Post. In some places, there is little room left in hospitals or ICUs.
About 58 percent of the nation’s 14,000 nursing homes are limiting admissions, according to a voluntary survey conducted by the American Health Care Association, which represents them. According to the U.S. Bureau of Labor Statistics, 425,000 employees, many of them low-paid certified nursing assistants who are the backbone of the nursing home workforce, have left since February 2020.
“What we’re seeing on the hospital side is a reflection of that,” said Rob Shipp, vice president for population health and clinical affairs at the Hospital Association of Pennsylvania, which represents medical providers in that state. The backups are not just for traditional medical inpatients ready for follow-up care, he said, but psychiatric and other patients as well.
A handful of developmentally disabled patients at Erie County Medical Center waited as long as a year for placement in a group setting, Quatroche said. Medical patients recovered from illness and surgery who cannot go home safely may wait days or weeks for a bed, he said.
“I don’t know if everyone understands how serious the situation is,” Quatroche said. “You really don’t know until you need care. And then you know immediately.”
Nearly 237,000 workers left during the recovery, data through November show. No other industry suffered anything close to those losses over the same period, according to the Bureau of Labor Statistics.
Workers in the broader health-care industry have been quitting in record numbers for most of the pandemic, plagued by burnout, vulnerability to the coronavirus and poaching by competitors. Low-wage workers tend to quit at the highest rates, Labor Department data show, and nursing home workers are the lowest paid in the health sector, with nonmanagerial earnings averaging between $17.45 an hour for assisted living to $21.19 an hour for skilled nursing facilities, according to the BLS.
Nursing home occupancy fell sharply at the start of the pandemic, but inched back upward in 2021, according to the nonprofit National Investment Center for Seniors Housing and Care. One major force that held it back was worker shortages.
“Operators in the business have said we could admit more patients, but we cannot find the staff to allow that to happen,” said Bill Kauffman, senior principal at the organization.
Shortages have spawned fierce talent wars in the industry, Brookdale Senior Living Chief Executive Officer Cindy Baier said in a recent earnings call. When they don’t have enough workers, restaurants can reduce service hours and hospitals can cut elective surgeries, but nursing homes don’t have the option of eliminating critical services, she said. They must close beds.
“We are in the ‘people taking care of people’ business around-the-clock, 365 days a year,” she said.
Nursing homes tend to gain workers during a recession but can struggle to hire during expansions, according to an analysis of county-level data from the Great Recession recently published in the health care provision and financing journal Inquiry.
Steady income from their resident population and government programs such as Medicaid makes them recession-proof, and their low pay and challenging work conditions mean they’re chronically understaffed, said one of the study’s authors, Indiana University health-care economist Kosali Simon.
When recessions occur, nursing homes go on a hiring spree, filling holes in their staff with qualified workers laid off elsewhere.
“People during a recession may lose their construction jobs or jobs in retail sectors, and then look for entry-level positions at places like nursing homes where there is always demand,” Simon said.
Now, amid the “Great Resignation” and the hot job market, the opposite is happening. In sparsely populated areas and regions where pay is lower, the problem is even worse.
The Diakonos Group, which operates 26 nursing homes, assisted-living facilities and group homes in Oklahoma, closed an 84-bed location for seniors with mental health needs in May “simply because we couldn’t staff it any longer,” said Chief Executive Officer Scott Pilgrim. Patients were transferred elsewhere, including Tulsa and Oklahoma City, he said.
The home in rural Medford, which depended entirely on Medicaid payments, “was never easy to staff, but once we started through covid and everything, our staff was just burned out.”
Diakonos boosted certified nursing assistants’ pay from $12 an hour and licensed practical nurses’ pay from $20 an hour, used federal and state assistance to offer bonuses and employed overtime, but workers kept leaving for better health-care jobs and positions in other industries, he said.
“I’ve never been able to pay what we ought to pay,” Pilgrim said. Eventually he began to limit admissions and eventually was forced to close.
“The hospitals are backed up,” he said. “They’re trying to find anywhere to send people. We get referrals from states all around us. The hospitals are desperate to find places to send people.”
In south central Pennsylvania, SpiriTrust Lutheran is not filling 61 of its 344 beds in six facilities because of the worker shortage, said Carol Hess, the company’s senior vice president.
“I have nurses who went to become real estate agents,” she said. “They were just burned out.”
Pay raises of $1 to $1.50 an hour and bonuses brought the lowest-paid workers to about $15 an hour, Hess said, and the company is planning a recruiting drive after Jan. 1. But the prognosis is still grim.
“We’re competing with restaurants for our dining team members,” Hess said. “We’re competing with other folks for cleaning and laundry and others.” In the area around Harrisburg where SpiriTrust employees live, some schools that turned out certified nurse assistants closed during the pandemic and haven’t reopened.
The nursing homes have begun borrowing licensed practical nurses from WellSpan Health, the nearby hospital system that discharges many of its patients to SpriTrust after they recover. About 15 have began their orientations this month, she said, and the two systems are collaborating to pay them.
The bed shortage is causing backups that can average several days in the hospital, said Michael Seim, the hospital system’s chief quality officer. That gives the hospitals an interest in helping any way they can, he said.
“We have between 80 and 100 patients waiting for some type of skilled care,” Seim said this month. The hospital has begun caring for more people at home, enrolling 400 people so far in a program that sends clinicians to check on them there. More than 90 percent have said they are happy with the program.
“I think the future of hospital-based care is partnerships,” Seim said. “It’s going to be health systems partnering across their service areas … to disrupt the model we have.”
For nearly two years, Americans have looked carefully at coronavirus case numbers in the country and in their local states and towns to judge the risk of the disease.
Surging case numbers signaled growing dangers, while falling case numbers were a relief and a signal to let one’s guard down in terms of gathering with friends and families and taking part in all kinds of events.
But with much of the nation’s population vaccinated and boosted and the country dealing with a new COVID-19 surge from omicron — a highly contagious variant that some studies suggest may not be as severe as previous variants — public health officials are debating whether the nation needs to shift its thinking.
Many people are going to get omicron — but those that are vaccinated and boosted are unlikely to suffer dire symptoms.
As a result, hospitalizations and deaths are the markers that government officials need to monitor carefully to ensure the safety of communities as the nation learns to live with COVID-19.
“This is the new normal,” said Leana Wen, a public health professor at George Washington University and former Baltimore health commissioner. “This is what we will have to accept as we transition from the emergency of COVID-19 to living with it as part of the new normal.”
David Dowdy, an epidemiologist at Johns Hopkins Bloomberg School of Public Health, said that Americans all need to shift to focus on hospitalizations over cases as we enter into another year of the pandemic.
“I think that we need to start training ourselves to look, first of all, at hospitalizations. I think hospitalizations are a real-time indicator of how serious things are,” he said.
Rising case numbers still say something about the disease, and the spikes from omicron are leading to real concerns.
Anthony Fauci, the government’s top infectious disease expert, noted on Sunday that even if omicron leads to less severe cases of COVID-19, if it infects tens of millions it will have the potential of straining resources in hospitals.
“If you have many, many, many more people with a less level of severity, that might kind of neutralize the positive effect of having less severity when you have so many more people,” he said during an appearance on ABC’s “This Week.”
At the same time, the nation must get used to dealing with the coronavirus as it would deal with an annual flu season. It’s a challenge for most parts of American life, from schools and businesses that have to consider worker and student safety, to professional sports leagues that must decide how long someone sits out after a positive test — even if the person is vaccinated and not symptomatic.
“Omicron in a way is the first test of what it means to live with COVID-19,” said Wen. “And by that I mean we are going to see many people getting infected but as long as our hospital systems are not overwhelmed and as long as vaccinated people are generally protected against severe outcomes, that is how we end the pandemic phase and switch into the endemic phase.”
The omicron strain is so infectious that once the current surge has faded in the United States, it’s likely a large majority of the population will either have been vaccinated against COVID-19 or have been infected, experts say. At that point, the focus should shift away from preventing infection to preventing serious illness, multiple experts said, a message already being echoed in some corners of the White House.
Many states have been seeing staggering numbers of positive tests and lines for COVID-19 testing that stretch for several blocks. Washington, D.C., and New York state have set records in recent days for the number of new cases reported as omicron barrels through the population.
But even with case totals surpassing last year’s numbers, President Biden and White House officials have been quick to point out that hospitalizations haven’t been as high as the numbers seen in the winter of 2020.
“Because we have so many vaccinated and boosted, we’re not seeing hospitalizations drive as sharply as we did in March of 2020 or even this past fall. America has made progress; things are better,” Biden said on Monday on a White House COVID-19 response team call with the National Governors Association to discuss the administration’s response to the omicron variant.
“But we do know that with rising cases, we still have tens of millions of unvaccinated people and we’re seeing hospitalizations rise,” he added, saying that some hospitals are going to get overrun both in terms of equipment and staff.
The White House pointed to Biden’s remarks last week when asked about whether the president wants Americans and health experts to take the emphasis off of case numbers and put it on hospitalizations.
“Because omicron spreads so easily, we’ll see some fully vaccinated people get COVID, potentially in large numbers. There will be positive cases in every office, even here in the White House, among the vaccinated … from omicron. But these cases are highly unlikely to lead to serious illness,” Biden said on Dec. 21.
Chief of staff Ron Klain on Monday retweeted a CNN report about how hospitalizations are about 70 percent less than what they were around the last peak in September, but that COVID-19 cases in unvaccinated Americans could end up overwhelming health systems.
Health experts have suggested the White House’s shift in messaging away from a focus on the number of cases is a sign of what’s to come as the pandemic eventually becomes endemic.
“For two years, infections always preceded hospitalizations which preceded deaths, so you could look at infections and know what was coming,” Ashish Jha, dean of the Brown University School of Public Health, said Sunday on ABC. “Omicron changes that. This is the shift we’ve been waiting for in many ways.”
Dowdy said positive tests are also up because people are getting tested before visiting relatives.
“If a lot of people are testing positive because they are asymptomatic and wanting to make sure that they can travel etc., having a lot of those kinds of cases is not a big problem,” he said.
“In fact, that’s a good thing. It means that we’re doing the right thing as a country to define those cases,” Dowdy added.
Lawrence Gostin, a professor of global health at Georgetown University, said the shift away from tracking case numbers as a way to measure the pandemic means devoting more resources toward treatment options like the Pfizer antiviral pill.
Gostin also said testing should increasingly be used to self-diagnose so individuals can get proper treatment, rather than testing for the purpose of stopping the spread of the virus.
“The White House has got a very difficult balancing act. Certainly for now it’s going to have to emphasize the idea of masking and distancing for the purpose of protecting the health system,” Gostin said.
“We can’t live our lives in a bubble to prevent us from getting a pathogen that’s so contagious that you can’t avoid it if you’re going to be circulating and living a life in this world,” he continued. “What it means to transition to a normal life or more normal life is you have to focus not so much on preventing cases, but on preventing hospitalizations and deaths.”
Another challenging year defined by the continued COVID-19 fight and vaccination drives has created a unique healthcare landscape. Pandemic-induced telehealth booms, continued strain due to understaffing and pressure from big tech disruptors are just some of the issues that have presented themselves this year.
Here are five major trends that hospitals and health systems may see in 2022. While some present challenges, others present significant opportunities for healthcare facilities.
Workforce pressure
Record numbers of workers have quit their jobs in 2021, with some 4.4 million people quitting in September. That means that 1 in 4 people quit their jobs this year across all industries. Around 1 in 5 healthcare workers have left their positions, creating issues with understaffing and lack of resources in hospitals and health systems. Stress, burnout and lack of balance have all been cited as reasons for staff leaving their roles. An increase in violence toward medical professionals, continued COVID-19 surges and low pay and benefits have contributed to the exodus of healthcare workers. None of those problems seems poised to disappear come 2022, so the new year could bring continued workforce and staffing challenges.
Pressure from disruptors
Big tech and retail giants have continued their push into healthcare this year. Companies like Apple, Amazon and Google stepped up their game in the wearables market. Pharmacy and retail chains Walmart and CVS Health both detailed their intended expansions into primary care. The pandemic also encouraged big corporations outside the healthcare sector, like Pepsi and Delta Airlines, to consider hiring CMOs to make sense of public health regulations guide them on their policy. These moves all mean there is a tightening of competition for the top physicians and hospital executives. Going into 2022, health systems may be under pressure to hang onto top talent and keep patients from using other convenient health services offered by retail giants.
Health equity
The unequal toll of the pandemic on people of color both medically and economically helped shed a light on the rampant inequities in American healthcare and society at large. Indigineous, Black and Hispanic people were much more likely than white or Asian people to suffer severe illness or require hospitalization as a result of COVID-19. Increasing numbers of hospitals, health systems and organizations are starting initiatives to advance health equity and focus on the socioeconomic drivers of health. The American Medical Association launched a language guide to encourage greater awareness about the power of language. Z-code usage has also been encouraged by CMS to increase knowledge and data about the social determinants of health. Next year, the perspective of health as holistic instead of just a part of an individual’s life will continue, with special attention being paid to social drivers.
Telehealth expansion
The pandemic helped the telemedicine industry take off in a big way. Telehealth was often the only healthcare option for many patients during the height of the lockdown measures introduced during the pandemic. Despite a return to in-person visits, telehealth has retained its popularity with patients. Some advocates argue that telehealth can help increase access to healthcare and improve health equity. About 40 percent of patients said that telehealth makes them more engaged and interact more frequently with their providers. However, while Americans see telehealth as the future of healthcare, a majority still prefer in-person visits. Regardless of patient opinion, telehealth will remain a key part of health strategy. In late December, the FCC approved $42.7 million in funding for telehealth for 68 healthcare providers. This suggests that there are investments and subsidies available in the future for health systems to bolster their telehealth services.
Climate change
At the 2021 UN Climate Conference, Cop26, in Glasgow, Scotland, hospitals and health systems acknowledged the role they have to play in mitigating the effects of climate change. Hospitals and health systems shed light on the health-related effects of climate change, such as illness and disease from events like wildfires and extreme weather. Health systems are also becoming more aware of their own contributions to climate change, with the U.S. healthcare system emitting 27 percent of healthcare emissions worldwide. To that end, HHS created an office of climate change and health equity that will work alongside regulators to reduce carbon emissions from hospitals. More health systems too are taking charge and pledging net neutrality and zero carbon emissions goals, including Kaiser Permanente and UnitedHealth group. It’s expected that more systems will follow suit in the coming year and make more concrete plans to address emissions reduction.
The healthcare industry’s staffing shortage crisis has had clear consequences for care delivery and efficiency, forcing some health systems to pause nonemergency surgeries or temporarily close facilities. Less understood is how these shortages are affecting care quality and patient safety.
A mix of high COVID-19 patient volume and staff departures amid the pandemic has put hospitals at the heart of a national staffing shortage, but there is little national data available to quantify the shortages’ effects on patient care.
The first hint came last month from a CDC report that found healthcare-associated infections increased significantly in 2020 after years of steady decline. Researchers attributed the increase to challenges related to the pandemic, including staffing shortages and high patient volumes, which limited hospitals’ ability to follow standard infection control practices.
“That’s probably one of the first real pieces of data — from a large scale dataset — that we’ve seen that gives us some sense of direction of where we’ve been headed with the impact of patient outcomes as a result of the pandemic,” Patricia McGaffigan, RN, vice president of safety programs for the Institute for Healthcare Improvement, told Becker’s. “I think we’re still trying to absorb much of what’s really happening with the impact on patients and families.”
An opaque view into national safety trends
Because of lags in data reporting and analysis, the healthcare industry lacks clear insights into the pandemic’s effect on national safety trends.
National data on safety and quality — such as surveys of patient safety culture from the Agency for Healthcare Research and Quality — can often lag by several quarters to a year, according to Ms. McGaffigan.
“There [have been] some declines in some of those scores more recently, but it does take a little while to be able to capture those changes and be able to put those changes in perspective,” she said. “One number higher or lower doesn’t necessarily indicate a trend, but it is worth really evaluating really closely.”
For example, 569 sentinel events were reported to the Joint Commission in the first six months of 2021, compared to 437 for the first six months of 2020. However, meaningful conclusions about the events’ frequency and long-term trends cannot be drawn from the dataset, as fewer than 2 percent of all sentinel events are reported to the Joint Commission, the organization estimates.
“We may never have as much data as we want,” said Leah Binder, president and CEO of the Leapfrog Group. She said a main area of concern is CMS withholding certain data amid the pandemic. Previously, the agency has suppressed data for individual hospitals during local crises, but never on such a wide scale, according to Ms. Binder.
CMS collects and publishes quality data for more than 4,000 hospitals nationwide. The data is refreshed quarterly, with the next update scheduled for October. This update will include additional data for the fourth quarter of 2020.
“It is important to note that CMS provided a blanket extraordinary circumstances exception for Q1 and Q2 2020 data due to the COVID-19 pandemic where data was not required nor reported,” a CMS spokesperson told Becker’s. “In addition, some current hospital data will not be publicly available until about July 2022, while other data will not be available until January 2023 due to data exceptions, different measure reporting periods and the way in which CMS posts data.”
Hospitals that closely monitor their own datasets in more near-term windows may have a better grasp of patient safety trends at a local level. However, their ability to monitor, analyze and interpret that data largely depends on the resources available, Ms. McGaffigan said. The pandemic may have sidelined some of that work for hospitals, as clinical or safety leaders had to shift their priorities and day-to-day activities.
“There are many other things besides COVID-19 that can harm patients,” Ms. Binder told Becker’s. “Health systems know this well, but given the pandemic, have taken their attention off these issues. Infection control and quality issues are not attended to at the level of seriousness we need them to be.”
What health systems should keep an eye on
While the industry is still waiting for definitive answers on how staffing shortages have affected patient safety, Ms. Binder and Ms. McGaffigan highlighted a few areas of concern they are watching closely.
The first is the effect limited visitation policies have had on families — and more than just the emotional toll. Family members and caregivers are a critical player missing in healthcare safety, according to Ms. Binder.
When hospitals don’t allow visitors, loved ones aren’t able to contribute to care, such as ensuring proper medication administration or communication. Many nurses have said they previously relied a lot on family support and vigilance. The lack of extra monitoring may contribute to the increasing stress healthcare providers are facing and open the door for more medical errors.
Which leads Ms. Binder to her second concern — a culture that doesn’t always respect and prioritize nurses. The pandemic has underscored how vital nurses are, as they are present at every step of the care journey, she continued.
To promote optimal care, hospitals “need a vibrant, engaged and safe nurse workforce,” Ms. Binder said. “We don’t have that. We don’t have a culture that respects nurses.”
Diagnostic accuracy is another important area to watch, Ms. McGaffigan said. Diagnostic errors — such as missed or delayed diagnoses, or diagnoses that are not effectively communicated to the patient — were already one of the most sizable care quality challenges hospitals were facing prior to the pandemic.
“It’s a little bit hard to play out what that crystal ball is going to show, but it is in particular an area that I think would be very, very important to watch,” she said.
Another area to monitor closely is delayed care and its potential consequences for patient outcomes, according to Ms. McGaffigan. Many Americans haven’t kept up with preventive care or have had delays in accessing care. Such delays could not only worsen patients’ health conditions, but also disengage them and prevent them from seeking care when it is available.
Reinvigorating safety work: Where to start
Ms. McGaffigan suggests healthcare organizations looking to reinvigorate their safety work go back to the basics. Leaders should ensure they have a clear understanding of what their organization’s baseline safety metrics are and how their safety reports have been trending over the past year and a half.
“Look at the foundational aspects of what makes care safe and high-quality,” she said. “Those are very much linked to a lot of the systems, behaviors and practices that need to be prioritized by leaders and effectively translated within and across organizations and care teams.”
She recommended healthcare organizations take a total systems approach to their safety work, by focusing on the following four, interconnected pillars:
Culture, leadership and governance
Patient and family engagement
Learning systems
Workforce safety
For example, evidence shows workforce safety is an integral part of patient safety, but it’s not an area that’s systematically measured or evaluated, according to Ms. McGaffigan. Leaders should be aware of this connection and consider whether their patient safety reporting systems address workforce safety concerns or, instead, add on extra work and stress for their staff.
Safety performance can slip when team members get busy or burdensome work is added to their plates, according to Ms. McGaffigan. She said leaders should be able to identify and prioritize the essential value-added work that must go on at an organization to ensure patients and families will have safe passage through the healthcare system and that care teams are able to operate in the safest and healthiest work environments.
In short, leaders should ask themselves: “What is the burdensome work people are being asked to absorb and what are the essential elements that are associated with safety that you want and need people to be able to stay on top of,” she said.
To improve both staffing shortages and quality of care, health systems must bring nurses higher up in leadership and into C-suite roles, Ms. Binder said. Giving nurses more authority in hospital decisions will make everything safer. Seattle-based Virginia Mason Hospital recently redesigned its operations around nurse priorities and subsequently saw its quality and safety scores go up, according to Ms. Binder.
“If it’s a good place for a nurse to go, it’s a good place for a patient to go,” Ms. Binder said, noting that the national nursing shortage isn’t just a numbers game; it requires a large culture shift.
Hospitals need to double down on quality improvement efforts, Ms. Binder said. “Many have done the opposite, for good reason, because they are so focused on COVID-19. Because of that, quality improvement efforts have been reduced.”
Ms. Binder urged hospitals not to cut quality improvement staff, noting that this is an extraordinarily dangerous time for patients, and hospitals need all the help they can get monitoring safety. Hospitals shouldn’t start to believe the notion that somehow withdrawing focus on quality will save money or effort.
“It’s important that the American public knows that we are fighting for healthcare quality and safety — and we have to fight for it, we all do,” Ms. Binder concluded. “We all have to be vigilant.”
Conclusion
The true consequences of healthcare’s labor shortage on patient safety and care quality will become clear once more national data is available. If the CDC’s report on rising HAI rates is any harbinger of what’s to come, it’s clear that health systems must place renewed focus and energy on safety work — even during something as unprecedented as a pandemic.
The irony isn’t lost on Ms. Binder: Amid a crisis driven by infectious disease, U.S. hospitals are seeing higher rates of other infections.
“A patient dies once,” she concluded. “They can die from COVID-19 or C. diff. It isn’t enough to prevent one.”