Congress returns from its July 4 break today and its focus will be on the President: will he resign or tough it out through the election in 120 days. But not everyone is paying attention to this DC drama.
In fact, most are disgusted with the performance of the political system and looking for something better. Per Gallup, trust and confidence in the U.S. Congress is at an all-time low.
The same is true of the healthcare system:
69% think it’s fundamentally flawed and in need of systemic change vs. 7% who think otherwise (Keckley Poll). And 60% think it puts its profits above all else, laying the blame at all its major players—hospitals, insurers, physician, drug companies and their army of advisors and suppliers.
These feelings are strongly shared by its workforce, especially the caregivers and support personnel who service patient in hospital, clinic and long-term care facilities. Their ranks are growing, but their morale is sinking.
Career satisfaction among clinical professionals (nurses, physicians, dentists, counselors) is at all time low and burnout is at an all-time high.
Last Friday, the Bureau of Labor issued its June 2024 Jobs report. To no one’s surprise, job growth was steady (+206,000 for the month) –slightly ahead of its 3-month average (177,000) despite a stubborn inflation rate that’s hovered around 3.3% for 15 months. Healthcare providers accounted for 49,000 of those jobs–the biggest non-government industry employer.
But buried in the detail is a troubling finding: for hospital employment (NAICS 6221.3): productivity was up 5.9%, unit labor costs for the month were down 1.1% and hourly wages grew 4.8%–higher than other healthcare sectors.
For the 4.7 million rank and file directly employed in U.S. hospitals, these productivity gains are interpreted as harder work for less pay. Their wages have not kept pace with their performance improvements while executive pay seems unbridled.
Next weekend, the American Hospital Association will host its annual Leadership Summit in San Diego: 8 themes are its focus:
Building a More Flexible and Sustainable Workforce is among them. That’s appropriate and it’s urgent.
An optimistic view is that emergent technologies and AI will de-lever hospitals from their unmanageable labor cost spiral. Chief Human Resource Officers doubt it. Energizing and incentivizing technology-enabled self-care, expanding scope of practice opportunities for mid-level professionals and moving services out of hospitals are acknowledged keys, but guilds that protect licensing and professional training push back.
By contrast, the application of artificial intelligence to routine administrative tasks is more promising: reducing indirect costs (overhead) that accounts for a third of total spending is the biggest near-term opportunity and a welcome focus to payers and consumers.
Thus, most organizations advance workforce changes cautiously. That’s the first problem.
The second problem is this:
lack of a national healthcare workforce modernization strategy to secure, prepare and equip the health system to effectively perform. Section V of the Affordable Care Act (March 2010) authorized a national workforce commission to modernize the caregiver workforce. Due to funding, it was never implemented. It’s needed today more than ever. The roles of incentives, technologies, AI, data and clinical performance measurement were not considered in the workforce’ ACA charter: Today, they’re vital.
Transformational changes in how the healthcare workforce is composed, evaluated and funded needs fresh thinking and boldness. It must include input from new players and disavow sacred cows. It includes each organization’s stewardship and a national spotlight on modernization.
It’s easier to talk about healthcare’s workforce issues but It’s harder to fix them. That’s why incrementalism is the rule and transformational change just noise.
PS: In doing research for this report, I found wide variance in definitions and counts for the workforce. It may be as high as 24 million, and that does not include millions of unpaid caregivers. All the more reason to urgently address its modernization.
Chronic disinvestment and inadequate training have created a shortage of primary care workers.
As the presidential election nears, issues from the economy to climate change are vying for airtime, yet markedly absent from the headlines is a deepening crisis that threatens the future health and wellbeing of communities nationwide: a primary care sector on the brink of collapse.
Primary care is the cornerstone of community health. It helps us live longer lives, prevents disease and reduces health disparities. It is indispensable to strengthening our nation’s ability to withstand another deadly pandemic or climate disaster. And yet, over 100 million Americans report they lack access to a regular doctor or source of care.
Physicians and patients acutely feel the primary care workforce shortage. In recent interviews we heard an alarming refrain from clinicians and health executives: “I could spend all my time helping friends find doctors accepting new patients.” Another said, “I have 100 open staff positions and am in a bidding war for primary care physicians.”
Just in the past decade, there has been a 36% jump in the share of U.S. children without a usual source of care. Among adults it’s a 21% increase, according to a Milbank report.And with America’s rapidly aging population, access to critical primary care services is only expected to get worse.
Understanding what’s driving America’s primary care workforce shortage is key to finding effective, long-term solutions.
A workforce exodus amid chronic disinvestment
America is not producing enough primary care physicians to meet growing population needs. New primary care physicians are leaving for other fields at alarming rates. In 2021, only 15% of all physicians were practicing outpatient primary care three to five years after residency, according to a Milbank report.
When we look at the disparities in compensation rates and the nation’s chronic disinvestment in primary care, this workforce exodus shouldn’t come as a surprise. Specialists in the U.S. now routinely make two to three times what their primary care colleagues do, creating powerful incentives for physicians in training to “go for the gold.”
Primary care accounts for 35% of healthcare visits but receives only about 5% to 7% of total healthcare expenditures. For context, hospitals account for 30% of healthcare expenditures.Additionally, since 2019, the share of total spending by Medicare, Medicaid and commercial insurers in primary care has steadily declined; Medicare’s share has dropped by 15%, according to Milbank.
Inadequate training, disparities in access
Today, the vast majority of primary care residents train within hospitals and academic health centers, which do not expose them to the needs of underserved communities, nor provide them with the skills needed to successfully practice in challenging, real-world clinical environments. In 2021, only 15% of primary care residents spent a majority of their time training in community settings, outside of hospitals.
Moving forward, the solutions are clear. Congress and both the public and private sectors must work together to enact stronger federal and state policies in three critical primary care areas. First, Medicare and Medicaid physician reimbursement — which has led to our specialty-dominated healthcare system — must become more effective and efficient. We know that inadequate compensation is one reason why many medical students choose not to go into primary care.
Second, the billions in public dollars going to clinician training must be focused on creating a highly skilled primary care workforce with practical experience in community settings. This is essential to meet the complex health needs of our nation’s ever-changing and growing population.
And finally, we need to expand the footprint of community health centers, the linchpin to improving health outcomes in underserved communities. Currently, these centers provide care to 1 in 11 patients around the country, but that number needs to be vastly expanded.
It’s time to strengthen our fragile primary care system to ensure it delivers the comprehensive, affordable care Americans so desperately need. Access to high-quality primary care for everyone should not be an aspiration, but an expectation that we – as a nation – have an urgent duty to fulfill.
The U.S. health system has experienced three major shifts since the pandemic that set the stage for its future:
From trust to distrust: Every poll has chronicled the decline in trust and confidence in government: Congress, the Presidency, the FDA and CDC and even the Supreme Court are at all-time lows. Thus, lawmaking about healthcare is met with unusual hostility.
From big to bigger: The market has consistently rewarded large cap operators, giving advantage to national and global operators in health insurance, information technology and retail health. In response, horizontal consolidation via mergers and acquisitions has enabled hospitals, medical practices, law firms and consultancies to get bigger, attracting increased attention from regulators. Access to private capital and investor confidence is a major differentiator for major players in each sector.
From regulatory tailwinds to headwinds: in the last 3 years, regulators have forced insurers, hospitals and drug companies to disclose prices and change business practices deemed harmful to fair competition and consumer choice. Incumbent-unfriendly scrutiny has increased at both the state and federal levels including notable bipartisan support for industry-opposed legislation. It will continue as healthcare favor appears to have run its course.
Some consider these adverse; others opportunistic; all consider them profound. All concede the long-term destination of the U.S. health system is unknown. Against this backdrop, 2024 is about safe bets.
These 10 themes will be on the agenda for every organization operating in the $4.5 trillion U.S. healthcare market:
Not for profit health: “Not-for-profit” designation is significant in healthcare and increasingly a magnet for unwelcome attention. Not-for-profit hospitals, especially large, diversified multi-hospital systems, will face increased requirements to justify their tax exemptions. Special attention will be directed at non-operating income activities involving partnerships with private equity and incentives used in compensating leaders. Justification for profits will take center stage in 2024 with growing antipathy toward organizations deemed to put profit above all else.
Insurer coverage and business practices: State and federal regulators will impose regulatory constraints on insurer business practices that lend to consumer and small-business affordability issues.
Workforce wellbeing: The pandemic hangover, sustained impact of inflation on consumer prices, increased visibility of executive compensation and heightened public support for the rank-and-file workers and means wellbeing issues must be significant in 2024.
Board effectiveness: The composition, preparedness, compensation and independent judgement of Boards will attract media scrutiny; not-for-profit boards will get special attention in light of 2023 revelations in higher education.
Employer-sponsored health benefits: The cost-effectiveness of employee health benefits coverage will prompt some industries and large, self-insured companies to pursue alternative strategies for attracting and maintaining a productive workforce. Direct contracting, on-site and virtual care will be key elements.
Physician independence: With 20% of physicians in private equity-backed groups, and 50% in hospital employed settings, ‘corporatization’ will encounter stiff resistance from physicians increasingly motivated to activism believing their voices are unheard.
Data driven healthcare: The health industry’s drive toward interoperability and transparency will will force policy changes around data (codes) and platform ownership, intellectual property boundaries, liability et al. Experience-based healthcare will be forcibly constrained by data-driven changes to processes and insights.
Consolidation: The DOJ and FTC will expand their activism against vertical and horizontal consolidation that result in higher costs for consumers. Retrospective analyses of prior deals to square promises and actual results will be necessary.
Public health: State and federal funding for public health programs that integrate with community-based health providers will be prioritized. The inadequacy of public health funding versus the relative adequacy of healthcare’s more lucrative services will be the centerpiece for health reforms.
ACO 2.0: In Campaign 2024, abortion and the Affordable Care Act will be vote-getters for candidates favoring/opposing current policies. Calls to “Fix and Repair” the Affordable Care Act will take center stage as voters’ seek affordability and access remedies.
Every Board and C suite in U.S. healthcare will face these issues in 2024.
Health systems are recovering from the worst financial year in recent history. We surveyed strategic planners to find out their top priorities for 2024 and where they are focusing their energy to achieve growth and sustainability. Read on to explore the top six findings from this year’s survey.
Research questions
With this survey, we sought the answers to five key questions:
How do health system margins, volumes, capital spending, and FTEs compare to 2022 levels?
How will rebounding demand impact financial performance?
How will strategic priorities change in 2024?
How will capital spending priorities change next year?
Bigger is Better for Financial Recovery
What did we find?
Hospitals are beginning to recover from the lowest financial points of 2022, where they experienced persistently negative operating margins. In 2023, the majority of respondents to our survey expected positive changes in operating margins, total margins, and capital spending. However, less than half of the sample expected increases in full-time employee (FTE) count. Even as many organizations reported progress in 2023, challenges to workforce recovery persisted.
40%
Of respondents are experiencing margins below 2022 levels
Importantly, the sample was relatively split between those who are improving financial performance and those who aren’t. While 53% of respondents projected a positive change to operating margins in 2023, 40% expected negative changes to margin.
One exception to this split is large health systems. Large health systems projected above-average recovery of FTE counts, volume, and operating margins. This will give them a higher-than-average capital spending budget.
Why does this matter?
These findings echo an industry-wide consensus on improved financial performance in 2023. However, zooming in on the data revealed that the rising tide isn’t lifting all boats. Unequal financial recovery, especially between large and small health systems, can impact the balance of independent, community, and smaller providers in a market in a few ways. Big organizations can get bigger by leveraging their financial position to acquire less resourced health systems, hospitals, or provider groups. This can be a lifeline for some providers if the larger organization has the resources to keep services running. But it can be a critical threat to other providers that cannot keep up with the increasing scale of competitors.
Variation in financial performance can also exacerbate existing inequities by widening gaps in access. A key stakeholder here is rural providers. Rural providers are particularly vulnerable to financial pressures and have faced higher rates of closure than urban hospitals. Closures and consolidation among these providers will widen healthcare deserts. Closures also have the potential to alter payer and case mix (and pressure capacity) at nearby hospitals.
Volumes are decoupled from margins
What did we find?
Positive changes to FTE counts, reduced contract labor costs, and returning demand led the majority of respondents in our survey to project organizational-wide volume growth in 2023. However, a significant portion of the sample is not successfully translating volume growth to margin recovery.
44%
Of respondents who project volume increases also predict declining margins
On one hand, 84% of our sample expected to achieve volume growth in 2023. And 38% of respondents expected 2023 volume to exceed 2022 volume by over 5%. But only 53% of respondents expected their 2023 operating margins to grow — and most of those expected that the growth would be under 5%. Over 40% of respondents that reported increases in volume simultaneously projected declining margins.
Why does this matter?
Health systems struggled to generate sufficient revenue during the pandemic because of reduced demand for profitable elective procedures. It is troubling that despite significant projected returns to inpatient and outpatient volumes, these volumes are failing to pull their weight in margin contribution. This is happening in the backdrop of continued outpatient migration that is placing downward pressure on profitable inpatient volumes.
There are a variety of factors contributing to this phenomenon. Significant inflationary pressures on supplies and drugs have driven up the cost of providing care. Delays in patient discharge to post-acute settings further exacerbate this issue, despite shrinking contract labor costs. Reimbursements have not yet caught up to these costs, and several systems report facing increased denials and delays in reimbursement for care. However, there are also internal factors to consider. Strategists from our study believe there are outsized opportunities to make improvements in clinical operational efficiency — especially in care variation reduction, operating room scheduling, and inpatient management for complex patients.
Strategists look to technology to stretch capital budgets
What did we find?
Capital budgets will improve in 2024, albeit modestly. Sixty-three percent of respondents expect to increase expenditures, but only a quarter anticipate an increase of 6% or more. With smaller budget increases, only some priorities will get funded, and strategists will have to pick and choose.
Respondents were consistent on their top priority. Investments in IT and digital health remained the number one priority in both 2022 and 2023. Other priorities shifted. Spending on areas core to operations, like facility maintenance and medical equipment, increased in importance. Interest in funding for new ambulatory facilities saw the biggest change, falling down two places.
Why does this matter?
Capital budgets for health systems may be increasing, but not enough. With the high cost of borrowing and continued uncertainty, health systems still face a constrained environment. Strategists are looking to get the biggest bang for their buck. Technology investments are a way to do that. Digital solutions promise high impact without the expense or risk of other moves, like building new facilities, which is why strategists continue to prioritize spending on technology.
The value proposition of investing in technology has changed with recent advances in artificial intelligence (AI), and our respondents expressed a high level of interest in AI solutions. New applications of AI in healthcare offer greater efficiencies across workforce, clinical and administrative operations, and patient engagement — all areas of key concern for any health system today.
Building is reserved for those with the largest budgets
What did we find?
Another way to stretch capital budgets is investing in facility improvements rather than new buildings. This allows health systems to minimize investment size and risk. Our survey found that, in general, strategists are prioritizing capital spending on repairs and renovation while deprioritizing building new ambulatory facilities.
When the responses to our survey are broken out by organization type, a different story emerges. The largest health systems are spending in ways other systems are not. Systems with six or more hospitals are increasing their overall capital expenditures and are planning to invest in new facilities. In contrast, other systems are not increasing their overall budgets and decreasing investments in new facilities.
AMCs are the only exception. While they are decreasing their overall budget, they are increasing their spending on new inpatient facilities.
Why does this matter?
Health systems seek to attract patients with new facilities — but only the biggest systems can invest in building outpatient and inpatient facilities. The high ranking of repairs in overall capital expenditure priorities suggests that all systems are trying to compete by maintaining or improving their current facilities. Will renovations be enough in the face of expanded building from better financed systems? The urgency to respond to the pandemic-accelerated outpatient shift means that building decisions made today, especially in outpatient facilities, could affect competition for years to come. And our survey responses suggest that only the largest health system will get the important first-mover advantage in this space.
AMCs are taking a different tack in the face of tight budgets and increased competition. Instead of trying to compete across the board, AMCs are marshaling resources for redeployment toward inpatient facilities. This aligns with their core identity as a higher acuity and specialty care providers.
Partnerships and affiliations offer potential solutions for health systems that lack the resources for building new facilities. Health systems use partnerships to trade volumes based on complexity. Partnerships can help some health systems to protect local volumes while still offering appropriate acute care at their partner organization. In addition, partnerships help health systems capture more of the patient journey through shared referrals. In both of these cases, partnerships or affiliations mitigate the need to build new inpatient or outpatient facilities to keep patients.
Eighty percent of respondents to our survey continued to lose patient volumes in 2023. Despite this threat to traditional revenue, health systems are turning from revenue diversification practices. Respondents were less likely to operate an innovation center or invest in early-stage companies in 2023. Strategists also reported notably less participation in downside risk arrangements, with a 27% decline from 2022 to 2023.
Why does this matter?
The retreat from revenue diversification and risk arrangements suggests that health systems have little appetite for financial uncertainty. Health systems are focusing on financial stabilization in the short term and forgoing practices that could benefit them, and their patients, in the long term.
Strategists should be cautious of this approach. Retrenchment on innovation and value-based care will hold health systems back as they confront ongoing disruption. New models of care, patient engagement, and payment will be necessary to stabilize operations and finances. Turning from these programs to save money now risks costing health systems in the future.
Market intelligence and strategic planning are essential for health systems as they navigate these decisions. Holding back on initiatives or pursuing them in resource-constrained environments is easier when you have a clear course for the future and can limit reactionary cuts.
Advisory Board’s long-standing research on developing strategy suggests five principles for focused strategy development:
Strategic plans should confront complexity. Sift through potential future market disruptions and opportunities to establish a handful of governing market assumptions to guide strategy.
Ground strategy development in answers to a handful of questions regarding future competitive advantage. Ask yourself: What will it take to become the provider of choice?
Communicate overarching strategy with a clear, coherent statement that communicates your overall health system identity.
A strategic vision should be supported by a limited number of directly relevant priorities. Resist the temptation to fill out “pro forma” strategic plan.
Pair strategic priorities with detailed execution plans, including initiative roadmaps and clear lines of accountability.
Strategists align on a strategic vision to go back to basics
What did we find?
Despite uneven recovery, health systems widely agree on which strategic initiatives they will focus more on, and which they will focus less on. Health system leaders are focusing their attention on core operations — margins, quality, and workforce — the basics of system success. They aim to achieve this mandate in three ways. First, through improving efficiency in care delivery and supply chain. Second, by transforming key elements of the care delivery system. And lastly, through leveraging technology and the virtual environment to expand job flexibility and reduce administrative burden.
Health systems in our survey are least likely to take drastic steps like cutting pay or expensive steps like making acquisitions. But they’re also not looking to downsize; divesting and merging is off the table for most organizations going into 2024.
Why does this matter?
The strategic priorities healthcare leaders are working toward are necessary but certainly not easy. These priorities reflect the key challenges for a health system — margins, quality, and workforce. Luckily, most of strategists’ top priorities hold promise for addressing all three areas.
This triple mandate of improving margins, quality, and workforce seems simple in theory but is hard to get right in practice. Integrating all three core dimensions into the rollout of a strategic initiative will amplify that initiative’s success. But, neglecting one dimension can diminish returns. For example, focusing on operational efficiency to increase margins is important, but it’ll be even more effective if efforts also seek to improve quality. It may be less effective if you fail to consider clinicians’ workflow.
Health systems that can return to the basics, and master them, are setting a strong foundation for future growth. This growth will be much more difficult to attain without getting your house in order first.
Vendors and other health system partners should understand that systems are looking to ace the basics, not reinvent the wheel. Vendors should ensure their products have a clear and provable return on investment and can map to health systems’ strategic priorities. Some key solutions health systems will be looking for to meet these priorities are enhanced, easy-to-follow data tools for clinical operations, supply chain and logistics, and quality. Health systems will also be interested in tools that easily integrate into provider workflow, like SDOH screening and resources or ambient listening scribes.
Going back to basics
Craft your strategy
1. Rebuild your workforce.
One important link to recovery of volume is FTE count. Systems that expect positive changes in FTEs overwhelmingly project positive changes in volume. But, on average, less than half of systems expected FTE growth in 2023. Meanwhile, high turnover, churn, and early retirement has contributed to poor care team communication and a growing experience-complexity gap. Prioritize rebuilding your workforce with these steps:
Recover: Ensure staff recover from pandemic-era experiences by investing in workforce well-being. Audit existing wellness initiatives to maximize programs that work well, and rethink those that aren’t heavily utilized.
Recruit: Compete by addressing what the next generation of clinicians want from employment: autonomy, flexibility, benefits, and diversity, equity, and inclusion (DEI). Keep up to date with workforce trends for key roles such as advance practice providers, nurses, and physicians in your market to avoid blind spots.
Retain: Support young and entry-level staff early and often while ensuring tenured staff feel valued and are given priority access to new workforce arrangements like hybrid and gig work. Utilize virtual inpatient nurses and virtual hubs to maintain experienced staff who may otherwise retire. Prioritize technologies that reduce the burden on staff, rather than creating another box to check, like ambient listening or asynchronous questionnaires.
2. Become the provider of choice with patient-centric care.
Becoming the provider of choice is crucial not only for returning to financial stability, but also for sustained growth. To become the provider of choice in 2024, systems must address faltering consumer perspectives with a patient-centric approach. Keep in mind that our first set of recommendations around workforce recovery are precursors to improving patient-centered care. Here are two key areas to focus on:
Front door: Ensure a multimodal front door strategy. This could be accomplished through partnership or ownership but should include assets like urgent care/extended hour appointments, community education and engagement, and a good digital experience.
Social determinants of health: A key aspect of patient-centered care is addressing the social needs of patients. Our survey found that addressing SDOH was the second highest strategic priority in 2023. Set up a plan to integrate SDOH screenings early on in patient contact. Then, work with local organizations and/or build out key services within your system to address social needs that appear most frequently in your population. Finally, your workforce DEI strategy should focus on diversity in clinical and leadership staff, as well as teaching clinicians how to practice with cultural humility.
3. Recouple volume and margins.
The increasingly decoupled relationship between volume and margins should be a concern for all strategists. There are three parts to improving volume related margins: increasing volume for high-revenue procedures, managing costs, and improving clinical operational efficiency.
Revenue growth: Craft a response to out-of-market travel for surgery. In many markets, the pool of lucrative inpatient surgical volumes is shrinking. Health systems are looking to new markets to attract patients who are willing to travel for greater access and quality. Read our findings to learn more about what you need to attract and/or defend patient volumes from out-of-market travel.
Cost reduction: Although there are many paths health systems can take to manage costs, focusing on tactics which are the most likely to result in fast returns and higher, more sustainable savings, will be key. Some tactics health systems can deploy include preventing unnecessary surgical supply waste, making employees accountable for their health costs, and reinforcing nurse-led sepsis protocols.
Clinical operational efficiency: The number one strategic priority in 2023, according to our survey, was clinical operational efficiency, no doubt in response to faltering margins. Within this area, the top place for improvement was care variation reduction (CVR). Ensure you’re making the most out of CVR efforts by effectively prioritizing where to spend your time. Improve operational efficiency outside of CVR by improving OR efficiency and developing protocols for complex inpatient management.
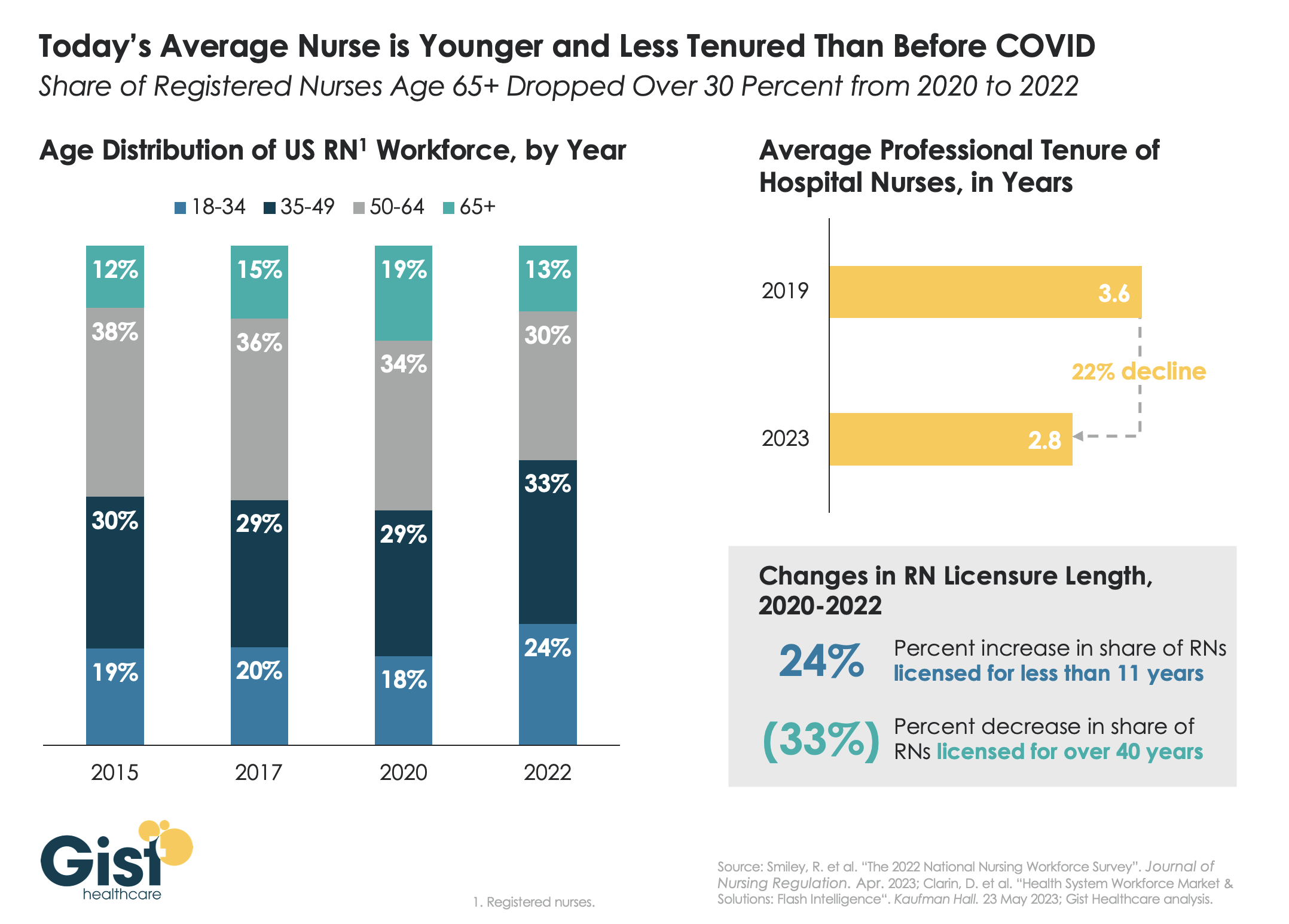
Last week we discussed how hospitals are still struggling to retain talent. This week’s graphic offers one explanation for this trend:
a significant share of older nurses, who continued to work during the height of the pandemic, have now exited the workforce, and health systems are even more reliant on younger nurses.
Between 2020 and 2022, the number of nurses ages 65 and older decreased by 200K, resulting in a reduction of that age cohort from 19 percent to 13 percent of the total nursing workforce. While the total number of nurses in the workforce still increased, the younger nurses filling these roles are both earlier in their nursing careers (thus less experienced), and more likely to change jobs.
Case in point:
From 2019 to 2023, the average tenure of a hospital nurse dropped by 22 percent. The wave of Baby Boomer nurse retirements has also resulted in a 33 percent decrease from 2020 to 2022 in the number of registered nurses who have been licensed for over 40 years.
Given these shifts, hospitals must adjust their current recruitment, retention, training, and mentorship initiatives to match the needs of younger, early-career nurses.
Monday’s walkout of tens of thousands of nurses and ambulance staff was the largest in the NHS’s 75-year history.
Labor demonstrations have been ongoing across the past few months, as workers demand higher pay and better working conditions amid rampant national inflation and increased workloads.
Specific demands vary by union and nation within the United Kingdom. Welsh nurses called off their strike this week to review a proposal from Wales’ Labour Party-run government, while the Royal College of Nurses, the UK’s largest nursing union, has countered a nominal 5 percent pay increase proposal with demands for a five percent pay raise on top of inflation, which topped 10 percent in Britain in December.
The Gist: A glance at our neighbors across the pond shows that the US healthcare system is not the only one currently experiencing a labor crisis.
The UK’s nationalized system has also failed to shield its workers from the combined impact of COVID burnout and inflation. But the NHS, as the UK’s largest employer and perennial object of political maneuvering, is more susceptible to organized labor actions.
In contrast, American healthcare unions, which only covered 17 percent of the country’s nurses in 2021, must negotiate with local employers, whose responses to their demands vary.
While this may enhance the bargaining power of US health system leaders, it also heightensthe risk that we will fail to adequately secure our nursing workforce, a key national resource already in short supply, for the longer term.
The majority of hospitals are predicted to have negative margins in 2022, marking the worst year financially for hospitals since the beginning of the Covid-19 pandemic.
In Part 1 of Radio Advisory’s Hospital of the Future series, host Rachel (Rae) Woods invites Advisory Board experts Monica Westhead, Colin Gelbaugh, and Aaron Mauck to discuss why factors like workforce shortages, post-acute financial instability, and growing competition are contributing to this troubling financial landscape and how hospitals are tackling these problems.
As we emerge from the global pandemic, health care is restructuring. What decisions should you be making, and what do you need to know to make them? Explore the state of the health care industry and its outlook for next year by visiting advisory.com/HealthCare2023.
Those who left their jobs during the Great Resignation did so out of more than just frustration, but instead used it as an opportunity to follow their dreams and aspirations, writes Whitney Johnson, CEO of Disruption Advisors, a talent development company, in the Harvard Business ReviewApril 6.
The pandemic forced many people to reevaluate many facets of their lives, from where to live to how to spend more time with family. Ms. Johnson argues that workers’ thoughts on changing the way they work is a good thing, giving workers agency to discover new aspirations and proactively seek them.
“The Great Resignation appellation is, I believe, mistaken. Most workers are not simply quitting. They are following a dream refined in pandemic adversity. They are aspiring to grow in the ways most important to them,” she writes.
Even for those who have been forced out of the workforce, like working mothers and caregivers, Ms. Johnson argues that it will lead to a boom of innovative new businesses, created by those resourceful workers who find another way to work outside the realms of traditional industry.
She also states that this “great aspiration” is beneficial for employers too, who can make the most of a fresh pool of talent, full of newly motivated employees who are dedicated and searching for meaning.
Health system executives continue to tell us that the top issue now keeping them up at night is workforce engagement.
Exhausted from the COVID experience, facing renewed cost pressures, and in the midst of a once-in-a-generation rethink of work-life balance among employees, health systems are having increasing difficulty filling vacant positions, and holding on to key staff—particularly clinical talent. One flashpoint that has emerged recently, according to leaders we work with, is the growing divide between those working a “hybrid” schedule—part at home, part in the office—and those who must show up in person for work because of their roles. Largely this split has administrative staff on one side and clinical workers on the other, leading doctors, nurses, and other clinicians to complain that they have to come into work (and have throughout the pandemic), while their administrative colleagues can continue to “Zoom in”. There’s growing resentment among those who don’t have the flexibility to take a kid to baseball practice at 3 o’clock, or let the cable guy in at noon without scheduling time off, making the sense of burnout and malaise even more intense. Add to that the resurgence in COVID admissions in some markets, and the “help wanted” situation in the broader economy, and the health system workforce crisis looks worse and worse. Beyond raising wages, which is likely inevitable for most organizations, there is a need to rethink job design and work patterns, to allow a tired, frustrated, and—thanks to the in-person/WFH divide—envious workforce the chance to recover from an incredibly difficult year.
This week we caught up with a benefits consultant colleague to get her perspective on how employers are thinking about health benefits as they come out of the pandemic. “It seems like employers and health systems have switched places in their enthusiasm for direct contracting,” she shared.
Prior to the pandemic, employer interest in working directly with a health system around a narrow network product to deliver coordinated care was growing, but there were few systems offering attractive solutions. Now more health systems are ready, but the number of employees working remotely has created a new obstacle for direct contracting.
One chief people officer for a large employer noted that while some employees have relocated permanently, others are still hopping from one Airbnb to another: “It’s at the point where I have no idea where half of our people are living on any given day.” In this new “employee diaspora”, some firms are seeing ten percent or more of their formerly office-based workforce now located outside the market, creating challenges for a geographically concentrated network to meet their needs.
How many companies will allow permanent telework, and how many employees will take them up on it, remains to be seen (our colleague suggested we’ll know more in the fall, after the return to school anchors many families in place). But for now, the best employer partners for direct contracting efforts are likely mid-sized regional employers, who are more likely to retain a local workforce, and face fewer obstacles to making benefit design changes.