With nearly 30% of workers now having a high deductible health plan and a typical family being responsible for on average the first $8,000 of costs, consumers are increasingly weighing care versus cost. Historically, with a small copay, you would conveniently take care of an ailment without shopping around, but with the average person now bearing the brunt of the initial costs, wouldn’t you want to know how much a service costs and what other providers are charging before you “buy” the service?
CMS believes“consumers should be able to know, long before they open a medical bill, roughly how much a hospital will charge for items and services it provides.” Cue the hospital price transparency rule that just went into effect January 1, 2021. Hospitals are now required to post their standard charges, including the rates they negotiate with insurers, and the discounted price a hospital is willing to accept directly from a patient if paid in cash. As a consumer, the intent is to make it “easier to shop and compare prices across hospitals and estimate the cost of care before going to the hospital.”
There are a few different angles to analyze here:
Are hospitals following the rules?
Each hospital must post online a comprehensive machine readable file with all items and services, including gross charges, actual negotiated prices with insurers, and the cash price for patients who are uninsured. Additionally, hospitals must post the costs for 300 common “shoppable” services in a “consumer-friendly format.” Some hospitals and health systems have done a good job at posting these prices in a digestible format, like the Cleveland Clinic or Sutter Health, but others have posted complicated spreadsheets, relied on online cost estimator tools, or simply not posted them at all. An analysis from consulting firm ADVI of the top 20 largest hospitals in the U.S. found that not all of them appeared to completely comply with this mandate. In some instances, data was not able to be downloaded in a useable format, others did not post the DRG or service codes, and the variability in the terms/categories used simply created difficulty in comparing pricing information across hospitals. CMS has stated that a failure to comply with the rules could result in a fine of up to $300 per day. As with most new rules, there are growing pains, and hospitals will likely get better at this over time, assuming the data is being used for its original intent.
Is this helpful to consumers?
Consumers will able to see the variation in prices for the exact same service or procedure between hospitals and get an estimate of what they will be charged before getting the care. But how likely is the average person to go to their hospital’s website, look at a price, and change their decision about where to get care? In addition, awareness of these price transparency tools is still low among consumers. Frankly, it is competitors and insurers that have been first in line to review the data. Looking through a number of hospital websites, and even certain state agency sites that have done a good job at summarizing the costs, like Florida Health Price Finder, the price transparency tools are helpful, but appear to be much more suited for relatively standardized services that can be scheduled in advance, like a knee replacement. It’s highly unlikely you will be telling your ambulance driver what hospital to go to based on cost while in cardiac arrest…Plus, it’s all still confusing – even physicians have shared their bewilderment, when trying to decipher and compare pricing. Conceptually, price transparency should be beneficial to consumers, but it will take time; and it will need to involve not just the hospitals posting rates, but the outpatient care facilities as well. Knowing what you will pay before you decide to go to a physician’s office or a clinic or an urgent care or an ED will hopefully help drive consumers to make more educated decisions in the future.
Will this ultimately drive down costs?
I sure hope so. Revealing actual negotiated prices between hospitals and insurers should push the more expensive hospitals in the area to reduce prices, especially if consumers start using the other hospitals, instead. However, it could also have an inverse effect, with lower cost hospitals insisting on a payment increase from insurers; thereby driving up costs. In the end, as has historically been the case, the market power of certain providers will likely dictate the direction of costs in a given region. That is, until both price AND quality become fully transparent and the consumer is armed with the tools to shop for the best care at the lowest cost – consumerism here we come.
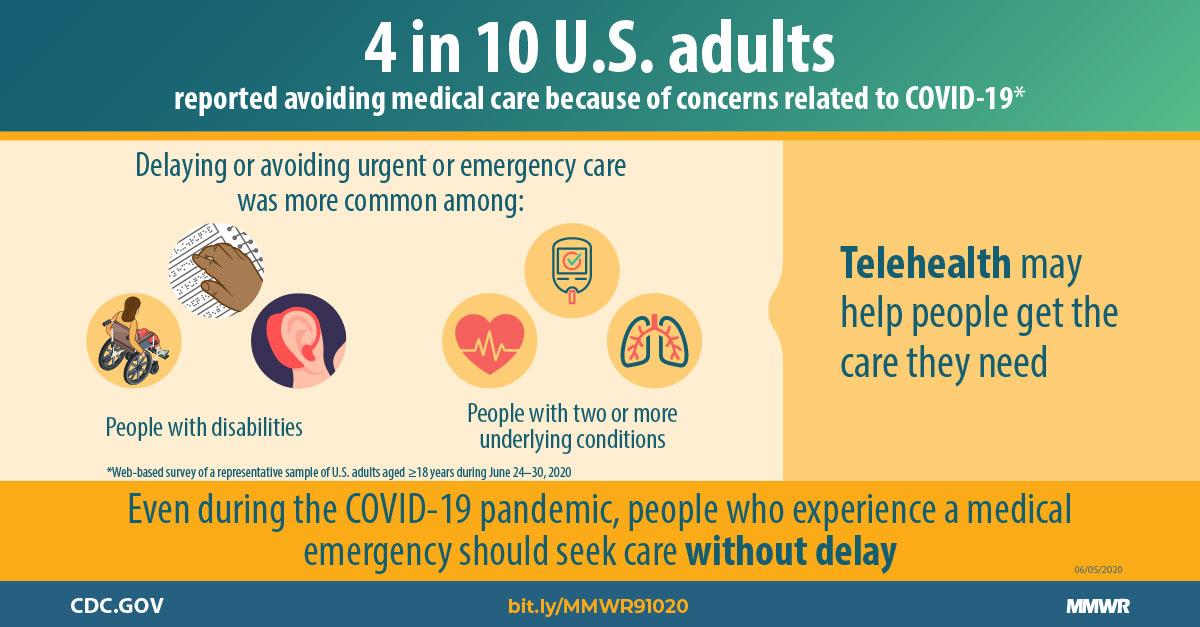
About 36% of nonelderly adults and 29% of children in the U.S. have delayed or foregone care because of concerns of being exposed to COVID-19 or providers limiting services due to the pandemic, according to new reports from the Urban Institute and Robert Wood Johnson Foundation.
Of those who put off care, more than three-quarters had one or more chronic health conditions and one in three said the result of not getting treatment was worsening health or limiting their ability to work and perform regular daily activities, the research based on polling in September showed.
However, the types of care being delayed are fairly routine. Among those surveyed, 25% put off dental care, while 21% put off checkups and 16% put off screenings or medical tests.
Dive Insight:
The early days of the pandemic saw widespread halts in non-emergency care, with big hits to provider finances.
In recent months, health systems have emphasized the services can be provided in hospitals and doctors offices safely as long as certain protocols are followed, and at least some research has backed them up. Groups like the American Hospital Association have launched ad campaigns urging people to return for preventive and routine care as well as emergencies.
But patients are apparently still wary, according to the findings based on surveys of about 4,000 adults conducted in September.
The research shows another facet of the systemic inequities harshly spotlighted by the pandemic. People of color are more likely to put off care than other groups. While 34% of Whites said they put off care, that percentage rose to 40% among Blacks and 36% among Latinos.
Income also played a role, as 37% of those with household incomes at or below 250% of the poverty level put off care, compared to 25% of those with incomes above that threshold.
Putting off care has had an impact industrywide, as the normally robust healthcare sector lost 30,000 jobs in January. Molina Healthcare warned last week that utilization will remain depressed for the foreseeable future.
Younger Americans were also impacted, with nearly 30% of parents saying they delayed at least one type of care for their children, while 16% delayed multiple types of care. As with adults, dental care was the most common procedure that was put off, followed by checkups or other preventative healthcare screenings.
The researchers recommended improving communications among providers and patients.
“Patients must be reassured that providers’ safety precautions follow public health guidelines, and that these precautions effectively prevent transmission in offices, clinics, and hospitals,” they wrote. “More data showing healthcare settings are not common sources of transmission and better communication with the public to promote the importance of seeking needed and routine care are also needed.”
“I don’t think we have good enough information to show how we should be deploying telemedicine,” a physician leader recently told us. “If we can’t show that a virtual visit can adequately substitute for an in-person visit, then we should be focusing on making sure patients know it’s safe to come in.” It struck us that viewing telemedicine as a direct substitute for an office visit was a narrow and antiquated way to think about virtual care.
Moreover, the argument that telemedicine visits are potentially cost-increasing if they are “additive” to other care interactions, rather than “substitutive”, is rooted in fee-for-service payment: more patient-provider interactions equals more billable visits, and with more visits, we run the risk of increasing costs.
Telemedicine (both video and phone visits) likelytaps into pent-up demand for accessby patients who would otherwise not seek care. Some patients could be aided by more frequent, brief encounters; this is considered a failure only when viewed through the lens of fee-for-service payment. (Honestly, with primary care accounting for less than 6 percent of total healthcare spending, it’s hard to argue that additional telemedicine visits will be responsible for supercharging the cost of care.) Of course, there are many clinical situations in which in-person interaction—to perform a physical exam, measure vitals, observe a patient—is fundamental. Patients know this, and understand that sometimes they’ll need to be seen in person. But hopefully that next encounter will be more efficient, having already covered the basics.
The ideal care model will look different for different patients, and different kinds of clinical problems—but will likely be a blend of both virtual and in-person interactions, maximizing communication, information-gathering, and patient convenience.
A growing body of research keeps undermining a key tenet of health economics, Axios’ Sam Baker writes — the belief that requiring patients to pay more out of their own pockets will make them smarter consumers, forcing the health care system to deliver value.
Driving the news:Even a seemingly modest increase in out-of-pocket costs will cause many patients to stop taking drugs they need, according to a new working paper from Harvard economist Amitabh Chandra.
Raising Medicare recipients’ out-of-pocket costs by just $10 per prescription led to a 23% drop in overall drug consumption, and to a 33% increase in mortality.
And seniors weren’t simply ditching “low-value” drugs. People at high risk for heart attacks or strokes cut back on statins and blood-pressure medications even more than lower-risk patients.
Between the lines: This research focuses on Medicare’s drug benefit, but higher cost-sharing is all the rage throughout the system, and there’s little evidence that it has generated “smarter shoppers.”
Patients with high-deductible plans — increasingly common in the employer market — don’t shop around for the best deal, which is all but impossible to do in many cases even if you wanted to try.
As “consumerism” becomes an ever-greater focus of health system strategy, we’ve begun to field a number of questions from leaders looking to develop a better understanding of consumers in their market.
In particular, there’s a growing desire for more sophistication around consumer segmentation—understanding how preferences and behavior differ among various kinds of patients.
Traditional segmentation has largely been marketing-driven, helping to target advertising and patient recruitment messages to key groups. For that, the old-school marketing segments were good enough: busy professionals, the worried well, the growing family, and so forth.
But as systems begin to develop product offerings (telemedicine or home-based services, for example) for target populations, those advertising-based segments need to be supplemented with a more advanced understanding of care consumption patterns over time. Segmentation needs to be dynamic, not static—how does a person move through life stages, and across care events, over time?
A single consumer might be in different segments depending on the type of care they need: if I have a new cancer diagnosis, that matters more than whether I’m a “busy professional”, and my relevant segment might be different still if I’m just looking for a quick virtual visit.
Layered on top of demographic and clinical segments is the additional complexity of payer category—am I a Medicare Advantage enrollee or do I have a high-deductible exchange plan?
With consumers exercising ever greater choice over where, when, and how much care to receive, understanding the interplay of these different kinds of segments is fast becoming a key skill for health systems—one that many don’t currently have.
Humana, the nation’s second-largest Medicare Advantage (MA) insurer, is pushing further into home-based care, partnering with Denver-based startup DispatchHealthto offer its members—especially those with conditions like heart failure, chronic obstructive pulmonary disease, and chronic cellulitis—access tohospital-level care at home.
The service will initially be available in the Denver and Tacoma, WA markets, with plans to expand to Arizona, Nevada, and Texas across 2021. Humana members who meet hospital admission criteria will receive daily home visits from an on-call, dedicated DispatchHealth medical team, as well as 24/7 physician coverage enabled by remote monitoring and an emergency call button.
DispatchHealth will also coordinate other patient care and wraparound services in the home as needed, including pharmacy, imaging, physical therapy, durable medical equipment, and meal delivery. Dispatch’s earlier offerings centered around home-based, on-demand urgent and emergency care services, now available in at least 29 cities nationwide.
Humana’s partnership with DispatchHealth could deliver a full care continuum of home-based services to its Medicare Advantage enrollees and has the potential to displace hospitals from at least a portion of acute care services.
Post-COVID, it’s becoming increasingly clear that the nexus of care delivery has shifted even more rapidly to consumers’ homes—and traditional providers will need to rethink service strategies accordingly.
UnitedHealth Group, both the nation’s largest health insurer and largest employer of physicians, just announced plans to continue to rapidly grow the number of physicians in its Optum division.
This week CEO Dave Wichmann told investors in the company’s fourth quarter earnings call that Optum entered 2021 with over 50,000 employed or affiliated physicians, and expects to add at least 10,000 more across the year.(For context,HCA Healthcare, the largest for-profit US health system, employs or affiliates with roughly 46,000 physicians, and Kaiser Permanente employs about 23,300.) Optum is already making progress toward its ambitious goal with the announcement last week that the company is in talks to acquire Atrius Health, a 715-physician practice in the Boston area.
As was the case with other health plans, United’s health insurance business took an expected hit last quarter due to increased costs from COVID testing and treatment, combined with rebounding healthcare utilization. Optum, however, saw revenue up over 20 percent, which drove much of the company’s overall fourth quarter growth.
Expect United, and other large insurers, flush with record profits from last year, to continue to expand their portfolio of care, digital and analytics assets(see also Optum’s recently announced plan to acquire Change Healthcare for $13B) as they looks to grow integrated insurance and care delivery offerings.
It’s part of what we expect to be a 2021 “land grab” for strategic advantage in healthcare, as providers, health plans, and disruptors look to create comprehensive platforms to secure long-term consumer loyalty.
The annual J.P. Morgan Healthcare Conference is one of the best ways to diagnose the financial condition of the healthcare industry. Every January, every key stakeholder — providers, payers, pharmaceutical companies, tech companies, medical device and supply companies as well as bankers, venture capital and private equity firms — comes together in one exam room, even when it is virtual, for their annual check-up. But as we all know, this January is unlike any other as this past year has been unlike any other year.
You would have to go back to the banking crisis of 2008 to find a similar moment from an economic perspective. At the time, we were asking, “Are banks too big to fail?” The concern behind the question was that if they did fail, the economic chaos that would follow would lead to a collapse with the consumer ultimately picking up the tab. The rest is history.
Healthcare is “Too Vital to Fail”
2020 was historic in too many ways to count. But in a year when healthcare providers faced the worst financial crisis in the history of healthcare, the headline is that they are still standing. And what they proved is that in contrast to banks in 2008 that were seen by many as “too big to fail,” healthcare providers in 2020 proved that they were “too vital to fail.”
One of the many unique things about the COVID-19 pandemic is we are simultaneously experiencing a health crisis, where healthcare providers are the front line in the battle, and an economic crisis, felt in a big way in healthcare given the unique role hospitals play as the largest employer in most communities. Hospitals and health systems have done the vast majority of testing, treating, monitoring, counseling, educating and vaccinating all while searching for PPE and ventilators, and conducting clinical trials. And that’s just the beginning of the list.
Stop and think about that for a minute. What would we have done without them? Thinking through that question will give you some appreciation for the critical, challenging and central role that healthcare providers have had to play over the past year.
Simply stated, healthcare providers are the heart of healthcare, both clinically (essentially 100 percent of the care) and financially (over 50 percent of the $4 trillion annual spend on U.S. healthcare). Over the last year they stepped up and they stepped in at the moment where we needed them the most. This was despite the fact that, like most businesses, they were experiencing calamitous losses with no assurances of any assistance.
Healthcare is “Pandemic-Proof”
This was absolutely the worst-case scenario and the biggest test possible for our nation’s healthcare delivery system. Patient volume and therefore revenue dropped by over 50 percent when the panic of the pandemic was at its peak, driving over $60 billion in losses per month across hospitals and healthcare providers. At the same time, they were dramatically increasing their expenses with PPE, ventilators and additional staff. This was not heading in a good direction. While failure may not have been seen as an option, it was clearly a possibility.
The CARES Act clearly provided a temporary lifeline, providing funding for our nation’s hospitals to weather the storm. While there are more challenging times ahead, it is now clear that most are going to make it to the other side. The system of care in our country is often criticized, but when faced with perhaps the most challenging moment in the history of healthcare, our nation’s hospitals and health systems stepped up heroically and performed miraculously. The work of our healthcare providers on the front line and those who supported them was and is one thing that we all should be exceptionally proud of and thankful for.In 2020, they proved that not only is our nation’s healthcare system too vital to fail, but also that it is “pandemic proof.”
Listening to Front Line at the 2021 J.P. Morgan Healthcare Conference
There has never been a more important year to listen to the lessons from healthcare providers. They are and were the front line of our fight against COVID-19. If there was a class given about how to deal with a pandemic at an institutional level, this conference is where those lessons were being taught.
This year at the J.P. Morgan Healthcare Conference, CEOs, and CFOs from many of the most prestigious and most well-respected health systems in the world presented including AdventHealth, Advocate Aurora Health, Ascension, Baylor Scott & White Health, CommonSpirit Health, Henry Ford Health System, Intermountain Healthcare, Jefferson Health, Mass General Brigham, Northwell Health, OhioHealth, Prisma Health, ProMedica Health System, Providence, Spectrum Health and SSM Health.
I’ve been in healthcare for 30 years and this is my fifth year of writing up the summary of the non-profit provider track of the conference for Becker’s Healthcare to help share the wisdom of the crowd of provider organizations that share their stories. Clearly, this year was different and not because the presentations were virtual, but because they were inspirational.
What did we learn? The good news is that they have made many changes that have the potential to move healthcare in a much better direction and to get to a better place much faster. So, this year instead of providing you a nugget from each presentation, I am going to take a shot at summarizing what they collectively have in motion to stay vital after COVID.
10 Moves Healthcare Providers are Making to Stay Vital After-COVID
As a leader in healthcare, you will never have a bigger opportunity to drive change than right now. Smart leaders are framing this as essentially “before-COVID (BC)” and “after-COVID (AC)” and using this moment as their burning platform to drive change. Credit to the team at Providence for the acronym, but every CEO talked about this concept. As the saying goes, “never let a good crisis go to waste.” Well, we’ve certainly had a crisis, so here is a list of what the top health systems are doing to ensure that they don’t waste it and that they stay vital after-COVID:
1. Take Care of Your Team and They’ll Take Care of You: In a crisis, you can either come together as a team or fall apart. Clearly there has been a significant and stunning amount of pressure on healthcare providers. Many are fearing that mental health might be our nation’s next pandemic in the near future because they are seeing it right now with their own team. Perhaps one of their biggest lessons from this crisis has been the need to address the mental, physical and spiritual health of both team members as well as providers. They have put programs in place to help and have also built a tremendous amount of trust with their team by, in many cases, not laying off and/or furloughing employees. While they have made cuts in other areas such as benefits, this collective approach proved incredibly beneficial. And the last point here that relates to thinking differently about their team is that similar to other businesses, many health systems are making remote arrangements permanent for certain administrative roles and moving to a flexible approach regarding their team and their space in the future.
2. Focus on Health Equity, Not Just Health Care: This was perhaps the most notable and encouraging change from presentations in past years at J.P. Morgan. I have been going to the conference for over a decade, and I’ve never heard someone mention this term or outline their efforts on “health equity” — this year, nearly everyone did. In the past, they have outlined many wonderful programs on “social determinants of health,” but this year they have seen the disproportionate impact of COVID on low-income communities bringing the ongoing issue of racial disparities in access to care and outcomes to light. As the bedrock of employment in their community, this provides an opportunity to not just provide health care, but also health equity, taking an active role to help make progress on issues like hunger, homelessness, and housing. Many are making significant investments in a number of these and other areas.
3. Take the Lead in Public Health — the Message is the Medicine:One of the greatest failings of COVID, perhaps the greatest lesson learned, is the need for clear and consistent messaging from a public health perspective. That is a role that healthcare providers can and should play. In the pandemic, it represented the greatest opportunity to save lives as the essence of public health is communication — the message is the medicine. A number of health systems stepped into this opportunity to build trust and to build their brand, which are essentially one in the same. Some organizations have created a new role — a Chief Community Health Officer — which is a good way to capture the work that is in motion relative to social determinants of health as well as health equity. Many understand the opportunity here and will take the lead relative to vaccine distribution as clear messaging to build confidence is clearly needed.
4. Make the Home and Everywhere a Venue of Care:A number of presenters stated that “COVID didn’t change our strategy, it accelerated it.” For the most part, they were referring to virtual visits, which increased dramatically now representing around 10 percent of their visits vs. 1 percent before-COVID. One presenter said, “Digital has been tested and perfected during COVID,” but that is only considering the role we see digital playing in this moment. It is clear some organizations have a very narrow tactical lens while others are looking at the opportunity much more strategically. For many, they are looking at a “care anywhere and everywhere” strategy. From a full “hospital in the home” approach to remote monitoring devices, it is clear that your home will be seen as a venue of care and an access point moving forward. The pandemic of 2020 may have sparked a new era of “post-hospital healthcare” — stay tuned.
5. Bury Your Budget and Pivot to Planning:The budget process has been a source of incredible distrust, dissatisfaction and distraction for every health system for decades. The chaos and uncertainty of the pandemic forced every organization to bury their budget last year. With that said, many of the organizations that presented are now making a permanent shift away from a “budget-based culture” where the focus is on hitting a now irrelevant target set that was set six to nine months ago to a “performance-based culture” where the focus is on making progress every day, week, month and quarter. Given that the traditional annual operating budget process has been the core of how health systems have operated, this shift to a rolling forecast and a more dynamic planning process is likely the single most substantial and permanent change in how hospitals and health systems operate due to COVID. In other words, it is arguably a much bigger headline than what’s happened with virtual visits.
6. Get Your M&A Machine in Motion: It was clear from the presentations that activity around acquisitions is going to return, perhaps significantly. These organizations have strong balance sheets and while the strong have gotten stronger during COVID, the weak have in many cases gotten weaker. Many are going to be opportunistic to acquire hospitals, but at the same time they have concluded that they can’t just be a system of care delivery. They are also focused on acquiring and investing in other types of entities as well as forming more robust partnerships to create new revenue streams. Organizations that already had diversified revenue streams in place came through this pandemic the best. Most hospitals are overly reliant on the ED and surgical volume. Trying to drive that volume in a value-based world, with the end of site of service differentials and the inpatient only list, will be an even bigger challenge in the future as new niche players enter the market. As I wrote in the headline of my summary two years ago, “It’s the platform, stupid.” There are better ways to create a financial path forward that involve leveraging their assets — their platform — in new and creative ways.
7. Hey, You, Get into the Cloud:With apologies for wrapping a Rolling Stones song into a conference summary, one of the main things touted during presentations was “the cloud” and their ability to pull clinical, operational and financial dashboards together to monitor the impact of COVID on their organization and organize their actions. Focus over the last decade has been on the clinical (implementing EHRs), but it is now shifting to “digitizing operations” with a focus on finance and operations (planning, cost accounting, ERPs, etc.) as well as advanced analytics and data science capabilities to automate, gather insight, manage and predict. It is clear that the cloud has moved from a curiosity to a necessity for health systems, making this one of the biggest areas of investment for every health system over the next decade.
8. Make Price Transparency a Key Differentiator: One of the great lessons from Amazon (and others) is that you can make a lot of money when you make something easy to buy. While many health systems are skeptical of the value of the price transparency requirements, those that have a deep understanding of both their true cost of care and margins are using this as an opportunity to prove their value and accelerate their strategy to become consumer-centric. While there is certainly a level of risk, no business has ever been unsuccessful because they made their product easier to understand and access. Because healthcare is so opaque, there is an opening for healthcare providers to build trust, which is their main asset, and volume, which is their main source of revenue, by becoming stunningly easy to do business with. This may be tough sledding for some as this isn’t something healthcare providers are known for. To understand this, spend a few minutes on Tesla’s website vs. Ford’s. The concept of making something easy, or hard, to buy will become crystal clear as fast as a battery-driven car can go from zero to 60.
9. Make Care More Affordable:This represents the biggest challenge for hospitals and health systems as they ultimately need to be on the right side of this issue or the trust that they have will disappear and they will remain very vulnerable to outside players. All are investing in advanced cost accounting systems (time-driven costing, physician costing, supply, and drug costing) to truly understand their cost and use that as a basis to price more strategically in the market. Some are dropping prices for shoppable services and using loss leader strategies to build their brand. The incoming Secretary of Health and Human Services has a strong belief regarding the accountability of health systems to be consumer centric. The health systems that understand this are working to get ahead of this issue as it is likely one of their most significant threats (or opportunities) over the next decade. This means getting all care to the right site of care, evaluating every opportunity to improve, and getting serious about eliminating the need for expensive care through building healthy communities. If you’re worried about Wal-Mart or Amazon, this is your secret weapon to keep them on the sideline.
10. Scale = Survival: One of the big lessons here is that the strong got stronger, the weak got weaker. For the strong, many have been able to “snapback” in financial performance because they were resilient. They were able to designate COVID-only facilities, while keeping others running at a higher capacity. To be clear, while most health systems are going to get to the other side and are positioned better than ever, there are many others that will continue to struggle for years to come. According to our data at Strata, we see 25 percent operating at negative margins right now and another 50 percent just above breakeven. They key to survival moving forward, for those that don’t have a captive market, will be scale. If this pandemic proved one thing relative to the future of health systems it is this — scale equals survival.
When Will We Return to Normal?
Based on what the projections that these health systems shared, the “new normal” for health systems for the first half of 2021 will be roughly 95 percent of prior year inpatient volume with a 20 percent year-over-year drop in ED volume and a drop of 10-15 percent in observation visits. So, the pain will continue, but given the adjustments that were already made in 2020, it looks like they will be able to manage through COVID effectively. While there will be a pickup in the second half of 2021, the safe bet is that a “return to normal” pre-COVID volumes likely won’t occur until 2022. And there are some who believe that some of the volume should have never been there to begin with and we might see a permanent shift downward in ED volume as well as in some other areas.
With that said, I’ll steal a quote from Bert Zimmerli, the CFO of Intermountain Healthcare, who said, “Normal wasn’t ever nearly good enough in healthcare.”In that spirit, the goal should be to not return to normal, but rather to use this moment as an opportunity to take the positive changes driven by COVID — from technology to processes to areas of focus to a sense of responsibility — and make them permanent.
Thanking Our “Healthcare Heroes”
We’ll never see another 2020 again, hopefully. With that said, one of the silver linings of the year is everything we learned in healthcare. The most important lesson was this — in healthcare there are literally heroes everywhere. To each of them, I just want to say “thank you” for being there for us when we needed you the most. We should all be writing love letters to those on the front line who risked their lives to save others. Our nation’s healthcare system has taken a lot of criticism through the years from those on the outside, often with a blind eye to how things work in practice vs. in concept. But this year we all got to see first-hand what’s happening inside of healthcare — the heroic work of our healthcare providers and those who support them.
They faced the worst crisis in the history of healthcare. They responded heroically and were there for our families and friends.
They proved that healthcare is too vital to fail. They proved that healthcare is pandemic-proof.