

Cartoon – Betting on Management

Hospitals across the U.S. saw their operating margins remain negative for the second consecutive month in February as they continued to feel the repercussions of the winter omicron surge, according to Kaufman Hall’s “National Hospital Flash Report: March 2022” posted March 28.
The median operating margin in February was -3.45 percent, up from -4.52 percent in January, but “still well below sustainable levels,” Kaufman Hall said.
Kaufman Hall said the improvement in hospital margin was driven by disproportionate increases among several hospitals that saw margin gains, but most hospitals reported margin declines in February. Specifically, the median operating margin was down 11.8 percent month over month.
“The second month of 2022 brought further challenges for the nation’s hospitals and health systems,” Kaufman Hall said. “Overall, the year is off to a difficult start.”
Kaufman Hall noted that patient days were down 13.3 percent month over month, and fewer severely ill COVID-19 patients also contributed to shorter hospital stays as the average length of stay dropped 5.3 percent month over month.
Hospitals’ gross operating revenue also decreased 7.4 percent compared to January 2022, with outpatient revenue falling 5 percent and inpatient revenue declining 19.3 percent.
Kaufman Hall noted that hospitals saw some improvement month over month in terms of expenses. Total expenses per adjusted discharge fell 4.5 percent compared to January, labor expense per adjusted discharge fell 6.1 percent and non-labor expenses per adjusted discharge was down 3.6 percent. However, Kaufman Hall noted that year over year, expenses are still up significantly, with total adjusted expense per adjusted discharge rising 10.4 percent compared to February 2021.
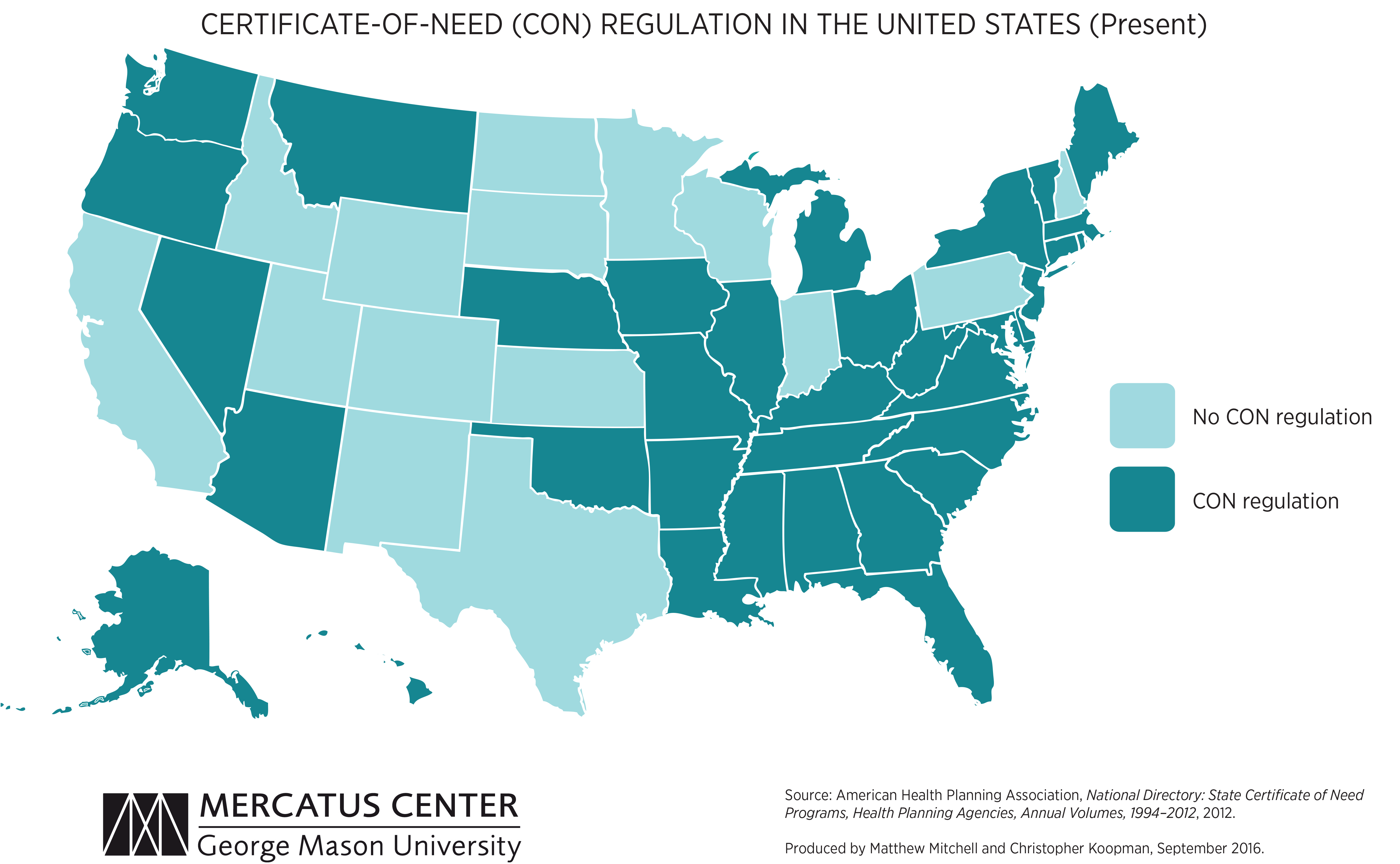
We’re picking up on a growing concern among health system leaders that many states with “certificate of need” (CON) laws in effect are on the cusp of repealing them. CON laws, currently in place in 35 states and the District of Columbia, require organizations that want to construct new or expand existing healthcare facilities to demonstrate community need for the additional capacity, and to obtain approval from state regulatory agencies. While the intent of these laws is to prevent duplicative capacity, reduce unnecessary utilization, and control cost growth, critics claim that CON requirements reduce competition—and free market-minded state legislators, particularly in the South and Midwest, have made them a target.
One of our member systems located in a state where repeal is being debated asked us to facilitate a scenario planning session around CON repeal with system and physician leaders. Executives predicted that key specialty physician groups would quickly move to build their own ambulatory surgery centers, accelerating shift of surgical volume away from the hospital.
The opportunity to expand outpatient procedure and long-term care capacity would also fuel investment from private equity, which have already been picking up in the market. An out-of-market health system might look to build microhospitals, or even a full-service inpatient facility, which would be even more disruptive.
CON repeal wasn’t all downside, however; the team identified adjacent markets they would look to enter as well. The takeaway from our exercise: in addition to the traditional response of flexing lobbying influence to shape legislative change, the system must begin to deliver solutions to consumers that are comprehensive, convenient, and competitively priced—the kind of offerings that might flood the market if CON laws were lifted.
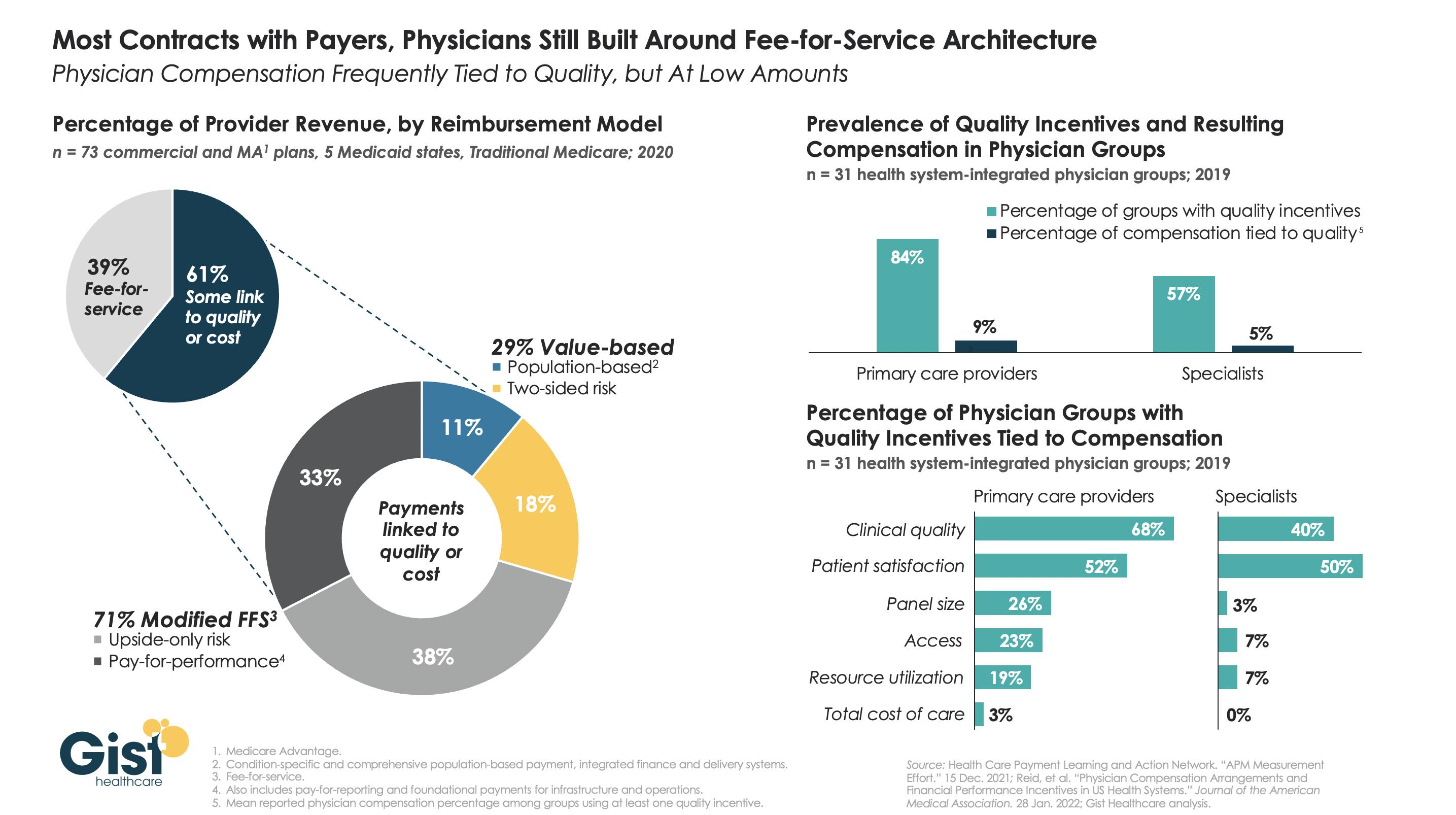
The healthcare industry has made some strides in the “journey to value” across the last decade, but in reality, most health systems and physician groups are still very much entrenched in fee-for-service incentives.
While many health plans report that significant portions of their contract dollars are tied to cost and quality performance, what plans refer to as “value” isn’t necessarily “risk-based.”
The left-hand side of the graphic below shows that, although a majority of payer contracts now include some link to quality or cost, over two-thirds of those lack any real downside risk for providers.
Data on the right show a similar parallel in physician compensation. While the majority of physician groups have some quality incentives in their compensation models, less than a tenth of individual physician compensation is actually tied to quality performance.
Though myriad stakeholders, from the federal government to individual health systems and physician groups, have collectively invested billions of dollars in migrating to value-based payment over the last decade, we are still far from seeing true, performance-based incentives translate into transformation up and down the healthcare value chain.

Dialysis giant Fresenius Medical Care is creating a new $2.4B company by combining its US value-based care division, Fresenius Health Partners, with nephrologist network InterWell Health, and digital-first kidney care startup Cricket Health. Cricket Health CEO Robert Sepucha is set to lead the new company, which will be named InterWell Health, assuming the deal closes in the second half of 2022 as expected.
The Gist: This move will enable Fresenius to move further up the renal care delivery chain, managing patients with earlier stage chronic kidney disease before they need dialysis. Fresenius says the new company will more than triple its total addressable market in the US, from $50B to around $170B.
Seeing an opportunity to disrupt the dialysis market, which has been dominated by for-profit giants Fresenius and DaVita, significant capital has been flowing to numerous disruptors in the kidney care space who aim to bring care closer to consumers. Medicare, which spends nearly $115B annually on chronic kidney disease, is testing new payment models aimed at delaying the need for dialysis, as well as moving care into patients’ homes.
But whether Fresenius’s latest moves will make a significant difference in lowering the cost of kidney care remains to be seen.

Spurred by the Consumer Financial Protection Bureau’s investigation into how credit companies report medical debt, TransUnion, Equifax, and Experian—the country’s three largest credit bureaus, who keep records on 200M Americans—are revising how they report medical debt.
As a result, the companies could eliminate up to 70 percent of medical debt from consumers’ credit reports. Starting in July, medical debts paid after going to collections will no longer appear on credit reports, and unpaid debts won’t be added until a year after being sent to collections (instead of six months, per current policy). And beginning in 2023, medical debts of less than $500 will also be excluded from credit reports altogether.
The Gist:The poorest and sickest patients have been disproportionately saddled with the highest levels of medical debt. In 2017, 19 percent of US households carried medical debt, including many with private insurance.
While these changes will help mitigate the impact of medical debt for some, they aren’t a fix to the larger underlying problem of rising healthcare costs and access to adequate health insurance coverage.
Starting next month, the federal government will stop reimbursing hospitals and other providers for the vaccination, testing, and treatment of uninsured COVID-19 patients. So far, about 50K providers have submitted a total of $20B of claims for COVID-related care for the uninsured.
Congress has yet to authorize more funding for this and other COVID relief programs, after stripping $15.6B from the latest government spending package. Though the White House is asking Congress to authorize $22.5B for further COVID aid and surge preparedness, it’s not clear how much of any new funding would go toward reimbursing care for the uninsured.
The Gist: This news comes as US officials expect a rise in cases driven by the Omicron BA.2 subvariant. Hospitals, already struggling with high labor and supply expenses, will face further margin pressures if a future COVID surge brings increased hospitalizations.
This will be especially true for safety net hospitals, and for those in states which haven’t expanded Medicaid. At the same time, 15M Americans are also at risk of losing Medicaid coverage when the federal government ends the public health emergency. Lower-income patients and the hospitals that treat them have already shouldered COVID’s worst effects, and the funding stalemate risks further worsening their situation.

The expected green light for a second coronavirus booster shot poses a challenge to the Biden administration, which will need to work overtime to convince a public that has largely decided to move on from the COVID-19 pandemic.
Both Pfizer and Moderna have filed for emergency use authorization with the Food and Drug Administration for a fourth dose of their respective vaccines, citing evidence that protection from the third shot has decreased enough to warrant a fourth dose.
Yet the nation’s vaccination and booster rates have dropped to record lows, just as experts and officials are bracing for the possibility of another wave of infections from the BA.2 subvariant of omicron.
The BA.2 version of omicron is much more transmissible than the original variant. Combined with relaxed precautions like indoor masking and waning immunity among those who have not received a vaccine booster, cases have risen sharply in Europe in the past few weeks, and the U.S. could follow shortly.
The omicron subvariant is responsible for about 35 percent of all cases in the country. In some regions though, like the northeast, it is responsible for the majority of infections.
Federal health officials are reportedly poised to authorize a fourth dose of coronavirus vaccine for adults age 50 and older as soon as this week. A fourth shot is already authorized for the immunocompromised.
But the issues that plagued the administration during the first booster campaign loom large, and officials are likely eager to avoid the same pitfalls.
Chaotic and at times disparate messages from administration health officials culminated in a complicated set of recommendations about who should be getting booster shots, and why, which experts said helped depress enthusiasm.
“I think that some of the low uptake of boosters, especially amongst people who would benefit, the high risk population, is because that message has been diluted,” said Amesh Adalja, a senior scholar at the Johns Hopkins Center for Health Security.
But the underlying disagreement about the goal of booster shots has not changed. While there’s widespread agreement that older Americans are much more at risk for severe outcomes, it’s still not clear if younger people will benefit from an additional dose.
Much of the debate has centered on whether the goal is to prevent people from being hospitalized with COVID-19 or whether the goal is to prevent them from getting sick at all, even if it is milder.
Anthony Fauci, White House chief medical advisor and the nation’s top infectious disease doctor, said regulators are trying to determine how low protection against hospitalization needs to drop before a booster is warranted.
“So the real open question that we don’t know definitively the answer to, is how long is the durability of protection against severe disease going to last even when the protection against infection diminishes substantially,” Fauci said during a Washington Post event last week.
“For example, we know that when you get down to a rather low level 30, 40 or so percent of protection against infection, you still have, when you look at hospitalization, a high degree [of protection],” Fauci said.
President Biden last summer promised widespread boosters for all Americans by the end of September, well before the FDA and the Centers for Disease Control and Prevention (CDC) had examined the evidence.
While officials were careful to say the booster program was contingent on the FDA and CDC giving the green light, scientists inside and outside the government argued there wasn’t enough evidence showing protection against severe illness and hospitalization dropped to levels that warranted a booster.
The CDC initially decided against recommending broad authorization, and instead recommended a booster shot for people over the age of 65, as well as anyone who was at “high risk” of exposure to the virus in the workplace.
The agency eventually decided to make everyone eligible, but by then much of the damage had been done. Vaccinated Americans have largely shown they are not interested in getting a booster.
According to current CDC data, less than 45 percent of all adults have received a booster shot, but the number rises to about 67 percent of adults age 65 and older.
Adalja said it makes sense to be proactive and have a plan to get additional booster shots to the older group. But he said the decisions should be left to the scientists, and the health agencies should make decisions independent of the White House.
“Keep the politicians out of it,” Adalja said. “The miscommunications occurred because they made boosters a political issue, not a scientific issue.”
But even if there is a targeted recommendation, a stalled funding request in Congress further complicates matters. The U.S government does not have enough doses on hand to vaccinate everyone who would be eligible for another booster.
The White House says it needs tens of billions of dollars in COVID response funding, which is tied up due to political disagreements. Administration officials say they don’t have enough doses on hand to cover anyone other than the immunocompromised and people aged 65 and older.
But an independent analysis from the Kaiser Family Foundation found the government only has enough vaccine supplies to cover 70 percent of the 65 and older group.


Cases of COVID-19 have increased during the last 14 days in 10 states and Washington, D.C., with the latest additions of the district and Illinois.
Nationwide, COVID-19 cases decreased 15 percent over the past 14 days, according to HHS data collected by The New York Times. But as the more contagious omicron subvariant BA.2 continues to spread, cases are ticking upward in 10 states and D.C. as of March 25. Cases were moving upward in nine states as of March 24, with D.C. and Illinois reporting increases a day later.
Here are the 14-day changes for cases in each state reporting an increase, according to HHS data collected by The New York Times:
New York: 44 percent
Kentucky: 35 percent
Arkansas: 23 percent
Colorado: 21 percent
Connecticut: 18 percent
Texas: 17 percent
Massachusetts: 15 percent
Vermont: 13 percent
Rhode Island: 11 percent
Washington, D.C.: 5 percent
Illinois: 1 percent
The latest variant proportion estimates from the CDC show the omicron subvariant BA.2 accounts for more than one-third of COVID-19 cases nationwide and more than half of cases in the Northeast. Rhode Island has the highest proportion of BA.2 cases of all states, according to the latest ranking of states by the subvariant’s prevalence.
“If we maintain our preparedness, an increase in cases does not need to be a cause for alarm like it once was,” Jeff Zients, White House COVID-19 response coordinator, said in a March 23 media briefing. “We know what tools we need to fight the virus. Unfortunately, because of congressional action, we’re at risk of not having these tools readily available.”
President Joe Biden signed into law March 15 a sweeping $1.5 trillion bill that funds the government through September. The legislation did not include COVID-19 funding the White House had requested from Congress due to partisan disagreement about offsetting the funding.
There is no clear path to approval of more COVID-19 funding.
The lack of funding is affecting resources for COVID-19 testing and treatment. The Health Resources and Services Administration stopped accepting providers’ claims for COVID-19 testing and treatment of the uninsured March 22 due to a lack of sufficient funds. The federal government is also cutting back shipments of monoclonal antibody treatments to states by 30 percent, and the U.S. supply of those treatments could run out as soon as May.
