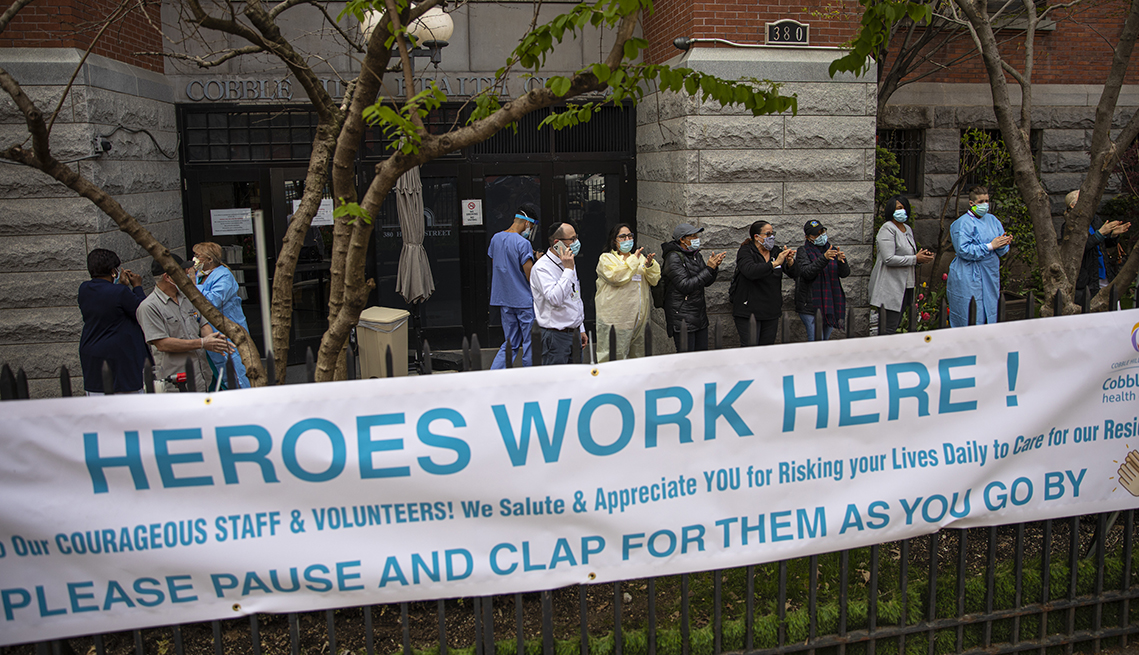
As the US approaches the grim statistic of one million deaths from COVID, journalist Ed Yong’s latest piece in The Atlantic takes a sobering look at how numb we’ve become to that astronomically high toll. In the early days of the pandemic, predictions of a few hundred thousand American deaths seemed shocking, but recent milestones of 800K and 900K lives lost have ticked by with little public attention.
Yong blames the invisibility of the virus: its worst impacts have been disproportionately concentrated among the disadvantaged—making it possible for COVID to more easily “disappear” from the lives of the healthy and economically advantaged. Case in point: while three percent of Americans have lost a close family member to COVID-19, the virus has taken a much larger toll on people of color, the elderly, and those with underlying health conditions.
The Gist:The pandemic has rendered us numb to the ongoing tragic loss of life, leading us to accept over 1,500 COVID deaths each day as “normal”.
As Yong points out, it’s hard to imagine we could turn a blind eye to this number of Americans perishing every day, compared to the number who perish from hurricanes or other weather disasters, for example. While permanent memorials are built for soldiers and victims of terror attacks, they are rarely erected for victims or medical heroes of pandemics, despite the far greater death toll.
While the pandemic is still far from over, we must ensure the difficult lessons learned are not forgotten by future generations—as has been the case with previous pandemics.
A National Bureau of Economic Research working paper found that higher-priced hospitals in competitive markets were associated with lower patient mortality—flying in the face of the common policy narrative that higher-priced care is not higher quality. However, in more concentrated, less-competitive healthcare markets (in which over two-thirds of the nation’s hospitals are located), the study found no correlation between price and quality. Authors of the study analyzed patient outcomes from more than 200K admissions among commercially insured patients, transported by ambulance to about 1,800 hospitals between 2007 and 2014.
The Gist: As hospitals have consolidated, prices have risen by about 30 percent between 2015 to 2019, leading policy experts and regulators to search for ways to rein in price inflation.
While there continues to be widespread consensus that industry consolidation has resulted in unsustainable cost growth, the new study’s findings bring a bit of welcome nuance around impact on quality and outcomes to an otherwise one-sided, price-centric policy narrative.
The US healthcare sector added 64K jobs in February, an increase from recent months, but the gains were concentrated in provider offices and home health companies. Hospitals and nursing facilities, which have both struggled with widespread staffing shortages, saw more anemic job growth. In particular, nursing homes have lost 15 percent of their workforce, remaining significantly understaffed even though resident occupancy rates still lag pre-pandemic levels. This week, nursing home groups pushed back against President Biden’s call for minimum staffing levels, calling them unrealistic without federal funding.
The Gist: Hospital and nursing facility workers have taken on some of the most taxing and dangerous jobs during the pandemic, caring for the sickest patients while personally risking COVID infection.
Healthcare workers are increasingly opting for safer, less intense jobs in outpatient care settings like physician offices, or are exiting direct patient care entirely. Even as the pandemic subsides, recruitment and retention of nurses and other caregivers will be of paramount importance, given rising vacancy rates and unabating staff shortages.
Congress cut billions of dollars in COVID-related funding from the broader government spending bill it just passed, jeopardizing President Biden’s plans for covering the costs of COVID testing and treatments, and making antiviral drugs available for free at pharmacies for those who test positive through the “test to treat” initiative.
However, a variety of other healthcare funding made it into the final package, including a five-month extension of COVID-era telehealth flexibilities for Medicare beneficiaries, and funds for pandemic preparedness. Congressional Democrats now plan to pass a separate COVID funding bill, although that effort will likely face stiff opposition from Senate Republicans.
The Gist: Removing COVID funding from the final spending package may signal the beginning of the end of federal pandemic relief spending, and could render the “test to treat” initiative, which has been praised by public health experts, dead on arrival.
Pharmacists, who have taken on a larger role in patient care during the pandemic, assisting with testing and vaccination of millions of Americans, have pushed for the ability to prescribe new antiviral therapies, but the American Medical Association criticized the initiative, maintaining that physicians should control the prescribing. Although the drug interactions and side effects cited by the AMA are important to manage, pharmacy-based “test to treat”would reduce time to treatment for those with COVID, and provide a sustainable mechanism for managing future surges of the disease.
The Democratic presidential primary might feel like a lifetime ago, but one important storyline in that race was health care — specifically single-payer health care, or the policy that the government should offer universal health insurance to everyone in the country. The nomination of now-President Biden, who opposed single-payer health care during the primary, has put single-payer health care on the backburner nationally. But that hasn’t stopped the issue from impacting state legislators, who have introduced more single-payer health care bills in the last few years than ever before.
Health care policy researchers Erin C. Fuse Brown and Elizabeth McCuskey tracked the number of unique single-payer bills introduced in state legislatures across the country from 2010 to 2019, finding a sharp uptick in bills introduced since 2017. During each of those three years, at least 10 single-payer proposals were introduced, according to Brown and McCuskey’s research, for the first time since 2013. In total, state legislators proposed more single-payer bills from 2017 to 2019 than in the previous seven years combined. And for 2021, we’ve identified 10 single-payer bills that legislators introduced across the country, from liberal states like California and Massachusetts to more conservative ones including Iowa and Ohio.1
What do all these proposals have in common? They’ve all universally failed. In fact, Vermont, the only state that managed to pass single-payer health care in 2011, ended up shelving its plan three years later.
It makes sense why single-payer advocates have tried to take these fights to the states. States have traditionally been seen as the “laboratories of democracy,” and some advocates of single-payer health care have argued that liberal states could provide unique opportunities to advance single-payer health care. But as I’ll explain, passing single-payer health care at the state level is next to impossible, as states are particularly limited in how they can allocate federal and private health care funds. There is, however, evidence that Americans may have an appetite for a public option, or government-run health insurance that people can opt into at the state level. Three states (Colorado, Nevada and Washington) have already passed a public option. It’s not single-payer health care reform, but it’s possible that we might see more states adopt their own public-option reforms.
One big reason single-payer proposals haven’t caught on at the state level is because finding a reliable way to pay for such a program is challenging. Single-payer advocates originally envisioned a federal proposal that would cover all Americans under a more generous version of a preexisting program — that is, Medicare, but now for all. Doing this state-by-state would require each state to apply for waivers to divert federal funds used for Medicare, Medicaid and Affordable Care Act exchanges to be used for their own single-payer plans. And that’s tricky because the Department of Health and Human Services has wide discretion to approve or deny states’ requests, which makes any proposal highly dependent on the national political climate.
This isn’t just a theoretical debate either: Trump’s administrator for the Centers for Medicare & Medicaid Services Seema Verma said in 2018 that she would deny waivers from states to create single-payer systems, while Biden’s Health and Human Services Secretary Xavier Becerra has expressed more favorable sentiments. Almost all single-payer proposals depend on these waivers and states don’t often have fallback plans for if this federal funding gets denied.
Employer-sponsored health insurance plans, which cover 54 percent of Americans, are another hurdle for states trying to pass single-payer health care. Federal law largely prevents states from regulating employer-provided health insurance, so states can’t just stop employers from offering their own health care benefits. The exact scope of this law has been litigated for decades, but suffice it to say that it’s successfully put the kibosh on many statewide health care reforms. Single-payer health insurance is particularly tricky as there’s no way to get everyone onto the plan without first changing how private insurance works. States have tried to address this through measures like increasing payroll taxes or restricting providers’ ability to accept reimbursement from private insurance plans. But the more elaborate these mechanisms get, the more complicated it becomes to implement — and the more people that could slip through the cracks.
Finally, another big financial barrier is that state governments have far less leeway than the federal government to increase budgetary spending. That means tax increases, which come with their own political challenges, are often necessary for states to secure the funding they need.
Take California’s single-payer proposal, which failed in late January. It would have required two-thirds of voters to pass a separate constitutional amendment to implement the necessary tax increases to pay for it. Concerns over tax increases also contributed to the demise of single-payer proposals in Colorado and Vermont. It’s true that a recent analysis of New York’s single-payer health care plan found that it would lower overall health care spending by 3 percent by 2031, but it would also require additional state tax revenue of $139 billion in 2022 — over 150 percent of the current state budget. Politicians facing the next election cycle may be leery of proposing short-term tax increases, even if the end result is long-term savings.
All of this creates a daunting picture for statewide single-payer health care. But the failures of single-payer doesn’t entirely close the door on health care reform, especially if these reforms are supplementing the existing system instead of entirely replacing it. Colorado and Nevada, for instance, successfully passed a public option in 2021, joining Washington, which passed one in 2019. Colorado’s success in advancing a public option is particularly striking, given that almost 80 percent of people voted against its single-payer proposal in 2016.
To be sure, though, efforts to implement a public option aren’t without their own challenges. In 2021, during its first year of implementation, Washington state’s public option struggled to enroll people and get health care providers to agree to lower payment rates. State lawmakers have tried to fix this problem by introducing legislation that would require more providers to participate and bring down premiums by increasing subsidies. Proponents have also cautioned that it might take years before the public option really gains a foothold with Washington state residents.
It’s not clear yet how successful these state-run public option plans will be, but it is possible that a public option may prove more popular than single-payer. For starters, while single-payer health care is popular among Democrats, the public option still polls much better among Republicans and independents. According to a Morning Consult/Politico poll from March 2021, the public option was roughly as popular as Medicare for All among Democrats — about 80 percent said they supported each. But support for the public option was much higher than support for Medicare for All among both Republicans and independents. Just 28 percent of Republicans and 50 percent of independents supported Medicare for All versus 56 percent of Republicans and 63 percent of independents who supported a public option.
Ultimately, any health care reforms would be easier to implement on a federal level than a patchwork, state-by-state approach. But Washington, Colorado and Nevada remain important tests of state governments’ ability to implement a public option in lieu of action by the federal government. It’s not single-payer, but it’s still some of the most consequential health care reforms in decades — and a potential sign of where the debates over health care are heading.
The House passed a sweeping spending bill last night that omitted billions in Covid-19 aid. Biden administration officials had said the funds were urgently needed to maintain supplies of essential treatments and support further vaccine development, but Republicans disagreed. Some public health experts have expressed dismay that the pandemic relief money was cut, given the likelihood that new variants will continue to emerge. After all, viruses keep evolving until they run out of hosts to infect, and there are billions of people around the world—and millions in the US—who haven’t been vaccinated against Covid-19.
Cases continue to decline in the US, and a number of top voices in public health recently put out a report mapping when and how the country can transition out of the pandemic. Their recommendations include vaccinating at least 85 percent of the US population by 2023, improving indoor air quality in public buildings, and allocating additional funding for Covid-19 response and to prepare for future pandemics.
Welcome to Friday’s Health 202, where today we have a special spotlight on the pandemic two years in.
🚨 The federal government is about to be funded. The Senate sent the long-term spending bill to President Biden’s desk last night after months of intense negotiations.
Two years since the WHO declared a pandemic, what health-care system changes are here to stay?
Nurses screened patients at a drive-through testing site in March 2020. (Win McNamee/Getty Images)
Exactly two years ago, the World Health Organizationdeclared the coronavirus a pandemic and much of American life began grinding to a halt.
That’s when the health-care system, which has never been known for its quickness, sped up. The industry was forced to adapt, delivering virtual care and services outside of hospitals on the fly. Yet, the years-long pandemic has exposed decades-old cracks in the system, and galvanized efforts to fix them.
Today, as coronavirus cases plummet and President Biden says Americans can begin resuming their normal lives, we explore how the pandemic could fundamentally alter the health-care system for good. What changes are here to stay — and what barriers are standing in the way?
A telehealth boom
What happened: Telehealth services skyrocketed as doctors’ offices limited in-person visits amid the pandemic. The official declaration of a public health emergency eased long-standing restrictions on these virtual services, vastly expanding Medicare coverage.
But will it stick? Some of these changes go away whenever the Biden administration decides not to renew the public health emergency (PHE). The government funding bill passed yesterday extends key services roughly five months after the PHE ends, such as letting those on Medicare access telehealth services even if they live outside a rural area.
But some lobbyists and lawmakers are pushing hard to make such changes permanent. Though the issue is bipartisan and popular, it could be challenging to pass unless the measures are attached to a must-pass piece of legislation.
“Even just talking to colleagues, I used to have to spend three or four minutes while they were trying desperately not to stare at their phone and explain to them what telehealth was … remote patient monitoring, originating sites, and all this wonky stuff,”said Sen. Brian Schatz (D-Hawaii), a longtime proponent of telehealth.
“Now I can go up to them and say, ‘So telehealth is great, right?’ And they say, ‘yes, it is.’ ”
A new spotlight on in-home care
What happened: The infectious virus tore through nursing homes, where often fragile residents share rooms and depend on caregivers for daily tasks. Ultimately, nearly 152,000 residents died from covid-19.
The devastation has sparked a rethinking of where older adults live and how they get the services they need — particularly inside their own homes.
“That is clearly what people prefer,” said Gail Wilensky, an economist at Project HOPE who directed the Medicare and Medicaid programs under President George H.W. Bush. “The challenge is whether or not it’s economically feasible to have that happen.”
More money, please: Finding in-home care — and paying for it — is still a struggle for many Americans. Meanwhile, many states have lengthy waitlists for such services under Medicaid.
Experts say an infusion of federal funds is needed to give seniors and those with disabilities more options for care outside of nursing homes and assisted-living facilities.
For instance, Biden’s massive social spending bill included tens of billions of dollars for such services. But the effort has languished on Capitol Hill, making it unclear when and whether additional investments will come.
A reckoning on racial disparities
What happened: Hispanic, Black, and American Indian and Alaska Native people are about twice as likely to die from covid-19 than White people. That’s according to age-adjusted data from a recent Kaiser Family Foundation report.
In short, the coronavirus exposed the glaring inequities in the health-care system.
“The first thing to deal with any problem is awareness,” said Georges Benjamin, the executive director of the American Public Health Association. “Nobody can say that they’re not aware of it anymore, that it doesn’t exist.”
But will change come? Health experts say they hope the country has reached a tipping point in the last two years. And yet, any real systemic change will likely take time. But, Benjamin said, it can start with increasing the number of practitioners from diverse communities, making office practices more welcoming and understanding biases.
We need to, as a matter of course, ask ourselves who’s advantaged and who’s disadvantaged” when crafting new initiatives, like drive-through testing sites, Benjamin said. “And then how do we create systems so that the people that are disadvantaged have the same opportunity.”