

Cartoon – Welcome to the Club



Kaiser Permanente saw its net income climb more than 68 percent in the third quarter of 2020, according to its financial report released Nov. 6.
The Oakland, Calif.-based health system recorded operating revenue of $22 billion in the quarter ended Sept. 30, up 5.3 percent from the same period a year earlier. Kaiser also saw expenses rise about 5.9 percent year over year, to $21.5 billion.
“Although the pandemic continues to have an impact on Kaiser Permanente, during the third quarter we safely resumed in-person preventive and elective care, started to address the backlog of deferred procedures that were put on hold due to COVID-19, and continued to leverage and grow virtual care for members’ safety and convenience,” said executive vice president and CFO Kathy Lancaster.
The 39-hospital system spent $964 million on capital projects in the third quarter, up from $891 million in the third quarter of 2019.
A lot of the capital spend has been shifted into the IT arena to boost patient and member access to various digital health services such as telehealth, Tom Meier, corporate treasurer of Kaiser, told Becker’s. It also included ongoing multi-year projects and maintenance of its hospitals.
Compared to the third quarter of 2019, Kaiser’s operating income fell 25.9 percent to $456 million.
Largely due to the result of returns in the financial market, the system ended the third quarter of 2020 with a net income of $2 billion. In the same quarter last year, Kaiser recorded a net income of $1.2 billion.
In the third quarter, Kaiser saw its non-operating income reach $1.5 billion, up from $556 million in the third quarter of 2019, Mr. Meier said.
Kaiser also offers a health plan to members across the U.S. As of Sept. 30, Kaiser had 12.4 million health plan members, representing a loss of 11,000 members in the third quarter. The decline was largely attributed to members losing access to their employer-sponsored plan as unemployment went up in the state. However, this decline was offset slightly by members purchasing individual plans or being enrolled in a government-sponsored plan, Mr. Meier said.
For the nine-month period ended Sept. 30, Kaiser reported a net income of $5.4 billion on revenue of $66.6 billion. In the same nine-month period in 2019, the health system recorded a net income of $6.4 billion on revenue of $63.7 billion.
The health system continues to respond to the COVID-19 pandemic. Through the third quarter the system has cared for 185,000 COVID-19 patients and tested nearly 2 million people for the novel virus.

The U.S. Supreme Court is set to hear a case questioning the legality of the ACA on Nov. 10.
Five things to know:
1. At the center of the case is whether the health law should be struck down. In a brief filed June 25 in Texas v. United States, the Trump administration argues the entire ACA is invalid because in December 2017, Congress eliminated the ACA’s tax penalty for failing to purchase health insurance. The administration argues the individual mandate is inseverable from the rest of the law and became unconstitutional when the tax penalty was eliminated; therefore, the entire health law should be struck down.
2. The administration’s brief was filed in support of a group of Republican-led states seeking to undo the ACA. Meanwhile, California Attorney General Xavier Becerra is leading a coalition of more Democratic states to defend the ACA before the Supreme Court.
3. The case goes before the Supreme Court days after media outlets projected Joe Biden as the next president of the U.S. President-elect Biden has said he seeks to expand government-subsidized insurance coverage and wants to the bring back the ACA’s tax penalty for failing to purchase health insurance, according to The Wall Street Journal. If a change regarding the tax penalty did occur, the publication notes that Republicans’ argument on severability would no longer apply.
4. The case also goes before the Supreme Court about two weeks after the Senate voted Oct. 26 to confirm Amy Coney Barrett to the Supreme Court. Ms. Barrett previously criticized Chief Justice John Roberts’ 2012 opinion sustaining the law’s individual mandate, The New York Times reported, but she said during her confirmation hearings in October that “the issue in the case is this doctrine of severability, and that’s not something that I have ever talked about with respect to the Affordable Care Act.”
5. According to the Journal, the Supreme Court is not expected to make a decision in the case until the end of June.
https://www.pwc.com/us/Biden2020healthagenda

President-elect Joe Biden’s healthcare agenda: building on the ACA, value-based care, and bringing down drug prices.
In many ways, Joe Biden is promising a return to the Obama administration’s approach to healthcare:
Bolder ideas, such as developing a public option, resolving “surprise billing,” allowing for negotiation of drug prices by Medicare, handing power to a third party to help set prices for some life sciences products, and raising the corporate tax rate, could be more challenging to achieve without overwhelming majorities in both the House and the Senate.
Biden is likely to mount an intensified federal response to the COVID-19 pandemic, enlisting the Defense Production Act to compel companies to produce large quantities of tests and personal protective equipment as well as supporting ongoing deregulation around telehealth. The Biden administration also will likely return to global partnerships and groups such as the World Health Organization, especially in the area of vaccine development, production and distribution.
Broadly, healthcare executives can expect an administration with an expansionary agenda, looking to patch gaps in coverage for Americans, scrutinize proposed healthcare mergers and acquisitions more aggressively and use more of the government’s power to address the pandemic. Executives also can expect, in the event the ACA is struck down, moves by the Biden administration and Democratic lawmakers to develop a replacement. Healthcare executives should scenario plan for this unlikely yet potentially highly disruptive event, and plan for an administration marked by more certainty and continuity with the Obama years.
All healthcare organizations should prepare for the possibility that millions more Americans could gain insurance under Biden. His proposals, if enacted, would mean coverage for 97% of Americans, according to his campaign website. This could mean millions of new ACA customers for payers selling plans on the exchanges, millions of new Medicaid beneficiaries for managed care organizations, millions of newly insured patients for providers, and millions of covered customers for pharmaceutical and life sciences companies. The surge in insured consumers could mirror the swift uptake in the years following the passage of the ACA.
Biden is expected to draw on his experience from H1N1 and the Ebola outbreaks to address the COVID-19 pandemic with a more active role for the federal government, which many Americans support. These actions could shore up the nation’s response in which the federal government largely served in a support role to local, state and private efforts.
Three notable exceptions have been the substantial federal funding for development of vaccines against the SARS-CoV-2 virus, Congress’ aid packages and the rapid deregulatory actions taken by the FDA and CMS to clear a path for medical products to be enlisted for the pandemic and for providers, in particular, to be able to respond to it.
The US health system has been slowly transforming for years into a New Health Economy that is more consumer-oriented, digital, virtual, open to new players from outside the industry and focused on wellness and prevention. The COVID-19 pandemic has accelerated some of those trends. Once the dust from the election settles, companies that have invested in capabilities for growth and are moving forcefully toward the New Health Economy stand to gain disproportionately.
The Trump administration made limiting the flow of immigrants to the US a priority. The associated policy changes have the potential to exacerbate shortages of physicians, nurses and other healthcare workers, including medical students. These consequences have been aggravated by the pandemic, which dramatically curtailed travel into the US.
Biden and lawmakers from both parties have been raising questions about life sciences’ supply chains. This focus has only intensified because of the pandemic and resulting shortages of personal protective equipment (PPE), pharmaceuticals, diagnostic tests and other medical products.
Presidents and lawmakers have been talking about drug prices for decades; few truly meaningful actions have been implemented. Biden has made drug pricing reform a priority.
While the pandemic delayed many of the federal interoperability rule deadlines, payers and providers should use the extra time to plan strategically for an interoperable future.
Health organizations should review their policies and consider whether they offer protections for customers under the new processes and what data security risks may emerge. They should also consider whether business associate agreements are due in more situations.
The pandemic has thrown millions out of work, generating many new customers for ACA plans just as the incoming Biden administration plans to enrich subsidies, making more generous plans within reach of more Americans.
Lawmakers and politicians often use bold language, and propose bold solutions to problems, but the government and the industry itself resists sudden, dramatic change, even in the face of sudden, dramatic events such as a global pandemic. One notable exception to this would be a decision by the US Supreme Court to strike down the ACA, an event that would generate a great deal of uncertainty and disruption for Americans, the US health industry and employers.

The financial challenges caused by the COVID-19 pandemic have forced hundreds of hospitals across the nation to furlough, lay off or reduce pay for workers, and others have had to scale back services or close.
Lower patient volumes, canceled elective procedures and higher expenses tied to the pandemic have created a cash crunch for hospitals. U.S. hospitals are estimated to lose more than $323 billion this year, according to a report from the American Hospital Association. The total includes $120.5 billion in financial losses the AHA predicts hospitals will see from July to December.
Hospitals are taking a number of steps to offset financial damage. Executives, clinicians and other staff are taking pay cuts, capital projects are being put on hold, and some employees are losing their jobs. More than 260 hospitals and health systems furloughed workers this year and dozens of others have implemented layoffs.
Below are 11 hospitals and health systems that announced layoffs since Sept. 1, most of which were attributed to financial strain caused by the pandemic.
1. NorthBay Healthcare, a nonprofit health system based in Fairfield, Calif., is laying off 31 of its 2,863 employees as part of its pandemic recovery plan, the system announced Nov. 2.
2. Minneapolis-based Children’s Minnesota is laying off 150 employees, or about 3 percent of its workforce. Children’s Minnesota cited several reasons for the layoffs, including the financial hit from the COVID-19 pandemic. Affected employees will end their employment either Dec. 31 or March 31.
3. Brattleboro Retreat, a psychiatric and addiction treatment hospital in Vermont, notified 85 employees in late October that they would be laid off within 60 days.
4. Citing a need to offset financial losses, Minneapolis-based M Health Fairview said it plans to downsize its hospital and clinic operations. As a result of the changes, 900 employees, about 3 percent of its 34,000-person workforce, will be laid off.
5. Lake Charles (La.) Memorial Health System laid off 205 workers, or about 8 percent of its workforce, as a result of damage sustained from Hurricane Laura. The health system laid off employees at Moss Memorial Health Clinic and the Archer Institute, two facilities in Lake Charles that sustained damage from the hurricane.
6. Burlington, Mass.-based Wellforce laid off 232 employees as a result of operating losses linked to the COVID-19 pandemic. The health system, comprising Tufts Medical Center, Lowell General Hospital and MelroseWakefield Healthcare, experienced a drastic drop in patient volume earlier this year due to the suspension of outpatient visits and elective surgeries. In the nine months ended June 30, the health system reported a $32.2 million operating loss.
7. Baptist Health Floyd in New Albany, Ind., part of Louisville, Ky.-based Baptist Health, eliminated 36 positions. The hospital said the cuts, which primarily affected administrative and nonclinical roles, are due to restructuring that is “necessary to meet financial challenges compounded by COVID-19.”
8. Cincinnati-based UC Health laid off about 100 employees. The job cuts affected both clinical and non-clinical staff. A spokesperson for the health system said no physicians were laid off.
9. Mercy Iowa City (Iowa) announced in September that it will lay off 29 employees to address financial strain tied to the COVID-19 pandemic.
10. Springfield, Ill.-based Memorial Health System laid off 143 employees, or about 1.5 percent of the five-hospital system’s workforce. The health system cited financial pressures tied to the pandemic as the reason for the layoffs.
11. Watertown, N.Y.-based Samaritan Health announced Sept. 8 that it laid off 51 employees and will make other cost-cutting moves to offset financial stress tied to the COVID-19 pandemic.

A promising vaccine developed by drug giant Pfizer and German biotechnology firm BioNTech would need to be stored at ultracold temperatures that experts say could make it far more difficult to distribute than other potential vaccines.
Pfizer announced Monday that an interim analysis had shown the vaccine was more than 90 percent effective, news that was greeted with near universal celebration among experts.
But the Pfizer vaccine is relatively unusual as it has to be stored and transported at an ultracold temperature of around -94 Fahrenheit (-70 Celsius), significantly complicating the process of getting the vaccine to people.
Ultracold storage is “is not necessarily routinely available in most health centers even in the U.K., let alone globally,” Michael Head, a fellow in global health at the University of Southampton said in a statement.
Vaccines often require some kind of cold storage to remain effective; some candidates for a coronavirus vaccine need to be held at cooler temperatures like 26 Fahrenheit (2 Celsius). They need to be kept this temperature not only while in storage but also while being delivering on planes and trucks.
The Pfizer vaccine would be considerably colder, requiring more than just refrigeration but something capable of producing freezing temperatures even during potential lengthy periods of transport. It has been done before, though at a smaller scale: A vaccine for the Ebola virus was notable for requiring ultracold storage. Pfizer has been preparing for the challenge by creating special containers that can last 10 days at -94 Fahrenheit, according to the Wall Street Journal.
Groups like the World Health Organization and UNICEF have said that countries need to improve their “cold chain” logistical networks to make sure vaccines can be distributed safely. The Associated Press reported last month that nearly 3 billion people live in areas where temperature-controlled storage is insufficient for the task.
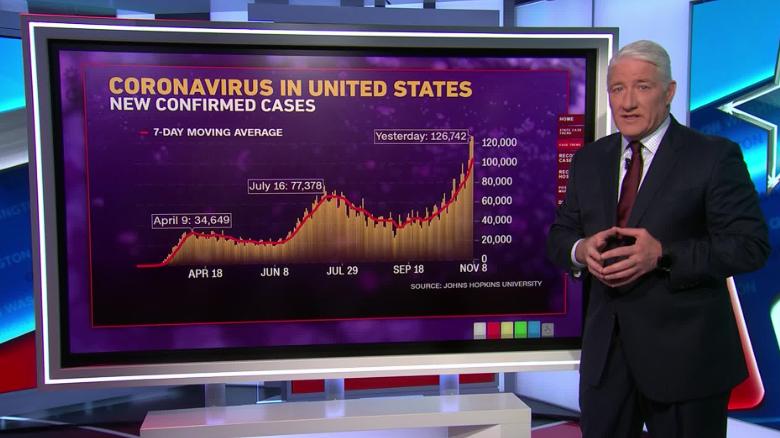
The United States surpassed 10 million coronavirus cases on Monday, just 10 days after hitting 9 million. The average number of daily new infections has exceeded 100,000, and public health experts warn the country is entering the pandemic’s worst phase yet.
The United States hit the milestone as Pfizer announced its coronavirus vaccine candidate was more than 90 percent effective, compared with a placebo. Epidemiologists and health experts were optimistic about the results, but also cautioned that more information is needed on the vaccine’s long-term efficacy and safety.

