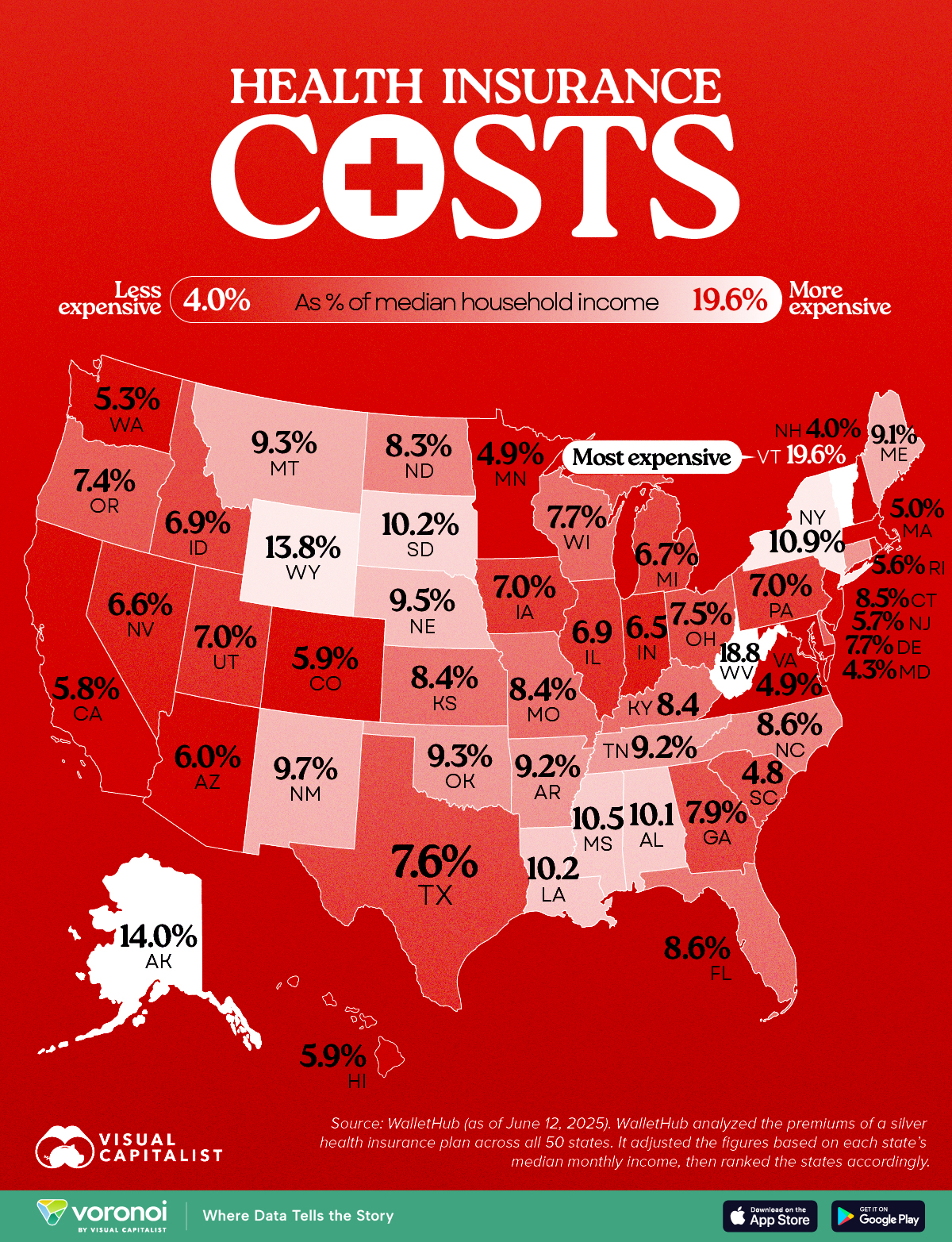
Health Insurance as a Share of Median Income by U.S. State
This was originally posted on our Voronoi app. Download the app for free on iOS or Android and discover incredible data-driven charts from a variety of trusted sources.
Key Takeaways
Vermont tops the list, with insurance costing 19.6% of median income.
New Hampshire residents spend just 4% of their income on health insurance, the lowest in the nation.
Americans pay wildly different amounts for health insurance depending on where they live. This map shows which states pay the most (and least) when health insurance costs are measured as a share of median income.
The data for this visualization comes from WalletHub. It analyzed silver-tier health plan premiums in all 50 states and compared them to local median incomes to determine cost burdens.
Vermont and West Virginia Lead in Cost Burden
In Vermont, residents spend 19.6% of their monthly income on health insurance, the highest share in the country. West Virginia follows closely at 18.8%.
The South and Mountain West Feel the Pinch
Many Southern and Mountain West states, like Mississippi, Wyoming, and Louisiana, also rank high in insurance cost burden. These regions tend to have poorer health outcomes and lower median incomes, exacerbating affordability issues. As Brookings notes, Medicaid expansion status and rural demographics heavily influence insurance markets in these areas.
New Hampshire and the Northeast Are Least Burdened
New Hampshire residents spend just 4% of their income on health insurance, the lowest in the nation.
Massachusetts, Maryland, and Minnesota also enjoy low cost burdens. These states often have robust state-run exchanges, higher incomes, and broader Medicaid expansion, all of which help reduce costs.
Medicaid cuts have received the lion’s share of attention from critics of Republicans’ sweeping tax cuts legislation, but the GOP’s decision not to extend enhanced ObamaCare subsidies could have a much more immediate impact ahead of next year’s midterms.
Extra subsidies put in place during the coronavirus pandemic are set to expire at the end of the year, and there are few signs Republicans are interested in tackling the issue at all.
To date, only Sens. Lisa Murkowski (R-Alaska) and Thom Tillis (R-N.C.) have spoken publicly about wanting to extend them.
The absence of an extension in the “big, beautiful bill” was especially notable given the sweeping changes the legislation makes to the health care system, and it gives Democrats an easy message: If Republicans in Congress let the subsidies expire at the end of the year, premiums will spike, and millions of people across the country could lose health insurance.
In a statement released last month as the House was debating its version of the bill, House and Senate Democratic health leaders pointed out what they said was GOP hypocrisy.
“Their bill extends hundreds of tax policies that expire at the end of the year. The omission of this policy will cause millions of Americans to lose their health insurance and will raise premiums on 24 million Americans,” wrote Senate Finance Committee ranking member Ron Wyden (D-Ore.), House Ways and Means Committee ranking member Richard Neal (D-Mass.) and House Energy and Commerce Committee ranking member Frank Pallone (D-N.J.).
“The Republican failure to stop this premium spike is a policy choice, and it needs to be recognized as such.”
More than 24 million Americans are enrolled in the insurance marketplace this year, and about 90 percent — more than 22 million people — are receiving enhanced subsidies.
“All of those folks will experience quite large out-of-pocket premium increases,” said Ellen Montz, who helped run the federal ObamaCare exchanges under the Biden administration and is now a managing director with Manatt Health.
“When premiums become less affordable, you have this kind of self-fulfilling prophecy where the youngest and the healthiest people drop out of the marketplace, and then premiums become even less affordable in the next year,” Montz said.
The subsidies have been an extremely important driver of ObamaCare enrollment. Experts say if they were to expire, those gains would be erased.
According to the Congressional Budget Office (CBO), 4.2 million people are projected to lose insurance by 2034 if the subsidies aren’t renewed.
Combined with changes to Medicaid in the new tax cut law, at least 17 million Americans could be uninsured in the next decade.
The enhanced subsidies increase financial help to make health insurance plans more affordable. Eligible applicants can use the credit to lower insurance premium costs upfront or claim the tax break when filing their return.
Premiums are expected to increase by more than 75 percent on average, with people in some states seeing their payments more than double, according to health research group KFF.
Devon Trolley, executive director of Pennie, the Affordable Care Act (ACA) exchange in Pennsylvania, said she expects at least a 30 percent drop in enrollment if the subsidies expire.
The state starts ramping up its open enrollment infrastructure in mid-August, she said, so time is running short for Congress to act.
“The only vehicle left for funding the tax credits, if they were to extend them, would be the government funding bill with a deadline of September 30, which we really see as the last possible chance for Congress to do anything,” Trolley said.
Trolley said three-quarters of enrollees in the state’s exchange have never purchased coverage without the enhanced tax credits in place.
“They don’t know sort of a prior life of when the coverage was 82 percent more expensive. And we are very concerned this is going to come as a huge sticker shock to people, and that is going to significantly erode enrollment,” Trolley said.
The enhanced subsidies were first put into effect during the height of the coronavirus pandemic as part of former President Biden’s 2021 economic recovery law and then extended as part of the Inflation Reduction Act.
The CBO said permanently extending the subsidies would cost $358 billion over the next 10 years.
Republicans have balked at the cost. They argue the credits hide the true cost of the health law and subsidize Americans who don’t need the help. They also argue the subsidies have been a driver of fraudulent enrollment by unscrupulous brokers seeking high commissions.
Sen. Bill Cassidy (R-La.), chair of the Senate Health, Education, Labor and Pensions Committee, last year said Congress should reject extending the subsidies.
The Republican Study Committee’s 2025 fiscal budget said the subsidies “only perpetuate a never-ending cycle of rising premiums and federal bailouts — with taxpayers forced to foot the bill.”
But since 2020, enrollment in the Affordable Care Act marketplace has grown faster in the states won by President Trump in 2024, primarily rural Southern red states that haven’t expanded Medicaid. Explaining to millions of Americans why their health insurance premiums are suddenly too expensive for them to afford could be politically unpopular for Republicans.
According to a recent KFF survey, 45 percent of Americans who buy their own health insurance through the ACA exchanges identify as Republican or lean Republican. Three in 10 said they identify as “Make America Great Again” supporters.
“So much of that growth has just been a handful of Southern red states … Texas, Florida, Georgia, the Carolinas,” said Cynthia Cox, vice president at KFF and director of the firm’s ACA program. “That’s where I think we’re going to see a lot more people being uninsured.”
Health insurers and their lobbying arms have spent $476.5 million since 2020 to block reform, protect profits, and mislead the public — and it’s coming straight from our premiums and tax dollars.
AHIP, the big PR and lobbying outfit for most health insurers, undoubtedly believes the praise it got from Trump administration officials and some members of Congress this week – when it announced changes insurers presumably will make voluntarily to alleviate the burden of prior authorization demands on patients and health care providers – has taken the heat off insurers. AHIP’s message to Washington politicos: You don’t need to pass any new laws to make us do the right thing. You can trust us, despite our decades of engaging in untrustworthy behavior to maximize profits.
After all, AHIP is nothing more than a PR and lobbying shop with millions of our dollars to play with. It has zero ability to force insurers to do what AHIP claims they will do. I know this because I worked closely with AHIP during my 20 years in the industry and represented Cigna on its strategic communications committee.
From Fox to “Fixer”?
AHIP pulled off its big show on Monday – and got plenty of generally fawning press coverage – because of all the money it and affiliated insurers throw around Washington every year to protect what has become an incredibly profitable status quo.
Collectively, the seven biggest for-profit insurers reported $70 billion in profits last year.
(Beleauered UnitedHealth alone reported $34.4 million in operating earnings.) And that’s just seven among dozens. One way they make that kind of dough, for their shareholders and top executives, is by using prior authorization to avoid paying for patients’ medically necessary care. Many people die as a result, while investors get richer. It’s that simple and that cold.
So just how much money does AHIP and the insurance industry spend to bamboozle members of Congress and the White House every year? We’re talking stupid money. And orders of magnitude more than nonprofits that advocate for reforms that would benefit patients instead of shareholders.
Nearly Half a Billion Ways They Tip the Scale
To find out just how much, I turned to OpenSecrets and did some math. OpenSecrets, as a reminder, is the well-named organization that keeps tabs on campaign contributions and lobbying expenses.
What I discovered is that AHIP has spent almost $65 million lobbying Congress and the Biden and Trump administrations since 2020. Its cousin, the Blue Cross Blue Shield Association, has spent even more. More than twice as much more.
And that, folks, is just the tip of the iceberg, and it doesn’t even include the tens of millions the industry spends on massive advertising campaigns inside the DC beltway that it’s not required to report. Or the dark money ads and advocacy the industry bankrolls.
But just the lobbying totals are mind-blowing. When you factor in the money spent by the big seven insurers and the other PR and lobbying groups that insurers funnel money to, the total grows to almost $500 million. You read that right: nearly half a billion dollars.
Most of that spending was during the Biden administration, but the industry is on track to break spending records during the first year of the current Trump administration. They are lobbying not only to beat back new laws and regulations that could constrain their prior authorization practices but also to protect their biggest cash cows: Medicare Advantage and their pharmacy benefit managers (PBMs).
Three PBMs – owned by Cigna, CVS/Aetna and UnitedHealth –control 80% of the pharmacy benefit market and determine which drugs we’ll have access to and how much we have to pay out of pocket even with insurance.
The Big Number
$476.5 million – That’s the amount of money health insurance corporations and four of their PR and lobbying groups – AHIP, BCBSA (which includes contributions from Elevance/Anthem as well as numerous other BCBS companies), the Pharmaceutical Care Management Association and the Better Medicare Alliance – have collectively spent on lobbying Congress and federal regulators between January 1, 2020, and March 31, 2025.
Keep in mind that that money is not coming out of executives’ paychecks. It’s coming out of our pockets. Insurers skim money from our premiums and taxes to finance their propaganda and lobbying efforts to keep the gravy train rolling. And it’s in addition to all the campaign cash they dole out every year, which I tabulated recently.
This is not to say that reform is impossible. Scrappy advocacy groups with a tiny fraction of that total have scored important victories over the years. But it is why progress is so slow and setbacks are so frequent.
But just imagine how all that money could be put to better use to ensure that all Americans, including those with insurance, are able to get the care they need when they need it. It’s clear that in addition to reforming our health care system, we need political reforms that make it more difficult for big corporations and their trade groups to influence elections and public policy.
New Medicaid funding rules proposed by Congress this week would halt efforts at the state level to better fund rural hospitals and deliver services to the most vulnerable populations in those areas. You can be certain that the administrators and staff of those hospitals, as well as leaders of the communities they serve, are watching closely to see if the cuts are enacted.
Lawmakers at the federal level are trying to make deeper cuts to Medicaid spending in an effort to lower the amount of deficit spending that would be created by President Trump’s spending plan. Trump has dubbed the plan his “big beautiful bill.”
Feds Would Strip Rural Hospitals of Lifeline Funds
Republican members of the Senate Finance Committee this week released their version of the bill that would drain funding for rural hospitals, which rely heavily on Medicaid funds to treat patients. It’s estimated that 25 to 40 percent of services provided by such hospitals are funded by Medicaid.
The federal government and states share the up-front medical costs for Medicaid patients. The federal government then reimburses states up to 50 percent of their Medicaid spending every year.
Many states fund their portion of the cost by taxing entities that provide those services to Medicaid patients.
The latest proposal in Congress would not only restrict how many patients could receive benefits, but it would also stop states from implementing those provider tax programs to help fund Medicaid services provided to residents.
At the federal level, the thinking is that if states keep taxing providers to fund Medicaid services, then the federal government will have to keep reimbursing states a portion of those costs.
The downside to that is many experts, along with several Republicans in Congress, namely Sens. Susan Collins of Maine, Lisa Murkowski of Alaska and Josh Hawley of Missouri, have predicted it will decimate rural hospitals.
West Virginia Republican Sen. Jim Justice went a step further, saying that the plan to limit states’ use of provider taxes will “really hurt a lot of folks.” Despite that statement, Justice said he is OK with the freeze.
State Lawmakers Sound the Alarm
There are 39 states with at least three or more provider taxes used to help fund Medicaid services. Alaska is the only state with no such tax.
Some states, such as Ohio, have set up a new rural hospital fund using provider taxes to help rural hospitals deliver Medicaid services to patients.
Ohio Governor Mike DeWine and the Republican-led state legislature set up a pilot program called the Rural Ohio Hospital Tax Pilot Program. The measure would allow counties to levy a tax on their local hospitals that would then be used to fund Medicaid services.
DeWine said the pilot program would help ease the financial stress rural hospitals face in Ohio. The plan contained in Ohio House Bill 96 has the blessing of the Ohio Hospital Association.
A group of Republican state lawmakers recently sent a letter to their federal counterparts pleading with them to remove the bill language because it would “torpedo” plans to keep rural hospitals functioning.
The American Hospital Association, a 130-year-old trade group of more than 5,000 hospitals and health care providers, this month released the impact on rural hospitals if this plan went into effect.
More than $50 billion would be lost by 2034, and more than 1.8 million rural Americans would lose health benefits.
Kentucky residents would be impacted the most, with 143,000 losing benefits, followed by 135,000 Californians. More than 86,000 Ohioans would lose Medicaid coverage under the plan by 2034, making it the third most impacted state.
To blunt the effects of the cuts, Collins reportedly is proposing the establishment of a $100 billion relief fund that could provide financial support to affected providers, rural hospitals in particular. Whether that or a similar but smaller fund will wind up in the final draft of the legislation apparently will be decided this weekend. Meanwhile, the Senate parliamentarian has ruled against many of the provisions of the Senate version of the bill, including the Finance Committee’s provider tax framework, which puts the whole thing in flux.
Senate leaders say they plan a long series of votes on amendments of the bill on Sunday. The “vote-arama” likely will go on throughout Sunday night and into Monday. If the Senate does pass its version of the bill, it will have to go back to the House. Lawmakers are under a self-imposed deadline to get the legislation to Trump by the July 4 holiday.
Medicaid serves as a vital source of health insurance coverage for Americans living in rural areas, including children, parents, seniors, individuals with disabilities, and pregnant women. Congressional lawmakers are currently considering more than $800 billion in cuts to the Medicaid program, which would reduce Medicaid funding and terminate coverage for vulnerable Americans.
The proposed changes would also result in a significant reduction in Medicaid reimbursement that could result in rural hospital closures.
The National Rural Health Association recently partnered with experts from Manatt Health to shed light on the potential impacts of those cuts on rural residents and the hospitals that care for them over the next decade.
NRHA held a press conference on June 24 that can be accessed with passcode MBTZf4$H. NRHA chief policy officer Carrie Cochran-McClain discussed the findings with Manatt Health partner and former deputy administrator at CMS Cindy Mann and the real world implications of the details of this report with three NRHA member hospital and health system leaders
Report findings provide insight into the impact on rural America at a critical moment in the Congressional debate over the future of the reconciliation package.
The report shows the significant impact from coverage losses that rural communities will face given:
Medicaid plays an outsized role in rural America, covering a larger share of children and adults in rural communities than in urban ones.
Nearly half of all children and one in five adults in small towns and rural areas rely on Medicaid or CHIP for their health insurance.
Medicaid covers nearly one-quarter of women of childbearing age and finances half of all births in these communities.
According to Manatt’s estimates, rural hospitals will lose 21 cents out of every dollar they receive in Medicaid funding due to the One Big Beautiful Bill Act. Total cuts in Medicaid reimbursement for rural hospitals—including both federal and state funds—over the ten-year period outlined in the bill would reach almost $70 billion for hospitals in rural areas.
Reductions in Medicaid funding of this magnitude would likely accelerate rural hospital closures and reduce access to care for rural residents, exacerbating economic hardship in communities where hospitals are major employers.
As a key insurer in rural communities, Medicaid provides a financial lifeline for rural health care providers — including hospitals, rural health clinics, community health centers, and nursing homes—that are already facing significant financial distress. These cuts may lead to more hospitals and other rural facility closures, and for those rural hospitals that remain open, lead to the elimination or curtailment of critical services, such as obstetrics.
“Medicaid is a substantial source of federal funds in rural communities across the country. The proposed changes to Medicaid will result in significant coverage losses, reduce access to care for rural patients, and threaten the viability of rural facilities,” said Alan Morgan, CEO of the National Rural Health Association.
“It’s very clear that Medicaid cuts will result in rural hospital closures resulting in loss of access to care for those living in rural America.”
A media briefing will be held on Tuesday, June 24, from noon to 1:00 PMEST to provide more information about the analysis. This event will feature representatives from NRHA, Manatt Health, and rural hospital leaders across the country. Questions may be submitted in advance, as well as during the press conference. To register for and join the media briefing, click on the Zoom link here.
NRHA is a non-profit membership organization that provides leadership on rural health issues with tens of thousands of members nationwide. Our membership includes nearly every component of rural America’s health care, including rural community hospitals, critical access hospitals, doctors, nurses, and patients. We work to improve rural America’s health needs through government advocacy, communications, education, and research. Learn more about the association at RuralHealth.US.
About Manatt Health
Manatt Health is a leading professional services firm specializing in health policy, health care transformation, and Medicaid redesign. Their modeling draws upon publicly available state data including Medicaid financial management report data from the Centers for Medicare and Medicaid Services, enrollment and expenditure data from the Medicaid Budget and Expenditure System, and data from the Medicaid and CHIP Payment and Access Commission. The Manatt Health Model is tailored specifically to rural health and has been reviewed in consultation with states and other key stakeholders.
The Supreme Court on Friday upheld a key Affordable Care Act requirement that insurance companies cover certain preventative measures recommended by an expert panel.
Justices upheld the constitutionality of the provision in a 6-3 decision and protected access to preventative care for about 150 million Americans.
The justices found that the secretary of the Department of Health and Human Services has the power to appoint and fire members of the U.S. Preventative Services Task Force (USPSTF).
The cases started when a small business in Texas and some individuals filed a lawsuit against the panel’s recommendation that pre-exposure prophylaxis (PreP) for HIV be included as a preventative care service.
They argued that covering PreP went against their religious beliefs and would “encourage homosexual behavior, intravenous drug use, and sexual activity outside of marriage between one man and one woman.”
The plaintiffs further argued that the USPSTF mandates are unconstitutional because panel members are “inferior officers” who are not appointed by the president or confirmed by the Senate.
While the panel is independent, they said that since their decisions impact millions of people members should be confirmed.
A U.S. district judge in 2023 ruled that all preventative-care coverage imposed since the ACA was signed into law areinvalid and a federal appeals court judge ruled in agreement last year.
The Biden administration appealed the rulings to the Supreme Court, and the Trump administration chose to defend the law despite its long history of disparaging Obamacare.
Though public health groups celebrated the ruling Friday, some noted another potential outcome.
“While this is a foundational victory for patients, patients have reason to be concerned that the decision reaffirms the ability of the HHS secretary, including our current one, to control the membership and recommendations of the US Preventive Services Task Force that determines which preventive services are covered,” Anthony Wright, executive director of Families USA, said in a statement.
“We must be vigilant to ensure Secretary Kennedy does not undo coverage of preventive services by taking actions such as his recent firing of qualified health experts from the CDC’s independent vaccine advisory committee and replacing them with his personal allies.”
Last Thursday, the Make America Healthy Again Commission released its 68-page report “Making America’s Children Healthy Again Assessment” featuring familiar themes—the inadequacy of attention to chronic disease by the health system, the “over-medicalization” of patient care vis a vis prescription medicines et al, the contamination of the food-supply by harmful ingredients, and more.
HHS Secretary Kennedy, EPA Administrator Zeldin and Agriculture Secretary Rollins pledged war on the corporate healthcare system ‘that has failed the public’ and an all-of-government approach to remedies for burgeoning chronic care needs.
Also Thursday, the House of Representatives passed its budget reconciliation bill by a vote of 215-214. The 1000-page bill cuts federal spending by $1.6 trillion (including $698 billion from Medicaid) and adds $2.3 trillion (CBO estimate/$3.4 to $5 trillion per Yale Budget Lab) to the national deficit over the next decade. It now goes to the Senate where changes to reduce federal spending to pre-pandemic level will be the focus.
With a 53-37 advantage and 22 of the 36 Senate seats facing mid-term election races in November, 2026, the Senate Republican version of the “Big Beautiful Bill” will include more spending cuts while pushing more responsibility to states for funding and additional cuts. The gap between the House and Senate versions will be wider than currently anticipated by House Republicans potentially derailing the White House promise of a final Big Beautiful Bill by July 4.
And, over the last week and holiday weekend, the President announced a new 25% tariff on Apple devices manufactured in India and new tariffs targeting the EU; threatened cuts to federal grants to Harvard and cessation of its non-citizen student enrollment, a ‘get-tougher’ policy on Russia to pressure an end of its Ukraine conflict, and a pledge to Americans on Memorial that it will double down on ‘peace thru strength’ in its Make America Great Again campaign.
These have 2 things in common:
1-They’re incomplete. None is a finished product.
The MAHA Commission, working with the Departments of Health & Human Services, Interior and Agriculture, is tasked to produce another report within 90 days to provide more details about a plan. The FY26 budgeting process is wrought with potholes—how to satisfy GOP deficit hawks vs. centrist lawmakers facing mid-term election, how to structure a bill that triggers sequestration cuts to Medicare (projected $490 billion/10 yrs. per CBO), how to quickly implement Medicaid work requirements and marketplace enrollment cuts that could leave insurance coverage for up to 14 million in limbo, and much more. And the President’s propensity to “flood the zone” with headline-grabbing Truth Social tweets, Executive Orders and provocative rhetoric on matters at home and abroad will keep media occupied and healthcare spending in the spotlight.
2-They play to the MAGA core.
The MAGA core is primarily composed of older, white, Christian men driven by a belief that the United States has lost its exceptionalism through WOKE policies i.e. DEI in workplaces and government, open borders, globalization and excessive government spending and control. In the 2024 Presidential election, the MAGA core expanded incrementally among Black, Hispanic, and younger voters whose concerns about food, energy and housing prices prompted higher-than expected turnout. The MAGA core believes in meritocracy, nationalism, smaller government, lower taxes, local control and free-market policies that encourage private investment in the economy. The core is price sensitive.
The health system per se is not a concern but it’s the affordability and lack of price transparency are. They respect doctors and frontline caregivers but think executives are overpaid and prone to self-promotion. And the MAGA core think lawmakers have been complicit in the system’s lack of financial accountability largely beneficial to elites.
Looking ahead to the summer, a “Big Beautiful Bill” will pass with optics that allow supporters to claim fiscal constraint and lower national debt and opponents to decry insensitive spending cuts and class warfare against low-and-middle-class households.
Federal cuts to Medicaid and SNAP (Supplemental Nutrition Assistance Program) will be prominent targets in both groups—one a portrayal of waste, fraud and abuse and the other tangible evidence of societal inequity and lack of moral purpose. Each thinks the other void of a balanced perspective. Each thinks the health system is underperforming and in need of transformational change but agreement about how to get there unclear.
As MAHA promotes its agenda, Congress passes a budget and MAGA advances its anti-establishment agenda vis a vis DOGE et al, healthcare operators will be in limbo. The dust will settle somewhat this summer, but longer-term bets will be modified for most organizations as compliance risks change, state responsibilities expand, capital markets react and Campaign 2026 unfolds.
And in most households, concern about the affordability of medical care will elevate as federal and state funding cuts force higher out of pocket costs on consumers and demand for lower prices.
The summer will be busy for everyone in healthcare.
PS: Changes in the housing market are significant for healthcare: 36% of the CPI is based on shelter vs. 8% for medical services & products, 14% for food and 6% for energy/transportation. While the overall CPI increased 2.3% in the last 12 months, medical services prices increased 3.1%. contributing to heightened price sensitivity and delayed payments.
It has not escaped lawmaker attention: revenue cycle management business practices (debt collection) are being scrutinized in hospitals and community benefit declarations by not-for-profit hospitals re-evaluated. The economics of healthcare are not immune to broader market trends nor is spending for healthcare in households protected from day-to-day fluctuations in prices for other goods and services.
The U.S. health care industry is approaching a critical inflection point, according to veteran health care strategist Paul Keckley. In a candid and thought-provoking keynote at the 2025 Healthcare Marketing & Physician Strategies Summit (HMPS) in Orlando, Keckley outlined the challenges and potential opportunities health care leaders must navigate in an era of unprecedented economic uncertainty, regulatory disruption, and consumer discontent.
Drawing on decades of policy experience and his signature candid style, Keckley delivered a sobering yet actionable assessment of where the industry stands and what lies ahead.
Paul Keckley, PhD, health care research and policy expert and managing editor of The Keckley Report
Health care now accounts for a staggering 28 percent of the federal budget, with Medicaid expenditures alone ranging from the low 20s to 34 percent of individual state budgets. Despite its fiscal significance, Keckley points out that health care remains “not really a system, but a collection of independent sectors that cohabit the economy.”
In the article that follows, Keckley warns of a reckoning for those who remain entrenched in legacy assumptions. On the flip side, he notes, “The future is going to be built by those who understand the consumer, embrace transparency, and adapt to the realities of a post-institutional world.”
A Fractured System in a Fractured Economy
Fragmentation complicates any effort to meaningfully address rising costs or care quality. It also heightens the stakes in a political climate marked by what Keckley termed “MAGA, DOGE, and MAHA” factions, shorthand for various ideological forces shaping health care policy under the Trump 2.0 administration.
Meanwhile, macroeconomic conditions are only adding to the strain. At the time of Keckley’s address, the S&P 500 was down 8 percent, the Dow down 10 percent, and inflationary pressures were squeezing both provider margins and household budgets.
“Economic uncertainty is not just about Wall Street,” Keckley warns. “It’s about kitchen-table economics — how households decide between paying for care or paying the cable bill.”
Traditional Forecasting Is Failing
One of Keckley’s key messages was that conventional methods of strategic planning in health care, based on lagging indicators like utilization rates and demographics, are no longer sufficient. Instead, leaders must increasingly look to external forces such as capital markets, regulatory volatility, and consumer behavior.
“Think outside-in,” he urges. “Forces outside health care are shaping its future more than forces within.”
He encourages health systems to go beyond isolated market studies and adopt holistic scenario planning that considers clinical innovation, workforce shifts, AI and tech disruption, and capital availability as interconnected variables.
Affordability and Accountability: The Hospital Reckoning
Keckley pulls no punches in addressing the mounting criticism of hospitals on Capitol Hill, particularly not-for-profit health systems. Public perception is faltering, with hospital pricing increasing faster than other categories in health care and only a third of providers in full compliance with price transparency rules.
“Economic uncertainty is not just about Wall Street. It’s about kitchen-table economics — how households decide between paying for care or paying the cable bill.”
“We have to get honest about trust, transparency, and affordability,” he says. “I’ve been in 11 system strategy sessions this year. Only one even mentioned affordability on their website, and none defined it.”
Keckley also predicts that popular regulatory targets like site-neutral payments, the 340B program, and nonprofit tax exemptions will face intensified scrutiny.
“Hospitals are no longer viewed as sacred institutions,” he says. “They’re being seen as part of the problem, especially by younger, more educated, and more skeptical Americans.”
The Consumer Awakens
Perhaps the most urgent shift Keckley outlines is the redefinition of the health care consumer. “We call them patients,” he says, “but they are consumers. And they are not happy.”
Keckley cites polling data showing that two out of three Americans believe the health care system needs to be rebuilt from the ground up. Roughly 40 percent of U.S. households have at least one unpaid medical bill, with many choosing intentionally not to pay. Among Gen Y and younger households, dissatisfaction is particularly acute.
“[Consumers] expect digital, personalized, seamless experiences — and they don’t understand why health care can’t deliver.”
These consumers aren’t just passive recipients of care; they’re voters, payers, and critics. With 14 percent of health care spending now coming directly from households, Keckley argues, health systems must engage consumers with the same sophistication that retail and tech companies use.
“They expect digital, personalized, seamless experiences — and they don’t understand why health care can’t deliver.”
Tech Disruption Is Real
Keckley underscores the transformative potential of AI and emerging clinical technologies, noting that in the next five years, more than 60 GLP-1-like therapeutic innovations could come to market. But the deeper disruption, he warns, is likely to come from outside the traditional industry.
Citing his own son’s work at Microsoft, Keckley envisions a future where a consumer’s smartphone, not a provider or insurer, is the true hub of health information. “Health care data will be consumer-controlled. That’s where this is headed.”
The takeaway for providers: Embrace data interoperability and consumer-centric technology now, or risk irrelevance. “The Amazons and Apples of the world are not waiting for CMS to set the rules,” Keckley says.
Capital, Consolidation, and Private Equity
Capital constraints and the shifting role of private equity also featured prominently in Keckley’s remarks. With declining non-operating revenue and shrinking federal dollars, some health systems increasingly rely on investor-backed funding.
But this comes with reputational and operational risks. While PE investments have been beneficial to shareholders, Keckley says, they’ve also produced “some pretty dire results for consumers” — particularly in post-acute care and physician practice consolidation.
“Policymakers are watching,” he says. “Expect legislation that will limit or redefine what private equity can do in health care.”
Politics and Optics: Navigating the Policy Minefield
In the regulatory arena, Keckley emphasizes that perception often matters more than substance. “Optics matter often more than the policy itself,” he says.
He cautions health leaders not to expect sweeping policy reform but to brace for “de jure chaos” as the current administration focuses on symbolic populist moves — cutting executive compensation, promoting price transparency, and attacking nonprofit tax exemptions.
With the 2026 midterm elections looming large, Keckley predicts a wave of executive orders and rhetorical grandstanding. But substantive policy change will be incremental and unpredictable.
“Don’t wait for a rescue from Washington. The future is going to be built by those who understand the consumer, embrace transparency, and adapt to the realities of a post-institutional world.”
The Workforce Crisis That Wasn’t Solved
Keckley also addresses the persistent shortage of health care workers and the failure of Title V of the ACA, which had promised to modernize the workforce through new team-based models. “Our guilds didn’t want it,” Keckley notes, bluntly. “So nothing happened.”
He argues that states, not the federal government, will drive the next chapter of workforce reform, expanding the scope of practice for pharmacists, nurse practitioners, and even lay caregivers, particularly in behavioral health and primary care.
What Should Leaders Do Now?
Keckley closed his keynote with a challenge for marketers and strategists: Get serious about defining affordability, understand capital markets, and stop defaulting to legacy assumptions.
“Don’t wait for a rescue from Washington,” he says. “The future is going to be built by those who understand the consumer, embrace transparency, and adapt to the realities of a post-institutional world.”
He encouraged leaders to monitor shifting federal org charts, track state-level policy moves, and scenario-plan for a future where trust, access, and consumer empowerment define success.
Conclusion: A Health Care Reckoning in the Making
Keckley’s keynote was more than a policy forecast; it was a wake-up call. In a landscape shaped by economic headwinds, political volatility, and consumer rebellion, health care leaders can no longer afford to stay in their lane. They must engage, adapt, and transform, or risk becoming casualties of a system under siege.
“Health care is not just one of 11 big industries,” Keckley says. “It’s the one that touches everyone. And right now, no one is giving us a standing ovation.”
This segment reviews preconditions for having a focused discussion of healthcare reform necessitated by powerful vested interests, and it discusses how to overcome political polarization.
In the first six Segments, we have reviewed the relentless growth of healthcare spending. And how rising costs are literally built into the system as it is now. This review should give us some ideas on how to fix the system.
But before we talk about how to fix the healthcare system, we must first tackle some landmines that lurk beneath the surface. The landmines are power, politics and philosophy. They are the subject of the next 2 Segments.
In this Segment, we will discuss both preconditions necessary for a calm, focused discussion of healthcare reform as well as what I call “loaded” political words. Then in the following Segment we will look at traditional American values and principles that can be brought to bear on resolving the core philosophical dilemma that has kept us from fixing US healthcare all these years.
Let’s start with preconditions. The idea here is that healthcare now comprises 1/6 of the entire US economy. So, there are powerful interests, lots of money, and fierce political convictions that could derail any discussion before it even gets started.
So, I suggest setting preconditions to be agreed on beforehand. Only then can we calmly get into the meat of the discussion. Here are the preconditions.
First, for purposes of discussion, let’s agree to keep dollar spending at the 2017 level – no winners, no losers, everything the same.
Second, let’s keep power the same. Keep the AMA, the hospital association, the VA, Health & Human Services, etc. No power struggles.
Third, strive to keep partisan politics out of the discussion. Make it a joint problem-solving project. Give credit where it’s due: to politicians or policy writers who contribute constructively. The motto is: “U.S. spells us.” Healthcare employs 1/6 of us and touches all of us.
Fourth, here’s where I will insert a viewpoint from my 40 years experience as a doctor: Human beings all get the same illnesses, all suffer, all are interconnected mind/body/spirits. I – like all doctors — have taken care of rich and poor, all races and nationalities, religious and non-religious, social outcasts and VIPs, saints and sinners. In a hospital bed or in the doctor’s office, we’re all the same. We should remember, “We’re all in this together”
Lastly, since healthcare is “too big to fail,” whatever is done should be done deliberately, slowly, with monitoring along the way and mid-course corrections when needed. If we accept these preconditions, we can have a Win-Win Discussion.
This kind of discussion should look at Facts, Goals, Values and lastly Methods, the actual Fix.
We have already discussed the Facts. The key facts are:
– the US health system has grown to 3.2 trillion dollars, representing 1/6 of the entire economy
– Cost growth is built into the system, has always outpaced inflation, and has resisted attempts to restrain the growth
– Healthcare spending is draining vitality from the economy, government and individual household budgets
Here are the key Goals:
– We must stop excess healthcare growth beyond the natural increase expected from population increase, aging, and innovation.
– To do so will require fundamental reform of the system, not just tinkering with public finance and private insurance
– Since healthcare is “too big to fail”, a key goal is Avoid short-term disruption, again proceed slowly.
The last things to discuss before we get to specific Methods – what I am calling the Fix of healthcare – are Politics and Values.
We all know that our country is polarized to an unhealthy extent. This has contributed to political paralysis – not getting anything done. I’m not a political scientist and cannot tackle the whole subject of healthcare politics.
But I do want to look at what I call “loaded words” that creep into our debates on healthcare. These words lock us into a closed, rigid mindset and can shut down discussion.
Let’s look at a few “loaded words” and suggest more neutral words to help keep the discussion open-minded.
First is “socialized medicine.” This terminology stirs up the negative connotations of the so-called “Prussian menace” after World War I and “Red scare” after World War II. A more neutral term would be “publicly financed medicine.” The truth of the matter is that currently almost 50% of healthcare is already publicly financed through Medicare, Medicaid and other government programs. The issues behind the loaded words, which do need thoughtful discussion, are accountability; and also advantages and disadvantages of uniformity and nationwide scale, instead of the current fragmented system.
The next loaded terms are “free market” and “competition.” The connotations are freedom from government interference, freedom from politics, consumer freedom, and efficiency. The grain of truth behind the terms is that the law of supply and demand does drive down prices to a balance point in pure markets. The reality, however, is that healthcare is not a pure market, as we saw in Segment 5. Also, markets sometimes leave aside consumers who are poor or powerless, which includes many of the sick. A more neutral term is commercial market.
Next is “rationing.” The connotation is forcibly withholding something from an individual. A more neutral term is “limit-setting” or “prioritizing.” We will talk more about this in the next Segment, and about the need for patients’ to consent to limits on their health service or health insurance. The reality is that we already have de facto rationing by zip code, income level, government budgeting, and hospital technology policies. Prioritizing is not bad – it’s necessary.
Another loaded word is “choice.” The connotation is that the government will interfere in choice of doctor or into the doctor-patient relationship itself. This was one of the scare tactics used by the insurance association in 1993 to bring down the President Clinton’s health reform plan. But the reality is that insurance network plans restrict patient choice of doctor more than government rules do. In addition, doctor inclusion in Medicaid – and other insurance plans, for that matter — is often a matter of the pay scales set by Medicaid or insurance companies, not the choices made by patients.
And the last loaded term I’ll mention is “big government.” The connotation goes back to President Reagan saying, “Government is not the solution to the problem; government is the problem.” We always hear about the Army’s 100-dollar toilet seats (in 1986 dollars) and the disastrous roll-out of the Obamacare website.
And the truth is that government is big and can be just as flawed as any big institution. However, national government, unlike private companies, is legally transparent and accountable. Also, Government can fulfill some functions more effectively and efficiently than some private sector piecemeal approaches. Here are examples: FAA, FDA, FCC. Currently the military enjoys a high regard. Some examples of public-private partnerships are the moon shot, internet and healthcare research. Medicare has an enviable customer satisfaction rating of 77%.
The reality is that we are now a nation (and world) of big institutions – for-profit, non-profit, government, academic. All have institutional governance and administrative challenges, which are studied by the disciplines of public administration and business administration. Public administration and business administration tell us how best to run big institutions so as to fulfill their mission and to remain accountable and transparent. More neutral terms instead of “big government” are: public sector programs or taxpayer-funded program.
So we have some better neutral terminology to use for discussing healthcare to avoid inflammatory polemical words.
In the next Segment we will look at American values at stake in health care. We will also look at what philosophers say is a fair way to run US healthcare.
Abstract: This article looks into the importance of selling in business and the relevance of the development of selling skills to career success regardless of your role in an organization.
Really? You’re not a salesman or saleswoman or salesperson? What are you then? Zig Ziglar and others argue that everyone is in selling whether he or she recognize or acknowledge it or not. I have come across people that say that they consciously and intentionally do not know anything about selling or that selling is below their station in life. Some of them have no idea that some of the best-compensated people in society achieve the success they enjoy from being successful in sales.
What is selling anyway? I would define selling as bringing someone else around to your way of thinking. The hoped result of the selling process is that the other party will decide to act upon your suggestions and recommendations (closing questions). Sometimes this results in a sale for value in which goods or services are exchanged. In other cases, you are selling a concept or ideas like a strategy or recommended course of action to a decision maker that must put their reputation and possibly their job on the line by committing to your proposed course of action.
When some people hear the term ‘salesman’ the image that pops up in their mind is the high-pressure wielding scoundrel at the ‘buy here, pay here, Se Habla Español’ used car dealership with the moussed hair, polyester leisure suit, braided leather suspenders, and patent leather platform shoes. The sales weasel is the offensive stereotype that ‘professionals’ avoid at all costs. However, the argument can be made that the scoundrel has a much easier way of making a living than those of us that make our living by selling ideas, concepts, and strategies into sophisticated organizations. He is not up against counterparties that in many cases are considerably more experienced, educated, credentialed or intelligent than he is. More often than not, the reverse is true.
If you would just as soon not be bothered with selling, my suggestion is that you dispense with aspirations of obtaining or staying in a C-Suite role.What is a C-Suite? One definition is that it is a marketplace of ideas. The environment is characterized by continuous, ongoing debate of concepts and strategies to move the organization forward or respond to problems and threats. If you are not effective in getting your ideas heard, debated and accepted, you might want to start thinking about finding another way to make a living. If you cannot successfully sell your fair share of ideas in what is usually a very intimidating, competitive and sometimes hostile environment, your perceived value will fall along with the probability of achieving your career ambitions.
What types of selling occur?Direct selling involves interactions with the intended purpose of an agreement to exchange goods or services for money. What I will refer to as professional selling is focused on winning in the marketplace of ideas. In other words, getting decision-makers to take your advice, respond to your counsel or choose a course of action based primarily upon your input. Professional selling is infinitely more difficult because it has a variable that is usually not present in direct selling – politics. The politics are carried out generally behind the scenes by competitors of yours that could be trusted co-workers that advocate for their ideas behind the scenes or behind your back, without giving you the courtesy or respect of a face-to-face argument. They use whatever leverage is available to them behind the scenes, under the table, and behind your back to advance their causes, frequently resulting in decisions that do not make rational sense. Suboptimal results occur because, in the presence of politics, decision making is usually irrational.
For example, I experienced a situation where some physicians were not happy with some of the decisions coming out of the boardroom and the front office. Do you know how many visits I had from any of the doctors? The answer is zero! Instead, they took their grievances directly to members of the board or county commission that humored and engaged them possibly in utter and absolute ignorance of the degree to which this amounted to the active undermining of the leadership team of the organization. I learned that one board member was accosted in the church vestibule and never made it into the sanctuary to join their family for the service. Others are caught at their places of work or during unrelated social events. As we are seeing in our society right now, people that are sufficiently strident about their position will resort to extreme means including violence to have their ideology imposed upon the rest of us. If you are in a board meeting and something entirely unexpected comes out of left field and derails something that you have put a lot of time and energy into, there is a good chance you are a victim of cowardly, destructive politics.
The stakes of success in a political environment are exponentially higher. If you are to be successful when you are up against political resistance, your arguments or the effectiveness of your selling must be sufficiently compelling to not only overcome the logical burden of your case but the political forces that may be working against you behind the scenes or maybe more accurately stated, behind your back. If this is not selling, I don’t know what is. Most of the time, to one degree or another, your career is potentially on the line when you are selling to your leader or a board of trustees. Must close selling puts you in an Apollo 13 situation where failure is not an option. I sold vacuum cleaners in college. I learned these concepts early on. In-home vacuum selling can be very intense, high-pressure selling. That said, selling vacuum cleaners is infinitely more comfortable than surviving in the shark tank that is the C-Suite of most organizations I have experienced. I guess that’s why good vacuum cleaner salesmen make around $50K and C-Suite roles pay into seven figures.
So, the obvious question is what you should be doing? My recommendation is that you start dedicating significant time and energy to learning as much as you can about selling. The quintessential sales trainer is Zig Ziglar. He is one of the best but not the only one. I would also recommend Harvey Mackay. Both of these guys are retired, but their work is as relevant as ever. Effective selling requires a healthy positive attitude. There are many excellent motivational speakers. Some of my favorites are Les Brown, Earl Nightingale, Dr. Angela Duckworth, Zig Ziglar, and Ed Foreman. Don’t overlook some of the incredible ministers that deliver messages of hope and inspiration. For starters, I recommend Charles Stanley, Johnny Hunt, Robert Schuller, and Joel Osteen. I have found that the more time I spend listening to these inspiring people, the luckier I become in the marketplace of ideas in a consulting firm, among my compadres, in a hospital C-Suite or down at the local watering hole.
Contact me to discuss any questions or observations you might have about these articles, leadership, transitions or interim services. I might have an idea or two that might be valuable to you. An observation from my experience is that we need better leadership at every level in organizations. Some of my feedback is coming from people that are demonstrating an interest in advancing their careers, and I am writing content to address those inquiries.
The easiest way to keep abreast of this blog is to become a follower. You will be notified of all updates as they occur. To become a follower, click the “Following” bubble that usually appears near the bottom of each web page.
I encourage you to use the comment section at the bottom of each article to provide feedback and stimulate discussion. I welcome input and feedback that will help me to improve the quality and relevance of this work.
This blog is original work. I claim copyright of this material with reproduction prohibited without attribution. I note and provide links to supporting documentation for non-original material. If you choose to link any of my articles, I’d appreciate notification.